


Technology Refines the Refractive Results of Cataract Surgery
Roberto Bellucci, MD, FEBOS-CR
Verona, Italy

The essential role of cataract surgery is to replace a cloudy crystalline lens with an artificial lens without damaging the remaining ocular anatomy. Technology that influences safety may therefore be considered essential. In contrast, the correction of preexisting astigmatism, presbyopia, and iris defects as well as the related technology used in these procedures may be considered complementary.
ESSENTIAL TECHNOLOGY
In my opinion, there are two basic essential technologies in the OR.
Forced infusion. When the infusion pressure is instantaneously regulated by input from the aspiration line, the risk of chamber collapse greatly decreases.1 With peristaltic pumps, the flow rate is monitored and used to increase or decrease the irrigation pressure, and pressure sensors regulate the system during occlusion when there is no flow (Figure 1). With vacuum pumps, the infusion pressure increases as the vacuum level increases, completely preventing chamber collapse on disocclusion (Figure 2).
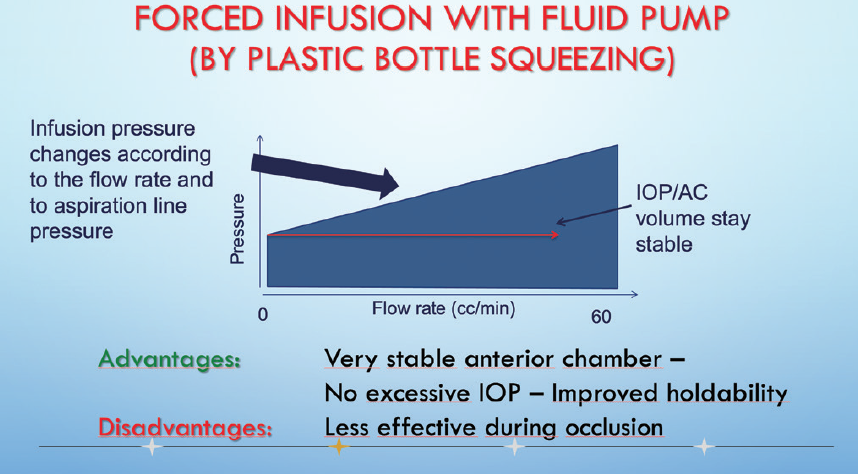
Figure 1. With a fluid pump, infusion pressure is regulated by fluid and by pressure sensors.
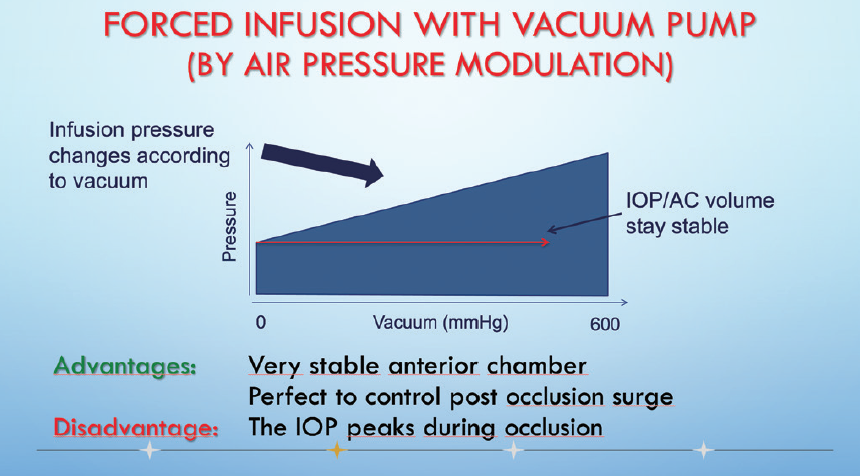
Figure 2. With vacuum pumps, infusion pressure is regulated by vacuum sensors.
Figures 1 and 2 courtesy of Roberto Bellucci, MD
Forced infusion represents a significant step forward in phaco technology.2 It has improved the safety of surgery with either type of pump and facilitated the teaching of cataract surgery.
Injectors. The safety of cataract surgery also depends on the ophthalmologist’s ability to insert a 6-mm IOL through a narrow 2.2-mm incision, which is essential to avoid inducing astigmatism. When surgeons implant an IOL, they rarely think about what a nice piece of engineering the injector is.
It is essential to use an injector designed for the chosen IOL implant. Recently released injectors with preloaded IOLs eliminate the need for IOL manipulation, a step that when required can decrease safety—either mechanical or in terms of infection. Although not every IOL is currently available as a preloaded model, I expect this to become standard in a few years.
COMPLEMENTARY TECHNOLOGY
Complementary technologies that represent surgical refinements are outlined herein.
Femtosecond laser. I started using a femtosecond laser during cataract surgery in 2012, and laser cataract surgery has been my go-to approach since then. I use a femtosecond laser to perform the capsulotomy, fragment the lens, create the main and sideport incisions, mark the capsule for a toric IOL, and create arcuate incisions. I have not encountered a laser-induced complication thus far.
I like this technology and will continue to use it, but I consider femtosecond lasers to be essential only for an eye with a very shallow anterior chamber or a white cataract. The same is true of other devices designed to create a mechanical capsulotomy; these technologies cost much less but are not yet widely accepted.3
Intraoperative aberrometers and image guidance. Intraoperative aberrometry fascinated me a few years ago, but the necessity of dedicating one surgical microscope to this purpose prevented me from implementing the technology in my practice. Fortunately, recent improvements in IOL calculation formulas have reduced refractive surprises even in post-LASIK eyes.
For a toric IOL, I mark the cornea at 0º and 180º before surgery. Then, as noted earlier, I mark the alignment axis with a femtosecond laser. Alternatively, image-guidance systems can be attached to the surgical microscope. They allow IOL alignment based on a preoperative image without corneal marking. These systems were found to be more precise than more standard technologies in studies published by Elhofi3 in 2015 and by Webers4 and Mayer5 in 2017. In these studies, the mean misalignment was 1.7º to 2.4º with an image-guided approach and 3.1º to 4.3º with a manual marking method.
CONCLUSION
The routine use of complementary technology refines the refractive results of cataract surgery and improves UCVA. Its implementation is worthwhile for refractive cataract surgery and refractive lens exchange.
1. Nicoli CM, Dimalanta R, Miller KM. Experimental anterior chamber maintenance in active versus passive phacoemulsification fluidics systems. J Cataract Refract Surg. 2016;42(1):157-162.
2. Jensen JD, Boulter T, Lambert NG, et al. Intraocular pressure study using monitored forced-infusion system phacoemulsification technology. J Cataract Refract Surg. 2016;42(5):768-771.
3. Elhofi AH, Helaly HA. Comparison between digital and manual marking for toric intraocular lenses: a randomized trial. Medicine (Baltimore). 2015;94(38):e1618.
4. Webers VSC, Bauer NJC, Visser N, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg. 2017;43(6):781-788.
5. Mayer WJ, Kreutzer T, Dirisamer M, Kern C, Kortuem K, Vounotrypidis E, Priglinger S, Kook D. Comparison of visual outcomes, alignment accuracy, and surgical time between 2 methods of corneal marking for toric intraocular lens implantation. J Cataract Refract Surg. 2017;43(10):1281-1286.
The Best Technologies for Subluxated Cataracts
Sergio Canabrava, MD
Belo Horizonte, Brazil

Subluxated cataracts present several surgical challenges. In particular, secondary lens dislocation is a common occurrence after IOL implantation. A variety of methods and devices have been described for stabilizing the IOL–capsular bag complex in eyes with zonular weakness. Based on my surgical experience with more than 100 eyes with subluxated cataracts, the most useful essential and the complementary technologies are the femtosecond laser, capsular tension rings (CTRs), and segments (CTSs), capsular hooks, sutures, triamcinolone acetonide, and the vitreophagus tip.
ESSENTIAL TECHNOLOGIES
I could not successfully complete surgery on an eye with a subluxated cataract without the following technologies.
Femtosecond laser. One of the most challenging surgical steps in eyes with subluxated cataracts is the capsulorhexis. Puncturing and tearing the anterior capsule can become difficult when zonular countertraction is compromised. I prefer to use a femtosecond laser for this step of the procedure (Figure 3) because it does not depend on zonular support to create a capsulotomy and therefore avoids putting traction on the zonules. This is especially helpful in the presence of lens subluxation.
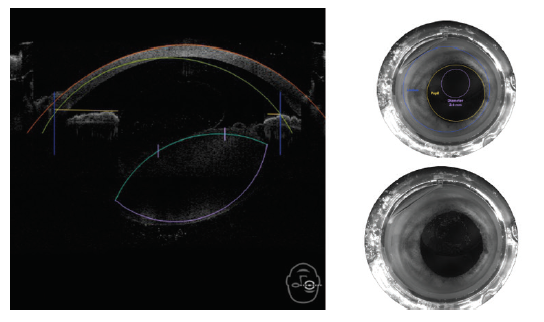
Figure 3. The femtosecond laser is one way to effectively perform an anterior capsulotomy.
Courtesy of Sergio Canabrava, MD
I consider the femtosecond laser to be the most essential technology developed in the past 10 years for avoiding complications in eyes with subluxated cataracts. The laser software of the Catalys (Johnson & Johnson Vision) allows me to reposition the capsulotomy and decrease its size manually. Thus, even in eyes with severely subluxated lenses, a perfect capsulotomy can be created.
Traditional CTRs. I like to insert a traditional CTR inside the capsular bag before phacoemulsification. This device redistributes the capsular forces, expands the fornices, and decreases the flaccidity of the posterior capsule.
Capsular hooks. In addition to a CTR, in some cases, I will place capsular hooks to further stabilize the capsular bag during phacoemulsification.
CTS. Another helpful tool is a CTS, which is inserted in the area of most fragility in the sclera. This device is fixated to the subluxated capsular bag.
Suture. A basic tool required during lens–capsular bag fixation is sutures. Polypropylene 10-0 hydrolyzes over time and has only a 5- to 10-year survival time, resulting in pseudophacodonesis and late IOL decentration. I therefore prefer to use either a PTFE suture (Gore-Tex, W.L. Gore Medical, off-label use) or a 5-0 polypropylene suture (Prolene, Ethicon) with my own personal double-flanged technique. In this Canabrava technique, a 5-0 polypropylene suture is externalized through the sclera and heated into a first flange. Next, a second flange is created and inserted into the scleral tunnel (see Watch It Now).
WATCH IT NOW
Dr. Canabrava demonstrates his technique for lens–capsular bag fixation of an IOL.
COMPLEMENTARY TECHNOLOGIES
The following complementary technologies aid in the successful completion of surgery in eyes with a subluxated cataract.
Triamcinolone acetonide. An injection of triamcinolone acetonide is useful for identifying vitreous in the anterior chamber.
Vitreophagus tip. This device is useful when a posterior capsular rupture occurs. Compared with other devices, it more easily avoids vitreous traction in my experience.
CONCLUSION
Regardless of whether technologies are essential or complementary, all to me are requirements to achieve excellent surgical results. Certain technologies will surely be added to this list as new devices and techniques are discovered, but for now those mentioned here are my go-tos for surgery in eyes with subluxated cataracts.
1. Canabrava S, Canedo Domingos Lima AC, Arancibia AEL, Bicalho Dornelas LF, Ribeiro G. Novel double-flanged technique for managing Marfan syndrome and microspherophakia. J Cataract Refract Surg. 2020;46(3):333-339.
2. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31:1320-1326.
3. Hoffman RS, Snyder ME, Devgan U, Allen QB, Yeoh R, Braga-Mele R, ASCRS Cataract Clinical Committee; Challenging/Complicated Cataract Surgery Subcommittee. Management of the subluxated crystalline lens. J Cataract Refract Surg. 2013;39:1904-1915.
Improvements to Workflow Are Essential
Oliver Findl, MD, MBA
Vienna, Austria

As tired as we may be of discussing COVID-19, we can all agree that increasing workflow efficiency is more crucial now than ever before. Some technologies are essential, and others are complementary to this mission. All, however, work together to help ensure maximal reliability, safety, and efficiency.
ESSENTIAL COMPONENTS
The following are two examples of technologies that are essential components of my cataract surgery workflow.
Electronic health records. I use electronic health record (EHR) software, from the company Lobmaier, that is available only in Austria. I need an EHR system that’s extremely stable, and I find this system to be both reliable and easy to use.
Biometry. One enhancement in biometry that I am using with increased frequency is the Zeiss EQ Workplace (Carl Zeiss Meditec). This digital surgical planning tool works with the company’s Forum software to compile all preoperative biometric data on the cloud (Figure 4). It also allows me to order an IOL of the appropriate power via an automatically generated email to my IOL supplier. When I enter the OR, I simply open the EQ mobile app on my phone (Figure 5) and download the data obtained from the IOLMaster 700 into the OPMI Lumera operating microscope (both from Carl Zeiss Meditec). It’s a seamless process that works well for me.
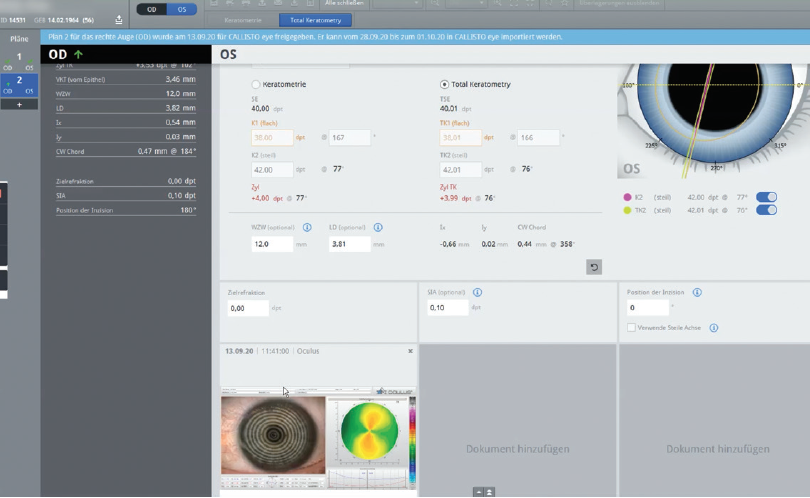
Figure 4. Sample screen of the EQ Workplace digital surgical planning tool.

Figure 5. Sample screen of the EQ mobile app.
Figures 4 and 5 courtesy of Oliver Findl, MD, MBA
COMPLEMENTARY COMPONENTS
Two complementary technologies in particular are useful to my practice.
Slit-lamp images. I show patients slit-lamp photographs of their cataracts on a big-screen TV so that they can see what is happening inside their eyes. Patients seem to like this; they have been to the optometrist or visited one or two other eye doctors before, but most have never seen their cataracts. This image is a powerful tool for patient education.
Animated educational material. The use of animated educational material also enhances efficiency. In our hospital, before patients are seen by the surgeon, they watch a video on an iPad that walks them through the entire cataract surgery procedure. The video shows them what a cataract is; describes what happens before, during, and after surgery; and provides an overview of the risks and complications associated with surgery. The video is broken into eight chapters. At the end of each chapter, patients have three options: watch the chapter again, continue to the next chapter, or ask a question about the content of the chapter. The surgeon receives a printout of the responses so that unanswered questions can be addressed with patients.
CONCLUSION
I use a variety of other essential and complementary technologies on a daily basis, but these four are particularly worth noting because they have helped to enhance our efficiency. We always welcome such enhancements, but they are especially valuable in the time of COVID-19.
Improving Patient Care and Practice Efficiency
Maria S. Romero, MD
Maryland, United States

When deciding which technologies to purchase for my practice, I ask myself three questions:
No. 1. Will it improve quality of care (ie, outcomes)?
No. 2. Will it increase practice efficiency by saving time, decreasing the chance of errors, or reducing staff requirements?
No. 3. Does it make financial sense for my practice?
This article describes several technologies that have made the cut.
ESSENTIAL
OCT. I find the Cirrus HD-OCT 5000/500 (Carl Zeiss Meditec) to be invaluable for the analysis of ocular structures, particularly OCT scans of the macula as part of the cataract evaluation (Figure 6).1 Further, I continue to rely on the IOLMaster 700 for central topography and IOL power calculation.
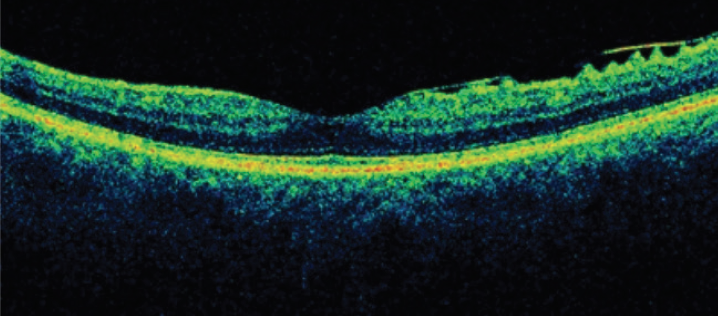
Figure 6. Spectral-domain OCT of the macula showing an epiretinal membrane.
Courtesy of Maria S. Romero, MD
Ray tracing. I recently acquired an iTrace (Tracey Technologies). I now use this technology in the examination of all of my patients, whether they are undergoing a contact lens fitting or a cataract evaluation because it assesses their full visual function. The iTrace is five devices in one: an autorefractometer, wavefront aberrometer, keratometer, corneal topographer, and pupillometer. I find this unit to be an excellent tool for educating patients, because it has a display that graphically simulates vision with and without correction. Moreover, the visual function breakdown includes the dysfunctional lens index versus high corneal aberration. The company plans to release diagnostic software for dry eye disease for the iTrace later this year.
COMPLEMENTARY
Images. EyePhotoDoc International offers slit-lamp photography systems that are compatible with iPads and iPhones. These devices attach to the slit lamp, and external photographs can be uploaded directly to an EHR system. The display also facilitates patient education. In my experience, this technology is especially helpful when explaining ocular surface disease to patients.
I also find the CheckedUp Explorer Waiting Room TV and CheckedUp Consult Digital Exam Room Wallboard (both from CheckedUp) to be helpful. The image-based presentations these technologies deliver improve my patients’ understanding of their disease states.
Workflow aids. A tool that has improved workflow at my office is uArrive (OTech Group). This technology allows patients to check themselves in for their appointments at a kiosk or on a tablet. It also collects copays and balances, scans IDs and insurance cards, updates demographics, verifies insurance and eligibility, and provides e-signature requests for admission forms. OTech’s uSign allows patients to read, complete, and sign forms electronically and then saves these forms in an EHR system. Both tools decrease my front desk staff’s workload and facilitate a paperless office.
1. Romero MS. The Role of SD-OCT in the preoperative evaluation of cataract surgery. Paper presented at: 2020 ASCRS Virtual Annual Meeting; May 16-17, 2020.
Preferences and Technologies Evolve With Time
Martín Sierra Meyer, MD
Montevideo, Uruguay

Which technologies are considered essential and which are complementary evolves over time. When an older colleague of mine began performing ophthalmic surgery, loupes were essential, whereas I currently require a surgical microscope.
ESSENTIAL TECHNOLOGY
To my mind, the most essential technology for ophthalmic surgery is an aspiration cannula. The earliest known iteration of this instrument dates to the 11th century, when its use by Ammar ibn Ali Mawsili in Cairo, Egypt, was recorded.1,2 Device development for cataract surgery really took hold in the 1960s.2
I practice medicine in Rivera, a small city in northern Uruguay along the border with Brazil that has a population of 90,000 inhabitants. Some of the rural areas where I operate do not have phaco machines with pump aspiration. Instead, I use a handmade device and anterior chamber maintainer. The device combines an aspiration cannula, an extender for a syringe perfusion pump, a three-way stopcock, and a manual driving force using a 10-mL syringe (Figure 7).
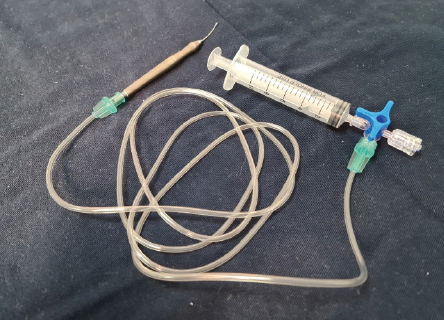
Figure 7. A handmade device for phacoemulsification that Dr. Sierra Meyer uses with an anterior chamber maintainer. The device consists of an aspiration cannula, an extender for a syringe perfusion pump, a three-way stopcock, and a manual driving force using a 10-mL syringe.
Courtesy of Martín Sierra Meyer, MD
COMPLEMENTARY TECHNOLOGY
The vitrector is my top choice of a complementary technology. High cutting rates reduce traction on the retina, which makes tears less likely. High cutting rates also result in smaller bites of vitreous, which create fewer shearing forces and improve flow.3
Although vitrectomy can be performed with scissors and sponges, a vitrector facilitates the removal of vitreous from the anterior chamber and decreases the possibility that a strand of vitreous will be incarcerated in the cataract incision, potentially putting traction on the retina.
1. Pérez-Cambrodí RJ, Ascaso FJ, Diab F, Alzamora-Rodríguez A, Grzybowski A. Hollow needle cataract aspiration in antiquity. Acta Ophthalmol. 2015;93(8):782-784.
2. Leffler CT, Letocha CE, Pierson K, Schwartz SG. Aspiration of cataract in 1815 in Philadelphia, Pennsylvania. Digit J Ophthalmol. 2017;23(4):4-7.
3. Nagpal M, Goswami S. Micro-incision vitrectomy surgery – past, present and future. European Ophthalmic Review. 2015;9(1):64-68.
Both Kinds of Technology Can Help to Optimize Outcomes
Ronald Yeoh, FRCS, FRCOphth, DO, FAMS
Singapore

Precise refractive outcomes are the desired target of all cataract surgeons, but the process of obtaining them involves many variables. Ophthalmologists with well-developed surgical techniques can enhance their surgical outcomes with many technologies, including those discussed herein.
BIOMETRY AND IOL CALCULATIONS
I consider an optical swept-source biometer to be an essential technology. My preferred device is the IOLMaster 700, which measures axial length, keratometry (K), lens thickness, white-to-white, and posterior corneal astigmatism. The last is important for biometry performed on eyes with a history of refractive surgery. I value this device’s ability to image the foveal pit because it confirms that the axial length has been accurately acquired.
As a refractive cataract surgeon, I target zero postoperative astigmatism. Most (75%) of my cataract patients receive a monofocal or multifocal toric IOL. Eliminating astigmatism requires using one of the latest generation of IOL formulas to crunch the data obtained with the IOLMaster 700. My favorite is the Barrett Toric Calculator, which is available for free at www.apacrs.org and other websites.
The most challenging variable is often the K reading because values often differ between machines. The integrated K calculator on the Barrett Toric Calculator allows me to enter three sets of K readings to generate the optimal toric power and axis for the IOL. These extra K values can be obtained from complementary devices such as autokeratometers and aberrometers. Combining these data with the latest generation of IOL formulas is the best strategy for achieving precise refractive outcomes regardless of whether a monofocal or a trifocal IOL is used.
OPERATING MICROSCOPE
A second essential technology is the operating microscope. Without it, I would not be able to perform cataract surgery at a level that permits me to take advantage of precise biometry. Most modern microscopes allow excellent visualization of all parts of the anterior segment, but two recent complementary technologies deserve mention.
Intraoperative digital toric alignment. The Callisto system (Carl Zeiss Meditec) on the OPMI Lumera 700 allows highly precise alignment of a toric IOL using data from the IOLMaster 700.
Intraoperative OCT. This technology is available on microscopes manufactured by both Leica Microsystems and Carl Zeiss Meditec. Interestingly, intraoperative OCT was designed to assist with epiretinal membrane peeling and with lamellar corneal surgery. Its use in cataract surgery, however, has been a revelation. Intraoperative OCT helps surgeons to understand and appreciate the anatomy of cataract surgery (Figures 8–10).
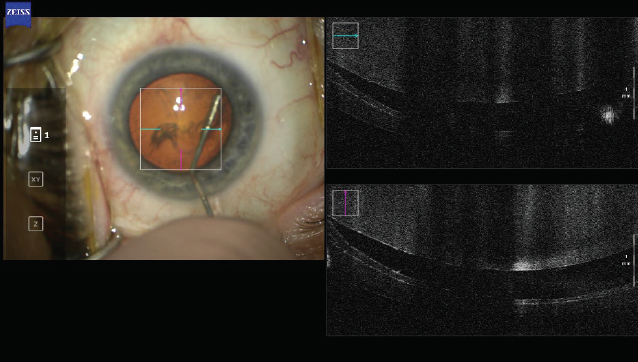
Figure 8. The fluid wave frees the nucleus during hydrodissection.
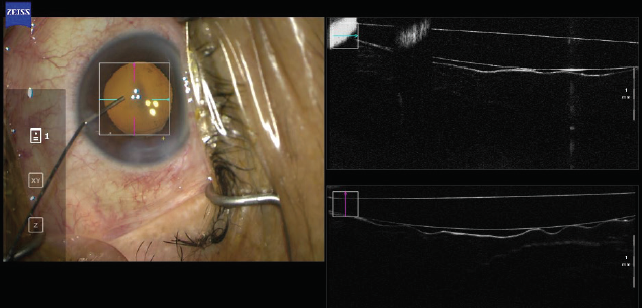
Figure 9. Removing the OVD from behind the IOL resulted in close contact between the IOL and the posterior capsule.
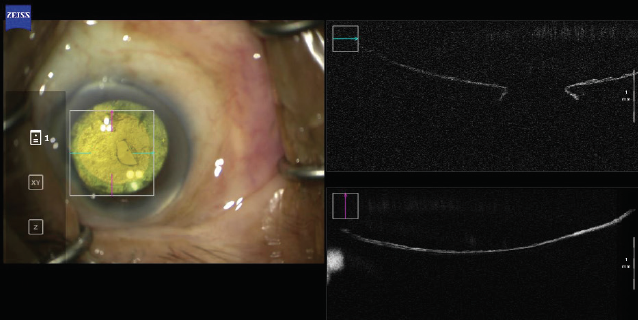
Figure 10. A cross-section of a ruptured posterior capsular.
Figures 8–10 courtesy of Ronald Yeoh, FRCS, FRCOphth, DO, FAMS
CONCLUSION
Cataract surgeons are only as good as technology allows them to be. The aforementioned essential and complementary technologies enable me to deliver better outcomes to my patients.
