


The Outlook Will Be Brighter After Availability of a Vaccine
Ahmed Assaf, MD, PhD, FRCS(Ed)
Cairo, Egypt

The COVID-19 pandemic has made patients extremely hesitant to seek elective health care, including cataract and refractive surgery. Surgical volume at my practice has declined dramatically. In the second half of March 2020, I performed 25% fewer surgical procedures than during the same period in 2019 (Figure 1), and the number of patients seen in clinic dropped by about 50%.
In April, the number of patients in my private clinic declined by more than 75%. Most presenting for care required IOP monitoring or treatment for conditions such as acute viral conjunctivitis, corneal ulcers, acute uveitis, and retinal detachment.
We implemented the highest safety measures for the sake of our patients and our staff. For example, we mandated that patients must wear masks and may be accompanied by only one companion, we reduced the number of bookings per session to three patients, and we reduced our working days from 5 to 2 per week.
Surgical volume in April 2020 was approximately 68% of that in April 2019 (Figure 1).
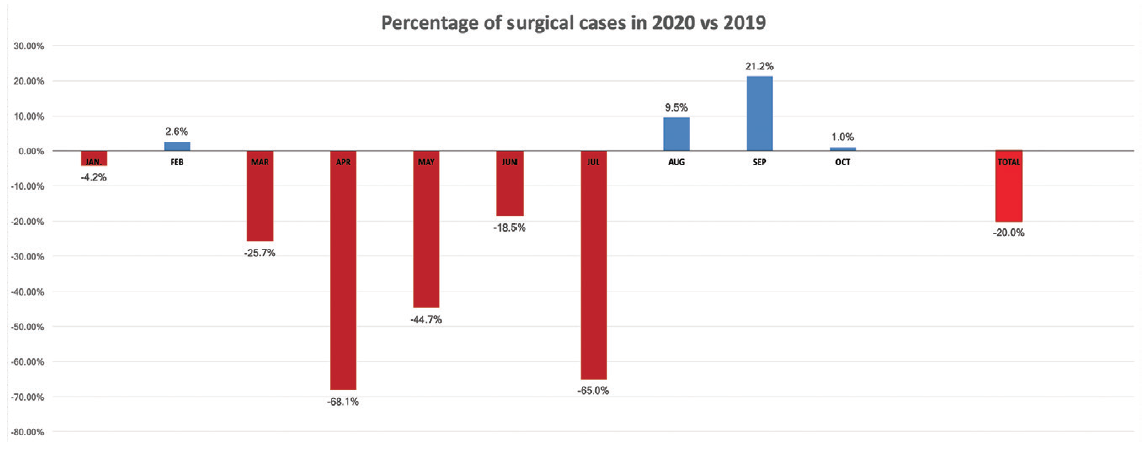
Figure 1. Percentage of surgical cases Dr. Assaf performed in 2020 compared with 2019.
Courtesy of Ahmed Assaf, MD, PhD, FRCS(Ed)
This reduction had a massive impact on monthly income, particularly because we did not implement a payroll reduction strategy for clinic employees.
A SUMMERTIME LIFT
Eased restrictions and a decrease in COVID-19 cases increased patient interest in cataract surgery and LASIK during May and June 2020, but volume was still lower compared to the same time period in 2019. In July 2020, surgical volume dipped again, perhaps owing to patients’ changing priorities. People in the community were restless after having to endure several weeks of lockdown, and going to the beach and enjoying leisure activities seemed to take precedence over cataract and refractive surgery.
Our practice experienced a slight rebound in August and September 2020. The total number of surgical procedures increased by 9.5% and 21%, respectively, compared to 2019. In other words, the peak number of surgeries shifted from early and mid-summer to late summer and autumn.
WINTER OUTLOOK
This winter, the number of elective surgeries is declining similarly to the same period in the previous year. We expect the decline to continue as the second wave of COVID-19 hits, but we are hopeful that the outlook in 2021 will be brighter after a vaccine becomes available.
A Huge Backlog, a Rise in Demand
Ali A. Mearza, MBBS, FRCOphth
London, United Kingdom

When the COVID-19 pandemic struck in early 2020, our practice was forced to close as part of the UK national lockdown. Like many other private health care organizations, ours faced an uncertain future. With ongoing business costs, it was hard to see how our practice would survive unless patients had confidence that they could visit our practice and receive treatment safely when the lockdown was lifted.
Our physicians and staff used the downtime to prepare for a world that would be very different from the one we were used to. We implemented appropriate protective measures in our clinics, streamlined all our processes, and updated our website with relevant information. After the lockdown ended, we used social media channels to announce that our practice was open and ready to help and that appropriate safety measures were in place. Thanks to our actions during the lockdown, our current outlook is bright.
A SURGE IN DEMAND
Once our practice reopened, demand surged across all our specialty areas. We believe this was directly related to the fact that the pandemic forced the UK’s National Health Service (NHS) to cancel thousands of nonessential operations, including cataract surgery and other eye procedures. Waiting lists were already long, but these cancellations created a huge backlog.
According to data from NHS England, in August 2020, more than 111,000 patients who had been referred for hospital treatment were still waiting to be seen—the highest level in 12 years. Among those awaiting eye surgery, barely two of five (41.8%) were seen within the NHS’s target of 18 weeks from referral.1
The demand for private treatment at our clinic was strongest among cataract patients. Between July and September 2020, we performed 47.1% more cataract operations than we did during the same period of the previous year. This is an incredible jump. Although cataract surgery is available through the NHS, waiting times vary widely by region, and they have been significantly extended by the extra demands placed on hospitals by the pandemic.
The number of patients being treated at our central London clinic (Figure 2) has increased by 34.8% overall compared to this time last year. We have also seen increases in the volume of many of the other procedures that we perform. This uptick seems to be holding steady despite a second wave in COVID-19 cases. The United Kingdom entered into a second national lockdown in November 2020, but at the time of this writing all health care facilities have been allowed to stay open. This is important because it means private organizations can help with the backlog of cases created by a lack of capacity within the NHS.

Figure 2. The flagship location of Ophthalmic Consultants of London.
Courtesy of Ali A. Mearza, MBBS, FRCOphth
PARTNERS, NOT COMPETITORS
We consider ourselves to be a complement rather than a competitor to the NHS, and that has never been truer than it is now. Approximately 10% of UK residents have private medical insurance, and an additional 5% choose to pay for private treatment themselves. The private sector is providing vital backup to the NHS while it must prioritize its resources to tackle a second wave of COVID-19 cases.
With millions of Britons once again living under lockdown conditions at the time of this writing, it is interesting that many baby boomers—the demographic most affected by cataracts—are choosing to spend money they might have spent on a holiday this year on their eyesight instead. One reason may be that wearing a mask can lead to foggy spectacle lenses. This may also account for increases in vision correction surgeries (laser vision correction and refractive lens exchange) and in the uptake of technology that reduces patient dependence on glasses (eg, multifocal IOLs).
CONCLUSION
At the outset of the COVID-19 pandemic, we worried what the future might hold, but preparation has helped our practice to be busier than ever. We drew on our firm foundation, teamwork ethic, strong clinical leadership, and operational expertise to see us through and to deliver exceptional, timely, and safe care to our patients.
1. NHS England. Statistical press notice: NHS referral to treatment (RTT) waiting times data August 2020. Published October 8, 2020. Accessed November 17, 2020. https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2020/10/Aug20-RTT-SPN-publication-version-1.pdf
Net Increase in Surgical Volume Points to a Solid Year to Come
Evan D. Schoenberg, MD
Atlanta, United States

In my practice, cataract surgical volume returned to near pre-COVID levels within a few weeks of reopening. Our first full month of regular operation was June 2020, and, at that time, we were down 10% year-over-year in case volume. Every month since July 2020, we have seen a net increase in cataract and refractive surgery volume year-over-year. If the increase is sustained, 2021 could be our best year yet.
Changes in Surgical Volume and Procedures in Italy Because of COVID-19
Daniele Tognetto, MD; Alex Lucia Vinciguerra, MD; and Rosa Giglio, MD
Trieste, Italy



COVID-19 has profoundly affected the delivery of elective health services. Ophthalmology has registered a bigger reduction in patient volume than other specialties. Up to a 97% decrease in the number of cataract procedures during the early phase of this pandemic compared to the same period of 2019 was reported.1,2
REOPENING
At our hospital, a tertiary referral center in Northeast Italy, all nonurgent procedures were suspended during the first spike of COVID-19 cases in mid-March 2020. As the number of cases fell in late May, we developed a reopening plan that included reduced schedules for visits and surgeries to maintain social distancing and strict sanitization and aeration of the working areas.
The day before a scheduled visit or procedure, patients responded to a telephone questionnaire to flag warning symptoms (eg, fever, cough, and loss of smell and taste). If symptoms were reported, appointments were rescheduled, and patients were encouraged to contact their family doctor or the regional health authority. We also introduced triage procedures (eg, handwashing, surgical mask provision, body temperature measurement) upon patients’ arrival at the hospital. When patients such as minors and those with special needs required companions, caregivers followed these measures as well.
All patients scheduled for surgery underwent a nasopharyngeal swab for the qualitative detection of nucleic acid from SARS-CoV-2 (reverse transcription polymerase chain reaction test) 24 to 72 hours before entering the OR. Periodic SARS-CoV-2 screenings were arranged for the staff as well.
A SECOND SHUTDOWN
In November 2020, the Italian government enacted new restrictive measures in response to a second wave of cases. At the time of this writing, elective surgical procedures have been postponed again, which will affect our ability to meet the demand going forward. Moreover, delaying the treatment of patients with some nonurgent ophthalmic diseases for weeks to months may ultimately have sight-threatening consequences.
Patients’ quality of life and psychological well-being may be negatively affected in the long term, and costs to the health care system may increase.3,4 It is clear that the term elective is misleading because, in many cases, elective procedures profoundly influence patients’ health and quality of life.5 This issue will be clearly evident for the next few years.
conclusion
Because we expect an increased volume of patients who require care when the hospital reopens, we are trying to develop new strategic approaches to address the burden of vision loss. We are also acting to outline priority criteria for patients in need of ocular procedures that have been suspended during this pandemic.
1. Toro MD, Brézin AP, Burdon M, et al. Early impact of COVID-19 outbreak on eye care: insights from EUROCOVCAT group. Eur J Ophthalmol. September 24, 2020. doi:10.1177/1120672120960339
2. Strata Decision Technology. Analysis: ophthalmology lost more patient volume due to COVID-19 than any other specialty. Eyewire News. Accessed December 7, 2020. https://eyewire.news/articles/analysis-55-percent-fewer-americans-sought-hospital-care-in-march-april-due-to-covid-19
3. Amedo AO, Koomson NY, Pascal TM, Kumah DB. Quality of life of cataract patients before and after surgery-evidence from four rural communities in Ghana. Mathews J Ophthalmol. 2016;1(1):3.
4. Wang W, Yan W, Fotis K, et al. Cataract surgical rate and socioeconomics: a global study. Invest Ophthalmol Vis Sci. 2016;57(14):5872-5881.
5. Meredith JW, High KP, Freischlag JA. Preserving elective surgeries in the COVID-19 pandemic and the future. October 5, 2020. JAMA. doi:10.1001/jama.2020.19594
