


A Variety of Rules and Requirements for This Growing Trend in Surgical Care
Ahmet Akman, MD, FACS
Ankara, Turkey

Office-based surgery (OBS) is an emerging trend, and a recent study supports its safety.1 Nearly all ophthalmic surgical procedures can be performed in an office setting, but cataract surgery is the main focus of many practices. Different countries have different rules or requirements for performing surgical procedures in an office setting, and OBS means different settings in different countries. In Turkey, OBS is performed in the setting of a small eye center.
WHERE SURGERY IS PERFORMED
In Turkey, eye surgery may be performed at several locations. Currently, approximately 45% of cataract procedures are performed at multidisciplinary university and government hospitals that have ophthalmology departments. The remaining 55% are performed mainly at private chain and independent eye hospitals. Some small eye centers meet the legal requirements for offering eye surgery in an office setting. The social security system and private insurers do not discriminate among these settings in terms of reimbursement.
Big eye hospital chains are the main competitors of the small ophthalmology centers. Because the practice of ophthalmology requires expensive equipment, it is sometimes difficult for small centers to compete with the economic power of eye hospitals for purchasing the latest technology. Because of the ease of decision-making at the management level, however, both small centers and eye hospitals tend to have newer technology than general hospitals.
For patients, more advanced technology and the ease of scheduling surgery are the main advantages of seeking care at eye hospitals and centers. At most of these facilities, patients are offered cataract surgery immediately after their eyes are examined. Although convenient, this approach sometimes means that patients are not making informed decisions or getting second opinions. Further, strong competition means that these facilities use advertising and business tactics to increase surgical volume, sometimes unethically.
Because eye hospitals and eye centers do not have a hospital license, they are required to employ an anesthesiologist and to have an ambulance ready to transfer patients to a general hospital if a systemic complication occurs during ocular surgery.
CONCLUSION
Office-based eye surgery is common in Turkey. A high volume of cataract surgery is performed at some of the small centers. Because current regulations limit the number of private centers that may be opened in a certain province, their main competitors—chain eye hospitals—are bidding on most of these centers for growth. Future mergers appear likely. Some of these centers are branding their names, and franchise options are becoming available.
1. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21,000 cases in the United States. Ophthalmology. 2016;123(4):723-728.
Office-Based Cataract Surgery Is the Next Chapter
Young H. Choi, JD, MD
Alabama, United States

It was not that long ago in the United States that cataract surgery was performed only in a hospital setting. Today, however, it is mainly performed in an ambulatory surgery center (ASC). Will practice patterns shift once again, this time to an office setting? In my opinion, the answer to this question is yes.
The first word that comes to mind when I think about office-based cataract surgery (OBCS) is safety. In an analysis of more than 21,000 OBCS cases conducted by Kaiser Permanente Colorado, the rate of ocular adverse events was comparable if not favorable to cataract surgery performed in ASCs and hospital outpatient department (HOPD) settings. Moreover, there was not a single case of endophthalmitis in that study.1 The safety of OBCS is excellent.
PERSONAL EXPERIENCE
I have been performing OBCS for about 3 years (Figure 1), but I continue to operate at a local ASC once a week. In the COVID-19 era, social distancing is a key factor in patient safety, and in my opinion, this is more challenging to achieve in an ASC setting than in an office setting. I perform cataract surgery in three different rooms during my block time at the ASC.

Figure 1. Dr. Choi performs cataract surgery in his office.
Courtesy of Young H. Choi, JD, MD
In contrast, in the OBCS workflow, patients wait in their vehicles until they are called, immediately enter an exam room, and then are taken straight into the operating suite. At the end of a case, my OR staff calls the patient’s driver, who brings the vehicle to the front of the building. The patient is ushered out of the practice without ever encountering another patient.
Given their age, some cataract surgery patients will not go to an HOPD or an ASC during this pandemic, but many will come to our practice for OBCS because of the social-distancing measures we have put in place to keep them—and our staff—safe. My OBCS patients have been extremely grateful for and appreciative of our efforts.
CLEAR ADVANTAGES
In my experience, OBCS has clear advantages over cataract surgery performed in an ASC or an HOPD.
Sedation. Oral sedation is enough to keep most cataract surgery patients comfortable during surgery. In the Kaiser study, more than 95% of patients did not require IV sedation.1 This has also been my experience in the past 3 years; 100% of my patients have done fine without IV sedation. Patients, especially those with diabetes, appreciate being able to eat and drink before surgery.
Workflow. OBCS provides a more fluid workflow. I can see clinic patients and perform OBCS seamlessly throughout the day. I start my day performing cataract surgery while my staff completes workups on patients in the clinic. After each surgery, I see patients in the clinic while my OR staff prepares the next patient for surgery. For me, this movement between the OR and the clinic is more enjoyable than when I am at the ASC to perform cataract surgery.
DRAWBACKS
The main drawback to OBCS is that most insurance carriers neither reimburse for a facility fee nor offer an enhanced profession fee. This, however, is rapidly changing. OBCS is a relatively novel concept to most insurance carriers, and time is required to adopt new reimbursement schemes.
In my area, three private insurance companies have recognized the benefits of OBCS and started to reimburse parts of the procedure.
CONCLUSION
It is impossible to ignore the impact that COVID-19 has had on ophthalmology, and there is no question that OBCS has allowed my practice more flexibility and adaptability during this time. OBCS provides a win-win scenario for both the provider, by increasing reimbursement per cataract procedure, and the overall health care macroeconomics system, by eliminating unnecessary fees associated with cataract surgery performed at an ASC.
1. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21 000 cases in the United States. Ophthalmology. 2016;123(4):723-728.
The Advantages Outweigh the Disadvantages
Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth), FRCS(Edin)
Dublin, Ireland

I started practicing ophthalmology in South Africa. I worked in a private eye hospital with four ORs, two excimer laser suites, and more than 20 ophthalmic colleagues. When I relocated to Ireland and started practicing ophthalmology here, I was immediately confronted with a new reality: All cataract surgeries—public and private—were performed in a hospital setting. Turnover was significantly slower in this environment. The most innovative approach at that time, in 1998, was to use a day care facility to usher patients in and out of surgery and the hospital’s OR and infrastructure to perform surgery (see What Is a Day Care Facility?). Things have changed since that time, thank goodness.
Today, one public hospital in Ireland is dedicated to eye care and otorhinolaryngology. Private surgery is performed in general hospitals, most of which do not have a dedicated ophthalmology OR. In those settings, nursing teams could be doing eye surgery in the morning and bowel surgery that same afternoon. I cannot think of an ophthalmologist who performs surgery who does not see room for improvement in the patient experience and for the professionals providing the medical services in this scenario.
The challenge with setting up an ASC in Ireland is that one cannot negotiate with the health insurance providers whether or not they will acknowledge the facility before building it. I know of ophthalmologists who have built a facility only to have their applications for insurance coverage denied. They were never even able to perform a single case in their ASCs. The only route to possible success with an ASC is to implement a cash-pay model. In ophthalmology, there are enough procedures that can be performed in this model, including phakic IOL implantation, refractive lens exchange/custom lens replacement, and some oculoplastic surgical procedures.
EXAMINING OBS
Another possibility that exists in the cash-pay model is building an office-based OR. If the number of self-paying patients can cover the cost of building and running an office-based OR, there is little reason not to proceed, in my view. I recently took time to research OBS to see if it is the right fit for Wellington Eye Clinic, and I uncovered some of the advantages of this surgical model.
We have our own LASIK suite within the clinic where we perform laser vision correction, corneal femtosecond laser procedures such as intrastromal corneal ring segment implantation, and CXL. We know how to provide an excellent patient experience, and we think that we can cut what is a 5-hour visit for cataract surgery in a hospital’s day care facility to about an hour in an office-based OR in our own facility. We are familiar with doing procedures with topical anesthesia only.
All of this experience translates well to an OBCS model. We would adopt oral sedation and topical anesthesia and have patients stay in their own clothing. Unlike the hospital experience, with OBCS, the entire patient experience is under our control. All professional services are being provided by our own medical team—a team dedicated to ophthalmologic care.
The costs of surgery can be managed better. If a patient needs to return to have a toric IOL realigned, this service can be offered at no cost within our own OR. If this were to be done at the hospital, patients would be charged a full fee for follow-up surgery. In an office setting, ophthalmic procedures can be profitable if the turnaround time is quick enough. We believe we can replicate the model we have established in our LASIK suite.
Being profitable is not the primary objective but an additional benefit of building an office-based OR. Controlling the entire environment, the surgical process, and the patient experience are the primary objective and goal.
CONCLUSION
OBCS is not in mainstream practice in Ireland, but the research I have done suggests that the advantages outweigh the disadvantages. We can still perform the surgical cases that require general anesthesia or closer monitoring in a hospital or ASC environment, but for healthier patients who want to get in and out of a medical setting in the shortest time possible and in the safest environment possible, OBS is a compelling proposition. Moreover, in the time of COVID-19, patients prefer clinic environments to hospitals for fear of contracting SARS-CoV-2 or another virus. In my opinion, if the arguments for OBS are not sufficiently compelling now, they never will be.
We Perform OBS, and We Are Never Looking Back
Isabel Dapena, MD, PhD
Rotterdam, Netherlands
Jack S. Parker, MD, PhD
Alabama, United States


In our experience, surgery in the hospital is no fun for almost everyone involved. It is an all-day affair for patients, typically starting with an early morning arrival, an embarrassing gown, needle sticks, and IV medication. They’re not allowed to eat or drink anything or to access their smartphones. They sit in a big room with no privacy and nothing to do except worry.
Family members get antsy in the waiting room, which is now probably inhospitable thanks to a lack of adequate seating because of the COVID-19 pandemic. In some centers, there’s a chance that family members are not in the waiting room but are instead in one of several lines of chairs set out in an adjacent hallway.
On the staff side, doctors may feel disgruntled and distracted by hospital bureaucracy, staffing shortfalls, and the complaints of patients and their families. The problem is the hospital, which cannot match the efficiency and economics of an ASC. What only a few people know is that there’s something much better than an ASC—the surgeon’s own office.
UTILITY
The concept of in-office surgery entered the popular consciousness in 2016 with the publication of a study of 21,000 eyes undergoing in-office phacoemulsification,1 but even before then in-office surgery was offered elsewhere. At the Netherlands Institute for Innovative Ocular Surgery, where one of us (I.D.) practices, in-office corneal transplantation has been the standard for more than 14 years.
The first question everyone asks about in-office surgery is this: Will it be reimbursed? The simple answer in the United States, in the experience of one of us (J.P.), is yes.
A BETTER SCENARIO
With that established, allow yourself to imagine the advantages of in-office surgery. Your patients show up to your familiar office. They are permitted to eat breakfast and have coffee. They don’t need an IV drip, and they may wear their normal clothes.
You perform surgery with your favorite instruments and your trained staff, who know exactly what you like. Meanwhile, the patient’s family waits comfortably in your waiting room. You move efficiently from case to case. If you like, you see some patients in clinic between surgical cases. After an hour’s time, door-to-door, your patient and their family leave, ready to enjoy the day.
Both of us use a modular downflow hood (SurgiCube, SurgiCube International) for our in-office procedures to ensure sterility and safety. This unit, designed by Gerrit Melles, MD, PhD, has been exceptionally easy and gratifying to work with (Figure 2). We cannot imagine ever going back to the hospital for routine intraocular surgery.

Figure 2. The SurgiCube allows an ultraclean surgical environment by supplying HEPA-filtered air to the OR using a unidirectional airflow technique.
Courtesy of Isabel Dapena, MD, PhD
1. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21,000 cases in the United States. Ophthalmology. 2016;123(4):723-728.
Office-Based Surgery in India
Sri Ganesh, MBBS, MS, DNB, FRCS
Karnataka, India

The popularity of OBS is increasing because it is more convenient and because of its reduced costs for infrastructure and maintenance. An OR attached to the practice is especially convenient for cash-pay cataract and refractive surgery patients. The procedure is more profitable and has minimum requirements for staff and basic equipment.
ADVANTAGES
OBS is more convenient for both surgeons and patients. For surgeons, scheduling is easier; there is less formality and paperwork than surgery in a hospital or ASC; the procedure boasts a faster turnover of patients, making it a more efficient system; and the profitability margin is higher. Another advantage is that surgeons can use their own equipment and preferred settings.
For patients, they are familiar with the location and the staff, and same-day surgery may be performed in certain circumstances, which likely increases patient satisfaction. OBS also offers patients a more personalized experience.
DISADVANTAGES
Many elderly patients with cataract have comorbidities like diabetes, hypertension, and cardiac conditions that may need monitoring by an anesthesiologist. Management of these conditions in an adverse situation may present a safety issue during OBS. These and other comorbidities may increase the risks associated with ocular surgery. Likewise, some patients may require sedation or general anesthesia, which may not be feasible in an office-based surgical suite.
Some insurance companies reimburse less for OBS or may not recognize centers without quality accreditations. Also, insurance requires a lot of paperwork, and staff may spend time following up on payments, which may be better in an ASC.
There may be a costly investment associated with beginning an OBS practice, especially for surgeons without access to higher-end equipment like microscopes, phaco machines, and femtosecond and excimer lasers. In this situation, the cost of investment in a surgical suite may prove uneconomical, and it might be easier to share equipment at an affiliate ASC.
PERSONAL EXPERIENCE
When I started my practice 26 years ago, I used an in-office surgical suite to perform cataract and glaucoma surgery and minor oculoplastics procedures. I later added a refractive surgery laser suite. At that time, most patients paid cash for their procedures, and insurance payments were less than 20%. The in-office surgical suite was convenient; I could perform same-day surgeries with highly efficient turnover and minimal staff. Over the years, we expanded and added other specialties and grew into a full-fledged hospital.
Office-based surgical suites are ideal when starting individual practices. They offer efficiency, high profitability, and good patient satisfaction. That said, it is good to be attached to an ASC or hospital in order to treat high-risk patients with comorbidities or those who require sedation or general anesthesia.
The OBS Model Is Here to Stay
Ivan Mac, MD, MBA
North and South Carolina

It is to be hoped that 2021 will bring an end to the COVID-19 pandemic. After this pandemic, the world will look different, and the way we practice ophthalmology will change. One of these changes is a transition to OBS. This model offers a safe, cost-effective, and more personal experience because patients have surgery at a facility with which they are familiar—our offices.
My colleagues and I have been performing OBS for about 6 months (Figure 3). Our center uses the same safety standards as ASCs. Our goal is to provide a patient experience that is superior to that at the hospital-owned ASC where we currently operate. With OBS, patients seem to have decreased anxiety, and most of our cases are completed with oral anesthesia only. The cost savings for our patients are significant because they have much lower copays with OBS compared to at the hospital-owned ASC.

Figure 3. Dr. Mac performs cataract surgery in his office.
Courtesy of Ivan Mac, MD, MBA
CONSIDERATIONS
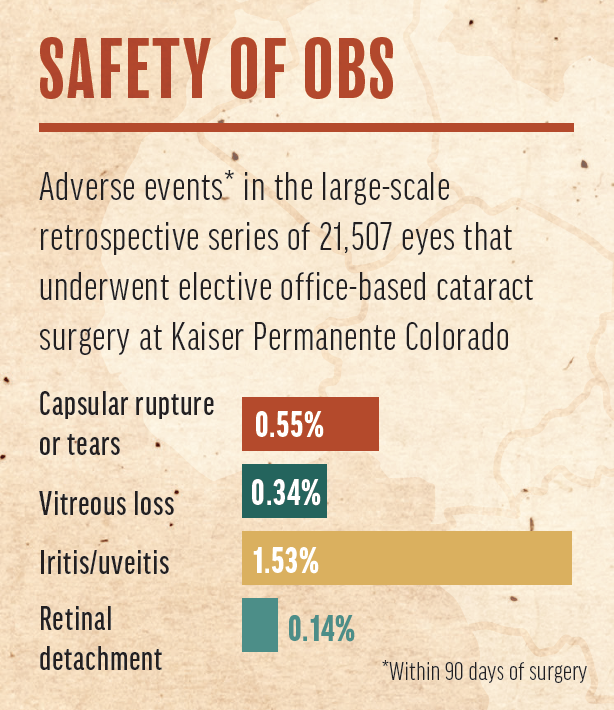
Safety. In terms of safety, OBS has a proven track record. In 2016, Kaiser Permanente Colorado published a large-scale retrospective series of 21,507 eyes of 13,507 patients who underwent elective OBCS.1 Adverse events were low (see Safety of OBS). Notably, no cases of endophthalmitis were observed within 30 days of surgery.
Economics. At this time, we are performing a mix of procedures in our center. The majority are self-pay cataract surgery, refractive lens exchange, and phakic IOL (Visian ICL, STAAR Surgical) implantation. We just received our first commercial insurance contract and look forward to gaining more in the future. At the moment, Medicare does not reimburse an OBS facility fee, but in 2016, CMS requested feedback from industry about OBCS. It is likely that CMS will cover OBS in the future because the model can provide Medicare savings by reducing the need for an anesthesia provider.
Because of the lower upfront cost to develop our OBS suite versus a traditional ASC, we were able to invest significantly more money in the most advanced cataract surgery equipment, including a femtosecond laser and a high-definition operative scope with recording capability. Our operative suites are also considerably larger than what we find at a typical ASC, which contributes to a more relaxed working environment.
Drawbacks. We typically cannot provide general anesthesia in an OBS environment, so cases that require general anesthesia must be performed in an ASC. Also, revenue per case from commercial insurers will most likely be lower for OBS than in a traditional ASC. As stated earlier, CMS does not pay a facility fee for OBS, but this may change in the future.
CONCLUSION
The OBS model is here to stay and will likely become more popular going forward. We decided that now was the time to get on board, and it has enhanced our ability to deliver high-quality, cost-effective care to patients.
1. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21,000 cases in the United States. Ophthalmology. 2016;123(4):723-728.
