


CASE PRESENTATION
A 74-year-old man who achieved a poor visual outcome after cataract surgery with a multifocal IOL is referred for an evaluation. The patient was diagnosed with macular corneal dystrophy before his referral. His history is significant for thermal keratoplasty 30 years ago.
On presentation, the patient’s BCVA is 0.9 OD with a refraction of +1.75 -1.00 x 170º and 0.6 OS with a refraction of +4.00 -1.50 x 20º. A slit-lamp examination reveals atypical corneal findings (Figure 1). OCT imaging is performed (Figure 2). Biomicroscopy shows a well-centered diffractive multifocal IOL in each eye. Fundoscopy is normal in the right eye but suggestive of branch retinal vein occlusion (BRVO) with collateral vessel formation in the left eye.

Figure 1. A slit-lamp examination finds a pseudophakic eye and eight pigmented spots that penetrate deep into the cornea. The distribution of the spots is symmetrical.
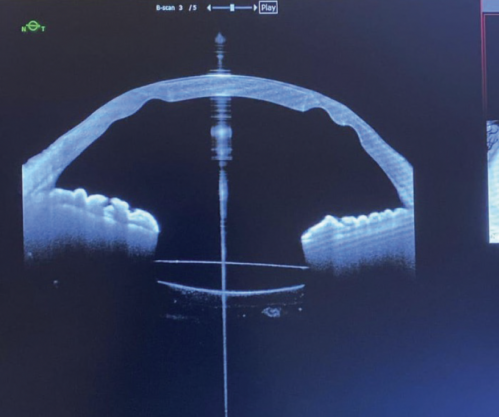
Figure 2. OCT imaging reveals indentations that correspond to the spots seen at the slit lamp. A retraction of the posterior corneal surface is observed in the areas of the spots.
Corneal topography of each eye (Figure 3) finds a flat central cornea and a peripheral area that corresponds to spots visible on an OCT scan. These spots are arranged in a geometric pattern typical of thermal keratoplasty. Figure 4 shows the endothelial cell study.
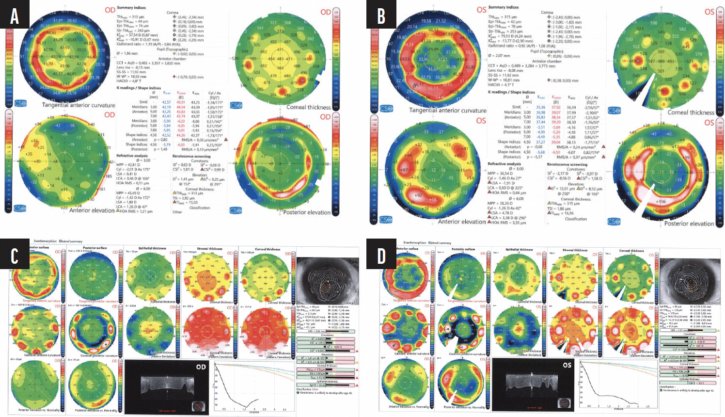
Figure 3. Corneal topography of the right (A, C) and left (B, D) eyes. Flattening of the central cornea of each eye is evident rather than the steepening normally expected after thermal keratoplasty.
Figure 4. Corneal endothelial density is normal, and cell morphology is adequate.
How would you proceed?
—Case prepared by Jorge L. Alió, MD, PhD, FEBOphth, FWCRS, and Hussein Almuhtaseb, MD, MSc, FEBO, FICO, FRCSEd

FRANCESCO CARONES, MD
This is a highly unusual case. Both corneas, contrary to what is typical after thermal keratoplasty, are decidedly flat instead of curved, and the laser lesions are well demarcated.
Regardless of what led to these unexpected results, the refractive outcome of cataract surgery in each eye is hypermetropia and astigmatism, and the patient has anisometropia. It is unclear if the refraction is stable or if it fluctuates (either daily or over a longer period of time) because of the weakened and altered corneas. For the purposes of this article, I will assume the refraction is stable.
First, the patient would undergo a contact lens trial with a plano target in each eye to determine if he would be satisfied with an emmetropic result. He might remain dissatisfied with the multifocal IOLs due to higher-order aberrations and poor visual acuity in the left eye (probably a consequence of BRVO).
If the patient is satisfied with the contact lens trial, piggyback IOLs would be implanted to correct his refractive error. If he reports visual disturbances, the only solution would be to perform an IOL exchange for a monofocal or enhanced monofocal IOL. In this situation, it would be important to discuss whether he prefers spectacle independence at distance or near. I would also consider an IOL exchange if his refraction fluctuates owing to corneal instability.

ARTHUR B. CUMMINGS, MBCHB, FCS(SA), MMED(OPHTH), FRCSED, CERTLRS, FWCRS
The next steps depend on the patient’s desires and willingness to undergo an IOL exchange. I will assume that he wishes to proceed and wants to retain a full range of vision but with a higher quality of vision.
Customized laser vision correction (LVC) might improve the patient’s vision to a satisfactory level. Given the posterior corneal changes, however, LVC is unlikely to provide an improvement to the corneal optics that is sufficient to minimize dysphotopsias from the diffractive optics. A hard contact lens fitting could help determine whether LVC would be beneficial. My guess is that it would not and an IOL exchange must be considered.
I would likely exchange the multifocal IOL in the dominant eye for a monofocal lens such as a Clareon (Alcon) with a target of emmetropia. I would review the previous biometry measurements to determine the source of the refractive surprise and incorporate this information into the IOL power calculation. I would avoid lens implants with optics altered to increase depth of focus. Instead, I would select an IOL that creates negative spherical aberration for the whole-eye wavefront when the oblate cornea is taken into account. For the nondominant eye, I would opt for a small-aperture IOL and a refractive target between -1.00 and -1.25 D. This strategy should reduce the dysphotopsias due to corneal aberrations, create some depth of focus, and maintain a reasonable refractive balance between the two eyes.
Informed consent would cover all possible complications peculiar to this case, the particular risks of an IOL exchange, and the medical retinal issues. The patient may decide against surgery. I would support whatever decision he makes.

PAVEL STODULKA, MD, PHD
The patient has eight symmetrical maculas of the cornea that are affecting the shape of each cornea. The IOL calculation likely did not account for the flat central cornea, which likely led to the refractive surprise. Additionally, retinal disease compromises the visual acuity in the left eye, but his corrected distance vision remains adequate to justify retaining the multifocal IOL.
My preference for additional intervention would be to address the lens rather than the cornea. Unless the patient’s visit is taking place only a few weeks after multifocal IOL implantation, I would not dare to exchange the IOLs but would instead implant an add-on lens to correct his hyperopia and low astigmatism.
Although his distance-corrected near visual acuity is not specified, it appears acceptable given the available information, despite the multifocal IOLs, aberrated corneas, and imperfect corrected distance visual acuity. The corneas are thin and have an unusual shape, likely due to thermal keratoplasty. Each eye has a healthy endothelial cell count.
A corneal incision would be made at the steep meridian (80º OD and 110º OS). The 2.2-mm incision would be enlarged slightly in the right eye and more so in the left eye to correct astigmatism. Given the complexity of the corneas, I would avoid toric lenses to simplify both logistical and optical considerations. I routinely use the IPCL phakic IOL (EyeOL UK) as an add-on IOL in situations like this one. I would expect the refractive outcomes to be precise because the patient’s refractive errors are small.
Retinal edema can increase hyperopia. Though not mentioned in the case presentation, if retinal edema is evident in the left eye, an intravitreal injection of bevacizumab (Avastin, Genentech/Roche) would be performed before proceeding to IOL surgery.
I suspect the diagnosis of macular corneal dystrophy is incorrect. It must have been based on scars resulting from a strange type of thermal keratoplasty because I do not see any maculas of the cornea outside of the eight regularly spaced spots, which is a typical thermal keratoplasty pattern.

JEFFREY WHITMAN, MD
This patient underwent an unknown type of thermal keratoplasty that produced flat rather than steep corneas. A history of macular dystrophy is noted in the case presentation but was not evident during the slit-lamp examination or with OCT imaging. The endothelial cell count for the right eye is half that for the left eye, but the patient’s visual acuity in the right eye corrects well. The BRVO in the left eye could negatively affect his visual outcome after further intervention, but macular OCT imaging is not provided. Whether he was a suitable candidate for a multifocal lens in either eye is a separate discussion.
When contemplating further intervention, my top priority would be to avoid injuring the corneal endothelium. First, the patient would undergo a (preferably hard) contact lens fitting in both eyes. If the vision he achieves is unsatisfactory or contact lens wear is intolerable, then I would consider performing an IOL exchange for a Light Adjustable Lens (RxSight), implanted either in the bag if it is intact or in the sulcus. A dispersive OVD would be placed against the cornea, and a delicate surgical technique would be employed. This strategy would give me the most latitude for hitting a refractive target without increasing visual aberrations.


WHAT WE DID: JORGE L. ALIÓ, MD, PHD, FEBOPHTH, FWCRS, AND HUSSEIN ALMUHTASEB, MD, MSC, FEBO, FICO, FRCSED
The clinical findings in this case provide a dramatic illustration of how Svyatoslav Fyodorov, MD, performed thermal keratoplasty in the late 1970s. During the procedure, the cornea was perforated in multiple locations down to the endothelium with an incandescent metal thread until a drop of aqueous emerged. The retraction of the burn sealed the perforation. Four perforations were made symmetrically per hemisphere for a total of eight spots. The diameter was usually 6 mm. The resulting scars indented the central cornea, and the refractive aim was hyperopia.
Holmium laser thermal keratoplasty and conductive keratoplasty were later developed as less traumatic alternatives to Fyodorov’s original technique. Most patients experienced a progressive loss of effect to the point of almost total regression that left them with irregular corneas.
The long-term effects of thermal keratoplasty in this case were atypical corneal flattening and irregular astigmatism. Why the flattening occurred is unclear, but it led to inaccurate IOL power calculations. A multifocal IOL, moreover, was obviously a poor choice for the patient.
A piggyback IOL (Eyecryl Plus, Biotech Healthcare) was implanted in the sulcus of each eye. The goal was to restore binocularity. The IOL power was selected based on the refraction. The postoperative refraction of each eye was plano -1.00 x 90º. The patient enjoyed improved uncorrected distance and near visual acuity after surgery and reported a high level of satisfaction.
