



It is impossible to avoid being inundated with discussions of AI on the television, radio, podcasts, or social media. Some herald AI as the next great advance, whereas others view the technology as evidence of further dehumanization.
I have never fully understood the term AI. The word artificial typically has a negative connotation. People bemoan artificial flavorings, avoid artificial ingredients, and denigrate individuals for being artificial, yet they are drawn to AI. What would the antonym of AI be—real intelligence? The terminology seems poorly chosen.
Perhaps what we physicians are really discussing, at least regarding the diagnosis, management, and treatment of keratoconus, is assisted intelligence. Diagnostic instruments allow us to diagnose keratoconus at an earlier stage than was previously possible, help us detect subtle disease progression, and let us evaluate the effectiveness of treatment.
ADVANCES IN CORNEAL IMAGING TECHNOLOGIES
The first modern imaging tool was computerized videokeratoscopy, which was introduced in 1984 by Stephen D. Klyce, PhD.1 Although Placido imaging dates back hundreds of years, digitization and computer analysis of a Placido image enabled the identification of subtle changes on the anterior corneal surface that would likely be missed by an observer. The technology’s limitations first became apparent in the field of refractive surgery when patients who met all standard preoperative parameters developed ectasia after refractive surgery.2 Subsequent developments in corneal imaging, including Scheimpflug photography and OCT, revealed that many of these individuals exhibited ectatic changes on the posterior but not the anterior corneal surface.3
REDEFINING KERATOCONUS DIAGNOSIS
The seminal 2015 article “Global Consensus on Keratoconus and Ectatic Diseases” published in Cornea stated that changes on the posterior corneal surface and/or changes in pachymetric progression are mandatory findings for a diagnosis of keratoconus, with or without anterior corneal abnormalities.4
Clinicians' ability to detect early ectatic change, however, predates the development of methods to alter the natural course of keratoconus. A sea change occurred with the introduction of CXL, which can slow or stop disease progression. Until then, all treatments addressed relatively late-stage keratoconus, and early diagnosis was not critical. Today, early disease detection and treatment with CXL can limit or prevent vision loss.
MODERN TOMOGRAPHIC IMAGING
Modern tomographic imaging helps clinicians diagnose keratoconus, monitor disease progression, and evaluate the effect of treatment. Many devices exist, including the Orbscan II (Bausch + Lomb), Galilei G4 (Ziemer Ophthalmic Systems), and Sirius (CSO), but the Pentacam (Oculus Optikgeräte) remains the most commonly used instrument for both keratoconus and refractive surgery evaluations.
The Pentacam uses Scheimpflug photography and a rotating optical head to capture 25 or 50 anterior segment optical cross-sectional images. These optical slices are then reconstructed to generate a 3D image of the eye’s anterior segment. Edge detection software can identify the anterior and posterior corneal surfaces, the anterior lens, and occasionally the posterior lens. Utilizing these surfaces, the device can construct a full pachymetric (corneal thickness) map and anterior chamber depth map.5
BELIN/AMBRÓSIO DISPLAY
The Belin/Ambrósio enhanced ectasia display (BAD) is the most widely used Pentacam software for refractive screening and keratoconus detection.
Introduced more than 15 years ago, this map has undergone numerous refinements. The current software performs a proprietary logistic regression analysis of nine separate parameters to determine variance from normal. The BAD software can detect subtle anatomic changes earlier than can be detected through the visual inspection of standard displays. The BAD analyzes both elevation and pachymetric parameters (Figure 1).
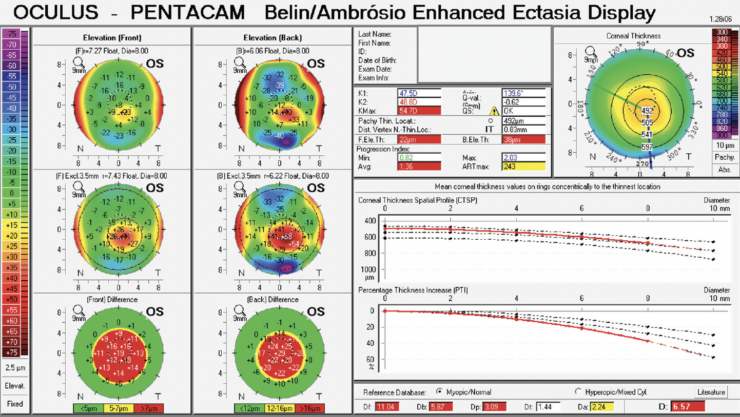
Figure 1. BAD of an eye with moderately advanced keratoconus. The first column (left) shows a positive island of ectasia, visually enhanced with the ERS in the middle display. The second column shows a similar finding for posterior elevation. The corneal thickness map (upper right) shows a thin cornea, and the pachymetric progression graphs indicate an increased rate of change.
Elevation Analysis
The left side of the BAD shows both anterior and posterior elevation against a standard best-fit sphere taken from the central 8-mm optical zone and against an enhanced reference surface (ERS), which further amplifies ectatic regions of the cornea. The ERS is constructed by removing a variable 3.0- to 4.0-mm optical zone centered on the thinnest point of the cornea from the standard best-fit sphere. Removing this area eliminates the bulk of the cone, allowing the ERS to contour to the more normal corneal periphery and further accentuate the conical region. The change in elevation when transitioning from the standard best-fit sphere to the ERS is highly accurate for distinguishing keratoconic from healthy corneas.6
Pachymetric Progression Graphs
The right side of the BAD shows pachymetric data. Normal values for corneal thickness vary greatly, and standard apical corneal thickness has little discriminatory potential because of significant overlap with keratoconic corneas. In addition to a traditional corneal thickness map, the BAD also shows pachymetric progression graphs. The concept underlying pachymetric progression graphs is similar to the ERS. A keratoconic cornea is thinner in the conical ectatic region but has a more normal corneal periphery. The rate of change in corneal thickness from the normal periphery to the cone is more rapid than in a healthy cornea.
Although this may seem intuitive, the power of the pachymetric progression graphs lies in their ability to distinguish a thin but otherwise normal cornea (exhibiting normal pachymetric progression) from an ectatic cornea with a similar central corneal thickness (Figure 2).7

Figure 2. Two corneas with similar apical pachymetry. The cornea on the left shows normal pachymetric progression, indicating a thin but otherwise healthy cornea. The cornea on the right demonstrates highly abnormal pachymetric progression that is suggestive of keratoconus.
Interpreting BAD Parameters
All measured parameters in the BAD are color-coded according to their variance from normal. Parameters change from white to yellow at 1.6 standard deviations from the norm and to red at 2.6 standard deviations from the norm. No single parameter has enough discriminatory ability to serve as an isolated screening parameter. The power of the BAD is that it uses a series of nine parameters in a logistic regression analysis and produces an overall reading (final D), which has demonstrated both sensitivity and specificity in indicating variance from normal.5 Variance from normal is different, however, from having high specificity for diagnosing keratoconus because other conditions (eg, a history of refractive surgery or corneal edema) also vary from normal and have an abnormal final D. To increase specificity in diagnosing keratoconus, one must eliminate these other (fairly obvious) conditions or look at other BAD parameters in addition to the final D.
BAD in Epithelium-on CXL Studies
A current US FDA phase 3 study of epithelium-on CXL is using the BAD as one of its major inclusion criteria. The research increases diagnostic specificity by mandating an abnormal pachymetric progression and an abnormal posterior elevation at the thinnest point in addition to an abnormal final D.8
THE BELIN ABCD PROGRESSION DISPLAY
Whereas the BAD prioritizes showing variance from normal, the Belin ABCD progression display was designed solely to follow keratoconus progression. Numerous parameters have been used in the past to monitor and document progression, the most common of which is maximum keratometry (Kmax). All of these parameters were based on the anterior corneal surface. They were therefore unable to detect early ectatic changes, and further degradation in visual function had to occur before disease progression could be detected. The ABCD progression display was developed both to alleviate this limitation and to allow the detection of ectasia progression without accompanying vision loss.
Understanding the ABCD Parameters
The Belin ABCD progression display shows three objective parameters:
- A is the anterior radius of curvature taken from a 3-mm optical zone centered on the thinnest point;
- B is the posterior (back) radius of curvature taken from a 3-mm optical zone centered on the thinnest point; and
- C is the minimal corneal thickness.
Each of these individual parameters is shown graphically over time (up to eight exams may be displayed) with their accompanying confidence intervals (CIs) for change. Both 80% and 95% one-sided CIs are displayed, which represent changes that exceed the normal measurement noise.9 Six different CIs are shown. Green bars are taken from a normal patient population. These bars are most applicable for very early disease and pediatric patients. Red bars are generated from a published population of keratoconus patients. These bars are applicable to older patients with more established disease. Blue gates are generated from a population that underwent CXL.
All three of these gates are displayed with a dotted or hatched line for the 80% CI and a solid line for the 95% CI. The fourth parameter, D, is best spectacle-corrected distance visual acuity. Although this is displayed graphically, it has no associated CI because this is not an objective machine-generated parameter (Figure 3).
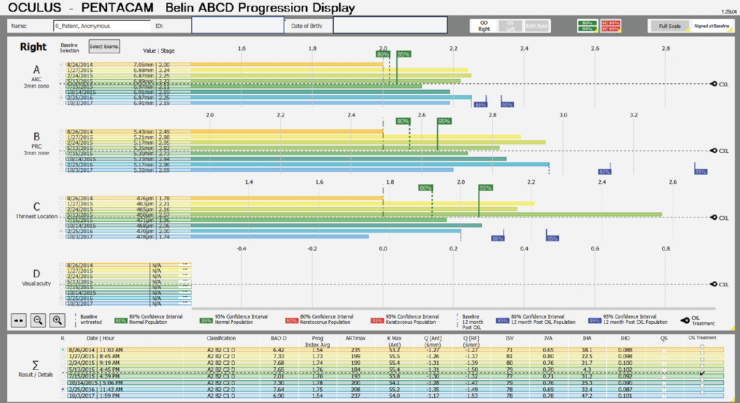
Figure 3. Belin ABCD progression display of a pediatric patient with moderately advanced keratoconus. The display shows marked progression (green gates) before CXL that is indicated by black dotted lines. Following CXL, stability is documented by the blue gates.
Clinical Advantages of the ABCD Progression Display
The clinical advantage of the Belin ABCD progression display is that it can document statistically significant progression despite a stable anterior surface or stable Kmax. Numerous peer-reviewed published articles have independently validated the progression display and have shown that it can detect disease progression, on average, 6 months earlier than relying on Kmax.10-12
THE FUTURE OF KERATOCONUS MANAGEMENT
Most current treatments are reactive, with intervention’s occurring only after vision has been lost. The development of newer treatments with improved risk-benefit ratios would make earlier intervention more appealing with the goal of preventing vision loss. Earlier intervention would benefit greatly from assisted intelligence.
1. Klyce SD. Computer-assisted corneal topography. High-resolution graphic presentation and analysis of keratoscopy. Invest Ophthalmol Vis Sci. 1984;25(12):1426-1435.
2. Binder PS. Ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2003;29(12):2419-2429.
3. Ambrósio R Jr, Dawson DG, Salomão M, Guerra FP, Caiado AL, Belin MW. Corneal ectasia after LASIK despite low preoperative risk: tomographic and biomechanical findings in the unoperated, stable, fellow eye. J Refract Surg. 2010;26(11):906-911.
4. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369.
5. Belin MW, Khachikian SS. Corneal diagnosis and evaluation with the OCULUS Pentacam. Highl Ophthalmol. 2007;35:5-8.
6. Belin MW, Khachikian SS, Ambrosio R Jr. Keratoconus/Ectasia Detection with a Modified (Enhanced) Reference Surface in Elevation Based Corneal Tomography. 2nd ed. Jaypee-Highlights Medical Publishers; 2012:93-104.
7. Orucoglu F, Toker E. Comparative analysis of anterior segment parameters in normal and keratoconus eyes generated by Scheimpflug tomography. J Ophthalmol. 2015;2015:925414.
8. Epion Therapeutics. Epithelium-on corneal cross-linking in subjects 8 to 45 years of age with keratoconus (APRICITY-A). ClinicalTrials.gov identifier NCT06100939. Updated September 26, 2024. Accessed September 27, 2024. https://clinicaltrials.gov/study/NCT06100939
9. Duncan JK, Belin MW, Borgstrom M. Assessing progression of keratoconus: novel tomographic determinants. Eye Vis (Lond). 2016;3:6.
10. Dubinsky-Pertzov B, Reinhardt O, Gazit I, et al. The ABCD keratoconus grading system-a useful tool to estimate keratoconus progression in the pediatric population. Cornea. 2021;40(10):1322-1329.
11. Neuhann S, Schuh A, Krause D, et al. Comparison of variables measured with a Scheimpflug device for evaluation of progression and detection of keratoconus. Sci Rep. 2020;10(1):19308.
12. Ozalp O, Atalay E. Belin ABCD progression display identifies keratoconus progression earlier than conventional metrics. Am J Ophthalmol. 2022;236:45-52.
