



I have spent a lifetime in ophthalmology in East Africa. I was brought up in Kenya but went to secondary school and university in England and performed my ophthalmology fellowship in Canada. I started as a medical officer in Wajir and Garissa in Northern Kenya, so I was aware of the conditions that would face me when I came back from my fellowship.
I have been lucky, having had an interesting job in an interesting place at an interesting time. My learning took off when I came back to Kenya and began practicing ophthalmology. This was in the era when modern cataract surgery with IOLs was just getting started. Most cataract surgery was performed as intracapsular cataract extraction (ICCE), with spectacles prescribed thereafter to correct the aphakia. During my residency in Canada, IOLs had not been used, and, as a result, I basically had to teach myself IOL implantation. I implanted my first IOL on the Orbis Flying Eye Hospital, which was visiting Kenya at the time, around 1982. Vitrectomy and vitreoretinal surgery were unheard of, and there was no laser machine at that time in East Africa.
THE EARLY YEARS
My family moved to East Africa in 1948, when I was 4 years old. My father practiced plastic surgery, and I think he was the first plastic surgeon in Kenya. Seeing the need for rural health care in huge uncovered areas, he started the flying doctor service in East Africa, which still functions today. The main nongovernmental organization (NGO) associated with this service is the African Medical and Research Foundation.
I was first exposed to ophthalmology during the elective time of my training, which I spent in Tanzania with the well-known medical missionary and ophthalmic surgeon Joseph Taylor, FRCS. This experience inspired me to pursue ophthalmology as a career because I was able to witness the dramatic effect that treatment could have on people’s lives, and the relative ease with which this could be achieved.
Equipment was minimal at that time. We would get into the aircraft with just two or three cataract sets. It was there I learned that cataract surgery could be done in even the most basic conditions.
After my training, I started work just outside Nairobi, Kenya, at Kikuyu Eye Hospital (Figure 1), where I have spent most of my working life. After 18 years there, I moved to our sister hospital in Dar es Salaam, Tanzania. Both these hospitals were supported by another NGO, Christoffel Blindenmission, now known as CBM. The main objective of both these units was service delivery, so maintaining a high volume of patients and surgeries was important. There was a large backlog of patients who were blind from cataract, and there was no other hospital doing high-volume surgery at that time.

Figure 1. Kikuyu Eye Hospital unit during a typical clinic.
When I started at Kikuyu Eye Hospital, our patients were in the general ward and we performed surgeries in the hospital’s operating room (OR). Often we would have to stop for a caesarean section or surgical emergency. With financing from CBM, we built new wards and a new OR with room to do two operations at a time. These hospitals became among the biggest in Africa in terms of numbers of surgeries. When I left Dar es Salaam, they were seeing about 60,000 patients per year and doing about 7,000 operations per year.
TRAINING AND TRAVELING
To maintain the high volume of cataract surgery, we had to train others to help. I trained unqualified nurse assistants as surgical support staff. Slowly they learned to do the superior rectus suture, incise the conjunctiva, and cauterize bleeding, for example, and eventually they were able to do the whole cataract operation. One of these nurse-surgeons now does extensive work in Sudan, and another has a private practice in Kikuyu. A problem for them, however, is that they have no recognized training or certificate, only my on-the-job training.
I had worked as a general doctor for 3 years in Wajir in Northern Kenya. I well remember the day I arrived; one side of the male ward was occupied by 19 patients who had been mauled by lions. Subsequently the game department shot many of these lions. When I returned to Kenya after my ophthalmic fellowship in Canada, I was keen to bring eye services to Wajir and the whole Northeastern province, the Somali part of Kenya and a dry scrub bush type of country.
The Somali people relied on camels for milk, meat, and their very existence. Sight by Wings, an NGO supported by Sightsavers International, provided aircraft for the purpose of delivering eye care to remote regions. Eye surgeons from the United Kingdom joined me in traveling to the north of Kenya by air, and we did the first eye operations in the area. The team used to cram into a little Cessna P 206 aircraft with all of our equipment.
EXPANDING SERVICES
As time went on, our equipment expanded and improved. We went from loupes to microscopes, from boiling water on a wood fire to electric autoclaves. Patient numbers increased (Figure 2), and it was a big step when a new Cessna 208 Caravan came to Kenya. It could take much more weight and was faster. It had a range of about 1,000 km carrying 3,000 pounds and could take off and land within 0.6 km. A lot of airstrips in the region were short and badly maintained, but the Caravan could cope with most of them. We were then able to extend our services to Somalia, Sudan (Figure 3), and the remote parts of Kenya. As numbers kept increasing, this plane could carry all the consumables for up to 500 operations a week plus two surgeons and their teams. There is nothing worse than running out of a vital drug, suture, or IOL when you are 1,000 km from base, with patients waiting and expecting to be operated on.

Figure 2. Operating inside a tent on a mobile air safari.
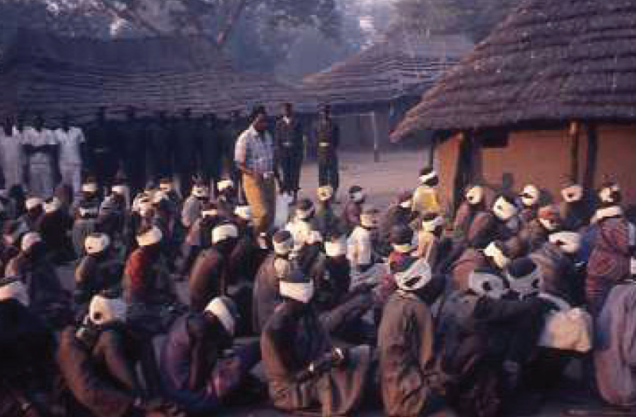
Figure 3. Air safari to Billing, Sudan.
There were no waiting rooms. Patients sat on the ground in the dust and heat (Figure 4). Some had traveled on foot for months or on buses for days. It is distressing to tell a patient with glaucoma in its final stages that there is nothing you can do after the effort he or she has put in to get to you. It is important to honor the dates you have set for your trips, so that you do not disappoint people after the trials they have been through to reach the hospital.

Figure 4. In the days of extracapsular surgery in Sudan.
In 1 week, we could do 500 operations in very basic facilities (Figures 5 and 6). Unfortunately, these times have passed, and, due to the expense and a lack of funds, these eye safaris are not often done nowadays. Many communities that we were able to serve at that time are without eye services now.
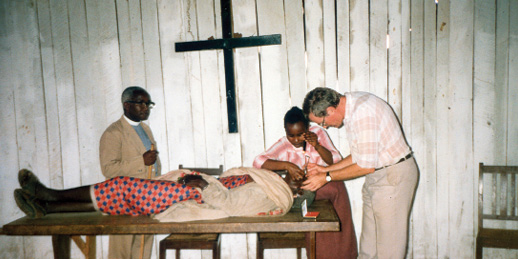
Figure 5. Schiotz tonometry on the altar.

Figure 6. Giving a retobulbar injection on the floor in Sudan.
Kenya has an excellent teaching program at Nairobi University, and many ophthalmologists trained there are now posted throughout Africa—but their program is an exception. In most African countries, there is little ophthalmic training, and, in many cases, clinical officers (paramedics) are trained and licensed to do cataract surgery. They are the backbone of services in Kenya and Tanzania. In Tanzania, these personnel are called assistant medical officers (AMOs), and they run the eye clinics, do the surgery, and even perform caesarean sections when needed.
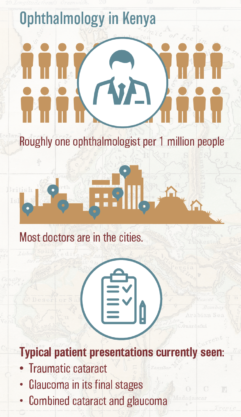
SPECTRUM OF EYE DISEASE
The spectrum of eye disease seen in this region of Kenya is probably similar to that seen in more developed nations, but the pathology is greatly advanced due to the scarcity of doctors. There is roughly one ophthalmologist per 1 million people in this region, and most of these doctors are in the cities. Frequently, patients with bilateral dense cataracts causing blindness walk into the clinic. Morgagnian cataracts are not uncommon. Glaucoma is often in its final stages, and there is little that can be done.
Tumors such as retinoblastoma can be huge protruding masses. Rarely are we able to save the lives of children with retinoblastoma, let alone provide palliative care. Good programs for retinoblastoma are being developed in Dar es Salaam, with support from Nairobi University and donors in Ireland, but the children often come too late or their parents refuse surgery.
HIV is a major health problem. Drugs are available free in the larger clinics in big towns. We see many squamous cell carcinomas of the conjunctiva, which can develop into huge orbital masses. We do not see much cytomegalovirus retinitis.
Congenital cataracts may seem to be common in the region, but this only reflects the lack of services. All these patients end up at the few existing facilities, and they come late. Some are sent straight to blind schools without ever seeing an ophthalmologist. In these schools, we have seen children up to 18 years old blind from cataract. Unfortunately, operating on children at this late age is usually hopeless, with no vision gained. Younger children with cataract are deeply amblyopic, and the normal operation for this condition is an IOL implanted after lens washout. Pediatric ophthalmologists are trained at the Comprehensive Community Based Rehabilitation in Tanzania hospital in Dar es Salaam.
One problem that is probably distinct from those seen in the developed world is the use of toxic traditional medicines, causing corneal ulcers, fungal ulcers, and keratitis. These conditions often do not have good outcomes. I once saw a patient with bilateral incisions at the limbus that penetrated the anterior chamber, which he explained to me had been made by a witch doctor to let out the “bad fluid.” I sutured the wounds, and he recovered. Two things about these incidents are surprising to me. First, these cases of penetrating trauma, including many with sticks and thorns, do not often develop endophthalmitis. Second, even traditional doctors continue to use toxic herbs in the eye despite their dismal results (Figure 7). Pain is often treated by burns to the skin applied over the area of pain, especially in Somalia.
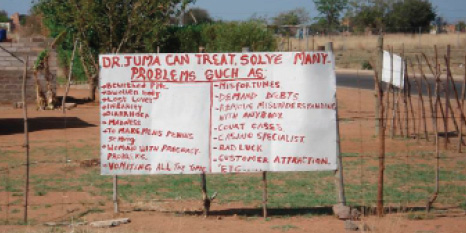
Figure 7. A sign posted by a local doctor, with no mention of cataract surgery.
Ian Murdoch, MSc, MD, FRCOphth, a glaucoma consultant surgeon at Moorfields Eye Hospital in London, started a telemedicine program, through which we were able to access Moorfields consultants. The main trouble with this was that our patients often did not wait for the resulting advice. Also, many times we were unable to carry out the advice we received, as we did not have the necessary drugs, equipment, or skills that were recommended. Now I no longer use telemedicine and instead usually write to friends.
Luckily patients accept many of our failures with grace and will even thank the doctor. “Inshalla,” they say—if God wills.
BREAKAGES AND MAINTENANCE
Ophthalmologists visiting our region need to cover many areas across many subspecialties, as there is no one to refer patients to. The advent of the Internet has been a great help as a resource during outreach efforts in the bush.
Breakages and maintenance are also part of the excitement of working in developing countries. It is good to have insight into how to maintain microscopes, slit lamps, and sterilizers. We must have spare parts available because they can take months to arrive. A powerful torch should always be handy.
Recently, while I was operating in the Democratic Republic of the Congo, the microscope bulb blew, a spare could not be found, and the spare that should have been in the instrument housing had not been installed. Then the main power went out, and the generator could not be started. When we tried to bypass the generator, an electrical fire started in one of the circuits in the outpatient area. The old switchboard for the sterilizer tripped, and, because it was installed in King Leopold’s time, no one in the hospital could restart it. We ran out of surgical gowns. I went back to the hotel to cool off.
Most ophthalmology units today have good equipment for routine operations. Vitrectomy machines are usually available, and these are a great help in managing capsular rupture and vitreous loss. Good microscopes and biometry are readily available, but phaco machines are only sometimes available. The St. Yvonne Eye Clinic, where I currently work, has an old Alcon unit, which the company says it would not be able to repair if it broke—it must be 20 years old. When it eventually stops working, we will stop doing phacoemulsification. This will be a pity because the combination phaco/trabeculectomy has been a useful and successful operation for us.
We are just starting to teach phaco techniques to the local surgeons. Expense is one reason for using phaco sparingly, although prices keep coming down. A PMMA lens now costs us $3, and a foldable lens $18. The affordable OVDs are methylcellulose and those manufactured by Aurolab India. Some visiting surgeons have experience only with phacoemulsification and have had to learn the manual small-incision cataract surgery (MSICS) that is our routine operation at present. Extracapsular cataract extraction with the incision at the limbus is still used, but the new teaching is MSICS.
CONCLUSION
These days it is difficult for expatriate ophthalmologists to find positions in the developing world as more local doctors are trained. Further, paid positions are rare and volunteering can be problematic. Volunteers need work permits to do even short-term assignments, and registration is needed in the country to be visited.
Figure 8. Use of the cell phone is widespread.
That being said, if ophthalmologists get the chance to go overseas, I think they will find it richly rewarding, especially in the interactions with the locals (Figure 8). Basic surgical techniques such as cataract surgery are well developed, but now we need to teach the local practitioners the subspecialties. There are few subspecialists in this region, and this is an area where visiting specialists who are willing to teach can be extremely valuable.