



Major advances in cataract surgery have occurred over the past decade, and refractive outcomes have significantly improved. In turn, refractive lens exchange (RLE) has become a frequently used refractive surgical modality.
However, RLE candidates must be carefully selected, paying strict attention to risk versus benefit. There are clear differences between the risk profiles of hyperopes and myopes. Risks for postoperative long-term complications, especially in myopes, include posterior capsular opacification (PCO), cystoid macular edema (CME), and rhegmatogenous retinal detachment (RRD; Figure 1).
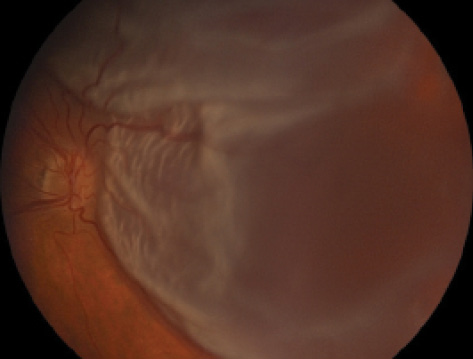
Figure 1. Rhegmatogenous retinal detachment, a potential long-term postoperative complication of RLE.
PCO
The rate of PCO after RLE is thought to be higher than that after cataract surgery due to the younger age of patients undergoing RLE.1 Higher rates of PCO lead to higher rates of Nd:YAG capsulotomy, which increases the risk of RRD. YAG capsulotomy seems to induce vitreous liquefaction and posterior vitreous detachment (PVD), which, in consequence, may create new breaks and enable preexisting asymptomatic retinal breaks to progress to RRD.2
AT A GLANCE
• RLE candidates must be carefully selected, paying strict attention to risk versus benefit.
• Risks for postoperative long-term complications, especially in myopes, include posterior capsular opacification, cystoid macular edema, and rhegmatogenous retinal detachment.
• Extensive informed consent is required, and patients should be educated about warning symptoms to allow prompt treatment.
These changes are suspected to be primarily the effect of the capsulotomy. However, the precise mechanisms are not clearly understood. Half of postcapsulotomy RRDs seem to be caused by horseshoe tears and the other half by antecedent small atrophic holes. An anterior vitreal shift can cause retinal breaks even in the presence of a preexisting stabilized PVD, due to anterior movement of the insertion line of the posterior limiting lamina.3
Several studies have been conducted to assess RRD risk after YAG capsulotomy in myopic eyes, but the results are divergent. Ranta et al showed that, for each millimeter of increased axial length, the hazard ratio for RRD after YAG capsulotomy was increased by 1.5.2 This would therefore suggest that YAG capsulotomy should be avoided if possible in myopic eyes. However, other studies did not find an increased risk of RRD after YAG capsulotomy in patients with high myopia.4
CME
As with cataract surgery, postoperative CME after RLE has been reported. In a post–cataract surgery population, the incidence of clinical CME was 3%, whereas the incidence of subclinical CME diagnosed with OCT was 5%.5 Recently, in a large database study of CME after cataract surgery, high myopia was not found to increase the risk of CME development.6
A SECOND LOOK: Complications of RLE
By Ahmed ElMassry, MD

Refractive lens exchange (RLE) is a refractive surgical option in young patients with anisometropia, eyes that are not anatomically suitable for phakic IOL implantation, and eyes with high hyperopia. Further, in the presence of water vacuoles in the crystalline lenses of patients older than 40 years, RLE is recommended over phakic IOL implantation. Lens options in RLE include multifocal refractive IOLs, designed with several optical zones, and apodized diffractive multifocal IOLs, which have gradual diffractive steps that create a smoother transition between focal points.
The risks of RLE are similar to those associated with cataract surgery. Like cataract surgery, RLE presents challenges in IOL selection, prediction of postoperative refraction, prevention of induced and residual astigmatism, possibility of retinal detachment, achieving good contrast sensitivity, and minimizing the incidence of posterior capsular opacification.
Colin et al1 reported improvement in UCVA in 100% of patients, improvement in BCVA of 2 lines or more in 75% of patients, and loss of BCVA in 0% to 4% of patients treated with myopic RLE. Gabric et al2 found that RLE was predictable, with 87.5% of cases within ±1.00 D of emmetropia and 95.8% within ±2.00 D. In hyperopic RLE, 88% of low hyperopes were within ±1.00 D of the target refraction.2
Good visual outcomes can be achieved with RLE, but complications do occur. The mean incidence of retinal detachment and cystoid macular edema (CME) after RLE are 1% and 0.1%, respectively.3 The risk of retinal detachment after RLE is increased with young age, male sex, degree of myopia, and axial length exceeding 27 mm. Peripheral retinal examination and identification of weak areas to be strengthened with argon laser photocoagulation before surgery are mandatory in these cases. Posterior capsular rupture, the most common complication of RLE, increases the incidence of retinal tears and CME postoperatively.
Considerations
Postoperative Nd:YAG capsulotomy. When YAG capsulotomy is necessary, precautions to decrease the risk of retinal detachment should include using low laser energy and aiming for a small-diameter posterior capsulotomy; however, even with the proper precautions, the possibility of retinal tears or secondary rise of IOP still exists.
Loss of accommodation. One of the most common complications of RLE is the loss of accommodation. Despite the high quality of premium IOLs implanted with current techniques such as laser-assisted cataract surgery, the young patient who undergoes RLE loses his or her natural accommodation. This cannot be replaced by trifocal or multifocal IOLs. Although these lenses provide a reasonable substitute for near and intermediate vision, they affect contrast sensitivity and the accuracy of distance vision in a way that is not comparable with monofocal IOLs or the natural accommodation process.
Short axial length. A different set of complications is possible in eyes with short axial length, including suprachoroidal hemorrhage and malignant glaucoma. When RLE is performed in these eyes, the predictability of IOL power is generally lower. High-add IOLs usually must be special-ordered, which requires time. If two piggybacked IOLs are inserted instead, deposits in the interface typically hinder some of the quality of vision. If deposits between the two IOLs cause opacification, the process of YAG laser posterior capsulotomy becomes difficult and may result in pitting of one of the IOLs.
When piggybacked IOLs are used, there is a lack of evidence regarding which IOL material combination is best—one acrylic and one silicone or two acrylic IOLs. The available studies are too small to rely on. Also up for debate is whether both IOLs should be placed in the sulcus; whether one should be in the bag and the other in the sulcus; whether to perform posterior capsulotomy with optic capture in the posterior rhexis; or whether to do a bag-in-the-lens approach for one IOL and place the other in the sulcus. There are many surgical techniques, and it is a good idea to have more than one basic technique for piggyback IOLs in your armamentarium.
The surgeon must differentiate between short eyes with normal structure of the globe and eyes with microphthalmos with a crowded anterior chamber, which are not suitable for RLE due to the higher risk of suprachoroidal hemorrhage. The risk of increased IOP is also higher with piggyback IOLs, and peripheral iridotomy may be required.
CONCLUSION
For best results with RLE, as with any surgical procedure, adequate preoperative care should be exercised. Preoperative patient counseling should include an explanation of the limitations of surgery, including the consequences of presbyopia, as well as a discussion of the patient’s expectations, the possible need for postoperative enhancement, and the potential for postoperative visual symptoms.
1. Colin J, Robinet A. Clear lensectomy and implantation of low power posterior chamber intraocular lens for the correction of high myopia. Ophthalmology. 1994;101:107-122.
2. Gabric N, Dekaris I, Karaman Z. Refractive lens exchange for correction of high myopia. Eur J Ophthalmol. 2002;12(5):384-387.
3. Barraquer C, Cavelier C, Mejia L, Incidence of retinal detachment following clear-lens extraction in myopic patients. Arch Ophthalmol. 1994;112:336-339.
RRD
In the general population, between 1 in 5,600 patients and 1 in 16,400 patients develop RRD each year.7 In pseudophakic eyes after lens surgery, the rate of RRD is 1:85 over 10 years.8 In general, the risk increases significantly—up to 1:12 cumulative risk—when surgery is complicated by a capsular rupture.9 It is well known that the longer the axial length, the higher the risk of RRD.
In unoperated eyes with more than -10.00 D myopia, the RRD risk is thought to be 1:147 per year.10 After phacoemulsification in myopic eyes, the cumulative RRD risk is 1:45, with large variation between studies.9
In general, younger patients are at a higher risk of RRD after lens surgery.8 This has also been shown for myopic patients.4 Alio et al reported a postoperative cumulative incidence of 1:27 in patients aged 50 years or younger versus 1:40 in patients older than 50 years of age.4 The risk is higher during the first 5 years after lens surgery.
CHANGES AFTER PHACOEMULSIFICATION
In lens surgery, the thick crystalline lens is replaced by a thin IOL. This leads to several physical changes. The volume of the posterior segment increases, leading to a forward movement of the vitreous body. This forward movement may also cause dynamic traction at the retina, promoting formation of retinal tears.7
Further, changes in the vitreous composition—in proteomes, particle size, viscosity, and inflammatory mediators—have been shown.11 Alterations in the hyaluronic acid composition cause changes in viscosity, and this may lead to instability of the vitreous.
All of these factors promote PVD and may thereby promote RRD. Also, the lack of the posterior protuberance of the crystalline lens has been proposed to affect RRD, as the protuberance is thought to reduce vitreoretinal traction during saccadic movements.7 Schäffer et al12 examined the prevalence of anterior vitreous detachment and showed that it was lower in pseudophakic RRD eyes than in pseudophakic non-RRD eyes, indicating strong vitreoretinal adhesions in the former.
PVD
In 1994, Yonemoto et al13 established a formula for the relationship between refractive error and onset of PVD:

In another study, the onset of PVD was significantly earlier both in patients with high myopia and partial PVD (47 vs 59 years) and those with high myopia and complete PVDs (61 vs 70 years), compared with controls.14
Mirshahi et al15 showed that 59% of cataract patients who did not have a PVD preoperatively developed some degree of PVD within 1 year postoperative. A study using OCT in addition to ultrasound to diagnose PVD showed even higher rates: 59% of patients developed a degree of PVD within 1 month after surgery, and 71% within 3 months.16 Further, the longer the axial length, the more likely for PVD to occur in pseudophakic eyes.17
Ripandelli et al18 examined the influence of PVD on RRD in emmetropic eyes. In the group with preoperative PVD, the rate of RRD was 1.1% within 5 years. In the group with no PVD preoperatively, 79% developed a postoperative PVD, of which 7.4% had an RRD. Patients with no preoperative PVD and presence of lattice degeneration are at particular risk.18
As this question has not been addressed in a purely myopic study population, the European Society of Cataract and Refractive Surgeons (ESCRS) is currently conducting a multicenter trial to assess the influence of PVD on pseudophakic RRD in myopic eyes. The MYOpic Pseudophakic REtinal Detachment (MYOPRED) study will include 618 patients with axial lengths of 25 mm or longer scheduled for lens surgery. Patients will be allocated to two groups preoperatively, depending on whether a complete PVD is present or not. The results of this study will contribute to patient safety, as cataract and refractive surgeons will be able to better inform myopic patients preoperatively about their individual risk level for RRD after lens surgery.
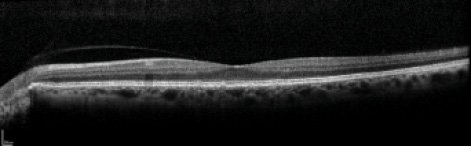
Figure 2. Partial PVD on SD-OCT imaging. OCT imaging can be helpful to define PVD status preoperatively.
CONCLUSION
To prevent and manage RLE complications, there are several pearls to keep in mind:
The presence of PVD should be assessed preoperatively, possibly with OCT (Figure 2);
• RLE in myopes may be most applicable for patients older than 55 years with PVD;
• Prophylactic laser coagulation may be indicated, such as to prevent RRD in the fellow eye;
• Preoperative treatment of lattice areas is still controversial;
• Extensive informed consent is required, as RLE is elective surgery;
• As always, intraoperative complications should be avoided to prevent further risk; and
• Patients should be educated about warning symptoms to allow prompt treatment.
1. Kook D, Kampik A, Kohnen T. Complications after refractive lens exchange [in German]. Ophthalmologe. 2008;105(11):1005-1012.
2. Ranta P, Tommila P, Kivela T. Retinal breaks and detachment after neodymium: YAG laser posterior capsulotomy: five-year incidence in a prospective cohort. J Cataract Refract Surg. 2004;30(1):58-66.
3. Framme C, Wolf S. Retinal complications after damaging the vitreolenticular barrier. Ophthalmologica. 2012;227(1):20-33.
4. Alio JL, Ruiz-Moreno JM, Shabayek MH, Lugo FL, Abd El Rahman AM. The risk of retinal detachment in high myopia after small incision coaxial phacoemulsification. Am J Ophthalmol. 2007;144(1):93-98.
5. Vukicevic M, Gin T, Al-Qureshi S. Prevalence of optical coherence tomography-diagnosed postoperative cystoid macular oedema in patients following uncomplicated phacoemulsification cataract surgery. Clin Exp Ophthalmol. 2012;40(3):282-287.
6. Chu CJ, Johnston RL, Buscombe C, et al. Risk factors and incidence of macular edema after cataract surgery: a database study of 81 984 eyes. Ophthalmology. 2016;123(2):316-323.
7. Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol. 2003;48(5):467-487.
8. Russell M, Gaskin B, Russell D, Polkinghorne PJ. Pseudophakic retinal detachment after phacoemulsification cataract surgery: ten-year retrospective review. J Cataract Refract Surg. 2006;32(3):442-445.
9. Rosen E. Risk management for rhegmatogenous retinal detachment following refractive lens exchange and phakic IOL implantation in myopic eyes. J Cataract Refract Surg. 2006;32(5):697-701.
10. Perkins ES. Morbidity from myopia. Sight Sav Rev. 1979;49(1):11-19.
11. Neal RE, Bettelheim FA, Lin C, Winn KC, Garland DL, Zigler JS Jr. Alterations in human vitreous humour following cataract extraction. Exp Eye Res. 2005;80(3):337-347.
12. Schaffer CB, Poschl EM, Steinwender G, Wedrich A, Ivastinovic D. Low prevalence of anterior vitreous detachment in eyes with pseudophakic retinal detachment indicates strong vitreoretinal adhesions. Acta Ophthalmologica. 2015;93(8):e687-e688.
13. Yonemoto J, Ideta H, Sasaki K, Tanaka S, Hirose A, Oka C. The age of onset of posterior vitreous detachment. Graefes Arch Clin Exp Ophthalmol. 1994;232(2):67-70.
14. Itakura H, Kishi S, Li D, Nitta K, Akiyama H. Vitreous changes in high myopia observed by swept-source optical coherence tomography. Invest Ophthalmol Vis Sci. 2014;55(3):1447-1452.
15. Mirshahi A, Hohn F, Lorenz K, Hattenbach LO. Incidence of posterior vitreous detachment after cataract surgery. J Cataract Refract Surg. 2009;35(6):987-991.
16. Ivastinovic D, Schwab C, Borkenstein A, Lackner EM, Wedrich A, Velikay-Parel M. Evolution of early changes at the vitreoretinal interface after cataract surgery determined by optical coherence tomography and ultrasonography. Am J Ophthalmol. 2012;153(4):705-709.
17. Hilford D, Hilford M, Mathew A, Polkinghorne PJ. Posterior vitreous detachment following cataract surgery. Eye. 2009;23(6):1388-1392.
18. Ripandelli G, Coppe AM, Parisi V, et al. Posterior vitreous detachment and retinal detachment after cataract surgery. Ophthalmology. 2007;114(4):692-697.
