

In order to discuss the current status of multifocal IOL use and the correction of presbyopia in Europe, we first must consider how the needs and demands of our patients have changed in recent years. Cataract surgery used to address only patients’ distance visual acuity, and it was assumed that near vision would require reading glasses. Now, increasingly sophisticated patients understand that, in many cases, their near and intermediate visual needs can also be addressed at the time of cataract surgery.
Patients’ needs and demands vary widely, depending on whether they more highly value reading or performing tasks at intermediate distances, such as computer use, hobbies, or other activities. With the increasing popularity of refractive surgery and the proliferation of information available on the Internet, many patients expect to achieve excellent unaided visual acuity at all distances after cataract surgery. This affects how we define, discuss, and test visual acuity: What is near acuity, what is intermediate acuity, and what is distance acuity? What are acceptable postoperative levels of visual acuity at these distances in 2015? Is 20/20 and J4 still good enough, or do we have to do better?
Many types of multifocal IOLs on the market aim to address these issues: refractive, asymmetric refractive, diffractive, apodized diffractive, multifocal toric, high adds, low adds, refractive trifocal, diffractive trifocal toric. The variations continue to proliferate.
The current trend is to emphasize intermediate vision, with the use of low adds or a trifocal optical approach. The ideal today seems to be to boost visual performance in the intermediate range so that it better matches the near and distance performances, thereby changing the defocus curve from a deep valley to a more even performance over a broad range of diopters (Figure 1).
It is not easy to obtain data for IOL use in all of Europe. This article examines current trends in multifocal IOL use in Europe through the lens of the German-speaking market. (The German-speaking countries represent approximately 30% of the total European IOL market.) The German-Speaking Society for Intraocular Lens Implantation and Refractive Surgery (Deutschsprachige Gesellschaft für Intraokularlinsen-Implantation, Interventionelle, und Refraktive Chirurgie; DGII) conducts an annual survey that can provide some insights in this area. Information in this article is taken from the 2013 DGII survey.1
THE GERMAN MEDICAL MARKET
Multifocal IOLs are implanted not only in cataract surgery but also in refractive lens exchange, so a combination of national health insurance and private pay is involved in the economy of their use. This is true not only in Germany but in many countries in Europe. In general, public reimbursement rates are high in Germany in comparison with other European countries.
There is also a high degree of diversity of medical spending regionally within Germany, depending on the culture and buying power of the population, with, in general, lower levels of expenditure in the East. This is mirrored to a degree in Europe as a whole, with lower levels of income and expenditure in the newer countries in the East than in the West.
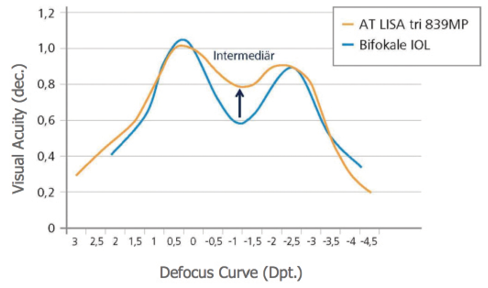
Figure 1. Monocular defocus curve of the AT LISA tri versus a bifocal IOL: The trifocal IOL boosts visual performance in the intermediate range, changing the defocus curve from a deep valley to a more even curve.
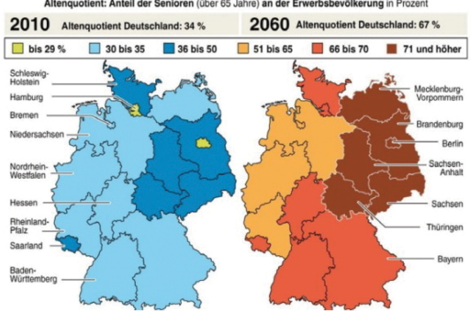
Figure 2. The aging quotient: The number of people residing in Germany who are over the age of 65 years is rising.
The medical insurance system in Germany is organized on a regional basis. The insurance company in a given region collects payments from patients in that region every month, so there are different reimbursement levels depending on the economics and politics of each region. For surgeons, this means cataract surgery is reimbursed at a higher level in some areas of the country than others. For patients, this system has an impact on whether they can afford to buy a multifocal IOL through a copayment route, depending on where they live. Also, the exposure of a surgeon to this kind of market is different, depending on whether he or she has a lot of patients who can afford a premium IOL or not.
In Germany, there is a generally high acceptance of ophthalmic products from the international brands, but there are also strong domestic brands that produce high-quality IOLs and other products. In contrast, some other European countries have no domestic companies that produce multifocal IOLs.
THE AGING QUOTIENT
The older the population gets, the more presbyopia there is, and the more cataract patients we have. This is the aging quotient. In Germany in 2010, 34% of people were over age 65 years. By 2060, this number will be almost 70% (Figure 2). But, again, the distribution of older people will vary regionally. For example, many people in the eastern part of Germany will be very old, whereas fewer will be in other parts of the country.
However, as noted above, the East has less money to spend on medical insurance. This may present a challenge for delivery of adequate health care to the elderly in this area of the country.
We also have to consider not only our own little area of cataract surgery, but also the increase in expenditures for other age-related eye diseases such as age-related macular degeneration and diabetic retinopathy, not to mention age-related systemic diseases. This will translate to less money for cataract surgery.
Another consideration is the number of people who are working and contributing to the health systems. The percentage of the population that is of working age is quite high now, but it will decline by about one-third in the next 30 years. The fewer people working, the less money will be in the health care system. I postulate that, 20 years from now, we may get 20% or 30% less reimbursement than we currently get for a cataract surgery procedure.
THE PRESBYOPIC MARKET
All of these factors will have an impact on the presbyopic market. Among the members of the DGII at the present time, around 800,000 IOL procedures are performed per year, with an expected annual growth rate of 6% for the coming years.
There are only a relatively small number of surgeon members of the DGII—about 200—who offer premium IOLs, compared with 6,000 to 7,000 conservative ophthalmologists who do not offer these lenses. (Germany does not have optometrists. In some parts of Europe, conservative ophthalmologists would be called optometrists.) Cataract surgeons are high-volume surgeons; 64% of them reported performing more than 1,000 cases per year in the 2013 DGII annual survey.
Most cataract patients are referred by nonsurgical, conservative ophthalmologists to eye clinics or surgical centers; follow-up is also performed by the referring ophthalmologist. Therefore, there is a big market for cataract surgery, but there is a small target group of people performing the surgeries.
Most of these surgeons, who may be performing 1,000 to 1,500 cataract surgeries per year, do not want 20 options of multifocal IOL. They do not have the chair time to spend with patients explaining all those options. They want to have one solution—one lens, at one price—that will cover a range of options for their patients.
Therefore, if you ask a rank-and-file ophthalmologist what he or she wants in a multifocal IOL, you may get a different answer than you would get from the so-called key opinion leaders who can compare and contrast the characteristics of a dozen multifocal options. Most ophthalmologists in Germany and elsewhere in Europe want a trusted brand and a reliable product that can deliver good results in a high-volume situation.
At a Glance
• The current trend in multifocal IOLs is to emphasize intermediate vision, with the use of low adds or a trifocal optical approach.
• The increase in expenditures for other age-related diseases such as age-related macular degeneration, diabetic retinopathy, and age-related systemic diseases will leave less money for cataract surgery.
• Most ophthalmologists want a trusted brand and a reliable product that can deliver good results in a high-volume situation.
CURRENT, FUTURE USE OF MULTIFOCALS
Some historical data can help to set the stage for where the multifocal IOL market is going. In 2008, in Western Europe, 2.8 million IOLs were implanted. Of these, about 90,000 were presbyopia-correcting IOLs, representing roughly 3.2% of the total. The percentage of presbyopia-correcting IOLs used in Germany was low—about 1.5%, in comparison with Spain, where usage was 7%. According to Market Scope, worldwide, the percentage of presbyopia-correcting IOLs in relation to total IOLs implanted was 2.5%; in the United States, it was 6%.
Since that time, the uptake of premium IOLs has increased. This is partially due to improvements in technology and also because of changes in the law. In the European Union, particularly in Germany, patient copayment for premium IOLs in now allowed (see What’s the Deal With Copayments for Premium Lenses?, pg 46).
In 2013, of a total 370,000 surgeries reported in the DGII survey, about 8,000 of these involved multifocal IOLs. Also, about 9,000 toric IOLs and 120,000 aspheric IOLs were reported in this evaluation. When all premium lenses are considered, the percentage in relation to total IOL implantations is more than 5% in Germany, although still well below 10%. This same trend can be extrapolated somewhat to the overall European market.
The factors influencing this increase in utilization of premium IOLs include the changes in national regulations affecting reimbursement and copayments for these devices and the increased awareness among surgeons, referring doctors, and patients about these technologies. There are no real incentives toward increased utilization for the implanting surgeon or the referring physician. If the surgeon or referring physician “sells” a patient on the utility of a particular premium IOL, it is the manufacturer that gets the money. There is no way to add to the physician fees for a normal public health insurance patient.
Although usage of multifocal IOLs is increasing, there are competing technologies that can be said to cannibalize the presbyopia-correction market. We have already mentioned the plethora of styles and models of presbyopia-correcting IOLs that compete with one another. Add to this the possibility of monovision correction and the various add-on or supplemental multifocal IOL options. Now, in addition, there are extended range of vision and extended depth of focus IOLs, and the marketing for some of these devices suggests that they are better than multifocal IOLs because they do not carry the potential complications of glare and halos. The logical conclusion of this line of reasoning is that multifocal IOLs are bad, and therefore we cannibalize our own market. We must be careful about how we market new technologies.
In addition to IOL options, there are non-IOL approaches to presbyopia correction. These include various excimer laser treatment approaches such as presby-LASIK and monovision LASIK; intrastromal corneal inlays; and femtosecond laser intrastromal procedures.
CONCLUSION
In summary, then, there is a growing market for presbyopia correction, but that growth is limited. Awareness and acceptance of multifocal IOLs and other presbyopia-correcting technologies are increasing, but advancement is slow. The Eastern European markets may catch up with the West and add to the overall growth of the market, but there are still many influencing factors that will restrict the growth of multifocal IOL use in our part of the world. There is a lot of work to be done to give multifocal IOLs the position in the overall market that they deserve. n
1. Annual Survey of DGII and BVA for the current status of cataract and refractive surgery. Published survey results [in German]. http://www.dgii.org/en/dgii-surveys-166.html. Accessed July 27, 2015.
Gerd U. Auffarth, MD, PhD
• Chairman, Department of Ophthalmology, University of Heidelberg, Germany
• Director, International Vision Correction Research Center & David J. Apple Laboratory for Ocular Pathology, Heidelberg, Germany
• auffarthg@aol.com
• Financial disclosure: None