

With advances in technology including femtosecond laser incisions and premium IOLs, there is little doubt that we practice in an era of refractive cataract surgery. However, surgeons often overlook the fact that these advantages can be lost with the slightest disruption of the tear film. Ocular surface disease (OSD) is exceedingly common in the cataract-age population, and the presence and exacerbation of OSD can negatively affect IOL calculations and postoperative visual quality.
Despite impeccable surgical technique and in the face of soaring patient expectations, postoperative dry eye disease (DED) is the most common and potentially distressful complication of cataract surgery today. This article outlines five fundamentals that can help to maximize the outcomes of cataract surgery in patients with OSD.
Fundamental #1 - Identify the magnitude, impact of OSD on cataract surgery
Studies suggest that the prevalence of asymptomatic DED is high in cataract patients and that cataract surgery can induce or exacerbate existing DED.1 The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study found that 87% of patients with dry eye were asymptomatic.2 However, more than 60% had a tear breakup time (TBUT) of less than 5 seconds, 50% had central corneal staining, and 21.3% had a very low Schirmer test value.
In a similar study of 200 eyes of 100 patients scheduled for cataract surgery, 59% had blepharitis, although a majority were asymptomatic. It is imperative to identify and treat aqueous-deficient or evaporative DED prior to surgery, as these conditions can adversely affect IOL calculations, toric IOL axis and magnitude estimations, and the outcomes of limbal relaxing incisions due to inaccurate keratometry and topography measurements. If they are not addressed in timely manner, tear film abnormalities can also slow down healing and delay visual recovery, thereby reducing patient satisfaction, particularly in patients undergoing premium IOL surgery.
OSD is far more common in the aging cataract population than is generally believed. Apart from DED, herpetic eye disease, chemical injuries, and immunologically driven OSD—including Sjögren syndrome, atopy, Mooren’s ulcer, Stevens-Johnson syndrome, and ocular cicatricial pemphigoid—can also affect this group of susceptible individuals. It is crucial that surgeons have a high index of suspicion for ocular surface disorders and initiate treatment well in advance of any surgical intervention.
Fundamental #2 - Perform a thorough preoperative assessment
Cataract surgeons need to place a great deal of emphasis on screening for OSD before surgery. Taking a thorough patient history and performing careful evaluation of the eye and ocular adnexa are central to the appropriate diagnosis and treatment of OSD. Vision that worsens with activity either before or after cataract surgery is almost always a sign of tear film insufficiency.3 A history of systemic collagen disease, vascular disease, or associated manifestations such as arthritis or dry mouth provides important clues for the possibility of concomitant OSD.4
At a Glance
• Because cataract surgery is a surface-damaging event, it is important to nurture the ocular surface in patients in both the pre- and postoperative periods.
• Ocular surface preparation can be beneficial not only in patients with established OSD but also in those with minimal signs or symptoms of OSD.
• Surgeons should identify patients who are at risk for exacerbation of OSD, optimize tear film stability preoperatively, minimize intraoperative dry eye with an appropriate surgical plan, maximize outcomes with aggressive postoperative management to restore surface integrity, and try to ensure long-term maintenance of the ocular surface.
A detailed slit-lamp examination should be performed to look for lack of corneal or conjunctival luster, reduced tear meniscus height, tear film debris, scarring, filaments, epithelial basement membrane dystrophy, poor meibomian gland morphology, and eyelid pathology. Vital dye staining of the ocular surface is an important component of the initial examination (Figure 1). Staining with vital dyes such as lissamine green or sodium fluorescein, TBUT testing, and Schirmer testing with anesthetic are important ways to quantify OSD.5 The combination of a tear meniscus height of less than 0.25 mm and a TBUT of less than 5 seconds indicates DED with high sensitivity and specificity.
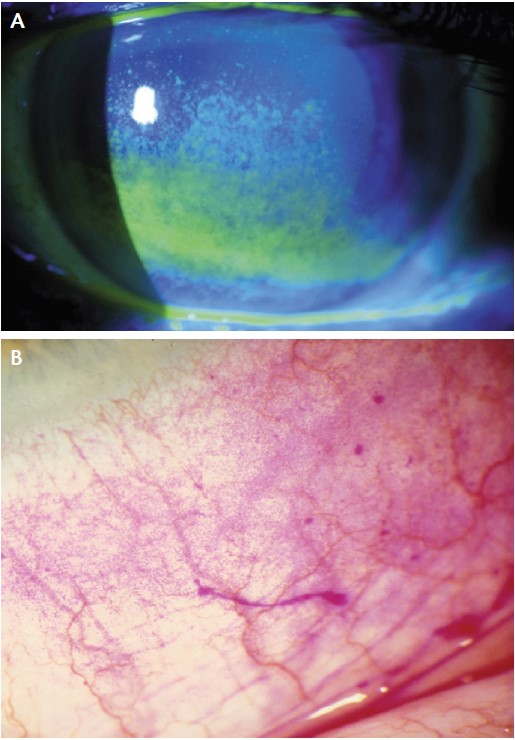
Figure 1. Fluorescein staining of the corneal epithelium (A). Rose bengal staining of the conjunctival epithelium (B).
DED can now also be assessed using noninvasive tests such as tear osmolarity analysis (TearLab Osmolarity System; TearLab), detection of tear matrix metalloproteinase 9 (Inflammadry; Rapid Pathogen Screening), lipid layer interferometry (Lipiview; TearScience), wavefront aberrometry, and noncontact topography-based TBUT (Keratography 5; Oculus Optikgeräte).
The ocular surface stress test described by Hardten can be used to identify patients who are at high risk for developing DED after phacoemulsification. If a patient examined 30 to 60 minutes after instillation of topical anesthetic and dilating drops shows an irregular corneal epithelium, this is a clear indicator of poor epithelial integrity.6
Corneal topography is an invaluable screening tool in patients with unstable tear films. Topography maps with areas of missing data are indicators of tear film disturbances. These dropout spots can be eliminated with treatment prior to surgery. Dry eye can also result in induced astigmatism, which can affect IOL calculations.
Further, any indication of immunologically driven OSD must be thoroughly investigated prior to surgery.
Fundamental #3 - Optimize the ocular surface in the preoperative period
Management of OSD may be accomplished by following established guidelines and recomendations.7 Using a systematic approach, treatment should begin with tear supplements, which have been shown to diminish ocular signs and symptoms of DED in a majority of cataract surgery patients.
Antiinflammatory agents play an important role in the treatment of moderate to severe inflammatory dry eye.8,9 A short course of topical steroids for rapid recovery of tear film stability, followed by topical cyclosporine 0.05% for a longer duration, has been shown to improve postoperative visual outcomes.10
The presence of blepharitis is often the reason for cancelling cataract surgery, as it is thought to be a primary risk factor for endophthalmitis.11 In patients with meibomian gland dysfunction and blepharitis, hot compresses, lid hygiene, topical azithromycin, and oral omega-3 fatty acid supplements have demonstrated effective reduction of ocular surface morbidity. If OSD goes untreated before cataract surgery, it is likely to result in patient dissatisfaction and, although rarely, may be implicated in postoperative infections. This is especially important in patients with moderate to severe OSD, who are at increased risk for complications, most notably corneal melting, in the postoperative period.
Optimization of the ocular surface before cataract surgery is imperative in patients with immune-mediated OSD. In the presence of active blepharitis, meibomitis, or conjunctivitis, it is recommended that lid and conjunctival swab cultures be taken 2 weeks before surgery and that appropriate topical antibiotic therapy be commenced 7 days before surgery. This is important, as surgery in the inactive stage of any immune disease has a better prognosis than surgery during the active stage. A quiet eye facilitates uneventful surgery and is less susceptible to the recurrence of inflammation, persistent epithelial defects, perioperative corneoscleral melts, and endophthalmitis. Cataract surgery in patients with ocular mucous membrane pemphigoid requires controlling the disease for a minimum of 1 year.12 Systemic steroids and immunosuppressive drugs are highly recommended in the perioperative period in patients with any immune-mediated OSD.13
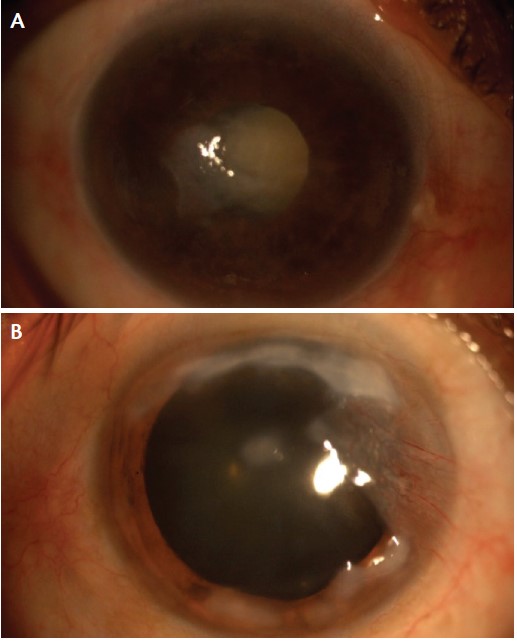
Figure 2. Cataractous eye with epithelial hyperplasia and scarring (A). Salzmann nodular degeneration with pterygium (B).
Fundamental #4 - Adopt intraoperative measures to ensure safe surgery
During surgery, the ocular surface is prone to damage from prolonged exposure and from eye drops containing preservatives. Frequent irrigation with balanced saline solution or the use of a dispersive OVD can minimize desiccation of the ocular surface and enhance the surgeon’s view during surgery. Kasetsuwan et al14 suggested that the use of light filters, decreased exposure time, proper irrigation, and gentle manipulation of the ocular surface tissue may reduce complications after surgery.
Clear corneal incisions are recommended, despite damage caused by the disruption of corneal nerves.15,16 Temporal clear corneal incisions also offer easy access in some difficult eyes. It is best to limit conjunctival manipulation in eyes with inflammatory OSD to avoid postoperative recurrences and melts. If a scleral incision is planned, additional immunosuppressive therapy will be needed during the perioperative period.17
A compromised view during surgery due to surface irregularities or preexisting corneal scarring (Figure 2) can be satisfactorily overcome with the use of trypan blue or endoillumination or by adjusting the angle of the microscope light. Paraxial illumination provides a better view compared with coaxial illumination. In a prospective study,18 the use of an aspirating speculum was found to worsen DED-related parameters, such as conjunctival staining, TBUT, conjunctivochalasis grade, and Ocular Surface Disease Index score during the early postoperative period.18 Topical anesthestics should be unpreserved. General anesthesia may be necessary in patients with short fornices, symblephara, or adhesions, in order to facilitate lid retraction sutures and canthotomies. Appropriate head positioning and use of a wick can minimize pooling of fluid in eyes with contracted apertures.
In eyes with extensive corneal scarring, cataract extraction is easier through a scleral tunnel. Subconjunctival injections should be avoided, as they may reactivate conjunctival inflammation.
Fundamental #5 - Aim postoperative care toward maximizing outcomes
Because DED is complex and multifactorial, maintaining a healthy ocular surface postoperatively is a growing challenge. The signs and symptoms of OSD typically get worse after cataract surgery, owing to the prolonged use of postoperative medications that contain preservatives. Other contributing factors include disruption of the corneal nerves and postoperative inflammation. Therefore, in patients with OSD, it is prudent to use preservative-free topical medications in limited dosages and for as short a duration as possible.
Topical NSAIDs such as nepafenac, ketorolac, and diclofenac have been reported to cause corneal melting in patients with significant OSD, mainly in the presence of epithelial breakdown.19 Concomitant use of topical steroids with NSAIDs may reduce, if not prevent, this complication. Careful postoperative follow-up is necessary to identify and treat indolent perioperative epithelial defects (Figure 3) and excessive conjunctival inflammation.20 Sterile corneal melts have been reported in patients with immune-mediated OSD, such as Sjögren syndrome, graft-versus-host disease, and Stevens-Johnson syndrome.21
The severity of postoperative DED may peak on day 7 and can last for 3 months or longer. Hence, the ocular surface must be actively rehabilitated postoperatively. Accumulating data suggest the efficacy of a combination of topical lubricants and topical cyclosporine for long-term ocular surface maintenance. Cyclosporine 0.05% therapy twice daily for 3 months has been reported to reduce dry eye signs and improve visual quality after cataract surgery. Studies indicate that pre- and postoperative therapy with topical cyclosporine 0.05% helps alleviate dry eye signs, improve visual outcomes, and enhance the satisfaction of patients undergoing cataract surgery with multifocal IOL implantation.10 The improved quality of tears with cyclosporine use may result in a more regular ocular surface and alleviate negative symptoms associated with multifocal IOL implantation. Additionally, mechanical blockage with punctal plugs and continued management of evaporative DED may help achieve long-term rehabilitation of the surgically violated ocular surface.
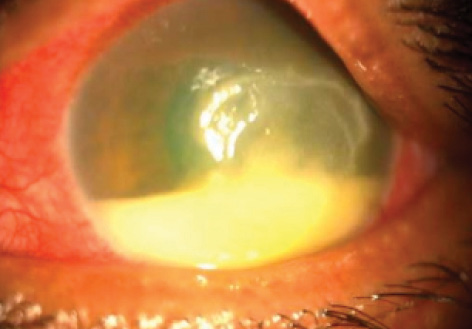
Figure 3. Postoperative persistent epithelial defect with secondary infection.
CONCLUSION
OSD is more prevalent than is commonly perceived. Maintenance of a pristine ocular surface can play a major role in achieving good visual outcomes after cataract surgery. Given that cataract surgery is a surface-damaging event, it is important to nurture the ocular surface in patients in both the pre- and postoperative periods. Ocular surface preparation can be beneficial not only in patients with established OSD but also in those with minimal signs or symptoms of surface disease. n
1. The epidemiology of dry eye disease: report of the Epidemiology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):93-107.
2. Trattler W, Goldberg D, Reilly C. Incidence of concomitant cataract and dry eye: prospective health assessment of cataract patients. Paper presented at: The World Cornea Congress; April 8, 2010; Boston, MA.
3. Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol. 2009;23:65-73.
4. Li XM, Hu L, Hu J, Wang W. Clinical observation of dry eye in patients before and after cataract surgery. Zhonghua Yan Ke Za Zhi. 2007;43:10-13.
5. Roberts CW, Elie ER. Dry eye symptoms following cataract surgery. Insight. 2007;32:14-21.
6. Hardten DR. Dry eye disease in patients after cataract surgery. Cornea. 2008;27:855.
7. Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):163-178.
8. Pflugfelder SC. Antiinflammatory therapy for dry eye. Am J Ophthalmol. 2004;137:337-342.
9. Pflugfelder SC, De Paiva CS, Villarreal AL, Stern ME. Effects of sequential artificial tear and cyclosporine emulsion therapy on conjunctival goblet cell density and transforming growth factor-beta2 production. Cornea. 2008;27:64-69.
10. Donnenfeld ED, Solomon R, Roberts CW, et al. Cyclosporine 0.05% to improve visual outcomes after multifocal intraocular lens implantation. J Cataract Refract Surg. 2010;36:1095-1100.
11. Speaker MG, Milch FA, Shah MK, et al. The role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis. Ophthalmology. 1991;98:639-649.
12. Saw VP, Dart JK. Ocular mucous membrane pemphigoid: diagnosis and management strategies. Ocul Surf. 2008;6(3):128-142.
13. Sangwan VS, Burman S. Cataract surgery in Stevens Johnson syndrome. J Cataract Refract Surg. 2005;31:860-862.
14. Kasetsuwan N1, Satitpitakul V, Changul T, Jariyakosol S. Incidence and pattern of dry eye after cataract surgery. PLoS One. 2013;8(11):e78657.
15. John T. Corneal sensation after small incision, sutureless, one-handed phacoemulsification. J Cataract Refract Surg. 1995;21:425-428.
16. Kohlhaas M, Stahlhut O, Tholuck J, Richard G. Development of corneal sensitivity after phacoemulsification with scleral tunnel incision. Klin Monbl Augenheilkd. 1997;211:32-36.
17. Perez VL, Azar DT, Foster CS. Sterile corneal melting and necrotizing scleritis after cataract surgery in patients with rheumatoid arthritis and collagen vascular disease. Semin Ophthalmol. 2002;17:124-130.
18. Moon H, Yoon JH, Hyun SH. Short-term influence of aspirating speculum use on dry eye after cataract surgery: a prospective study. Cornea. 2014;33(4):373-375.
19. Wolf EJ, Kleiman LZ, Schrier A. Nepafenac-associated corneal melt. J Cataract Refract Surg. 2007;33:1974-1975.
20. Movahedan A, Djalilian AR. Cataract surgery in the face of ocular surface disease. Curr Opin Ophthalmol. 2012;23:68-82.
21. Speaker MG, Milch FA, Shah MK, et al. The role of external bacterial flora in the pathogenesis of acute post-operative endophthalmitis. Ophthalmology. 1991;98:639-649.
Sanghamitra Burman, MD, FRCS
• Consultant Cornea, Cataract, and Refractive Surgeon, Vasan Eye Care Hospitals, Bangalore, India
• drsanghamitrab@yahoo.co.uk
• Financial disclosure: None
