


Since the introduction of the original endocapsular device in 1991, there has been a progressive evolution of designs to help surgeons manage profound zonular weakness. Standard capsular tension rings (CTRs) may be useful in eyes with mild zonular instability such as small, localized zonular dialysis or mild diffuse zonular weakness. However, a standard CTR may not supply sufficient support to maintain the capsular bag in situations of profound or progressive zonular insufficiency, such as advanced pseudoexfoliation syndrome or Marfan syndrome. Further, in the setting of an anterior or posterior capsular tear, the risks of tear extension or loss of the device into the posterior segment limit the use of a standard CTR.1,2
With the advent of sclerally fixated devices such as modified CTRs and capsular tension segments (CTSs), adequate intraoperative or postoperative support can be achieved in eyes with profound zonular weakness. Additionally, these suturable endocapsular devices may be of optimal value in eyes with progressive zonulopathy, as they can be secured to the sclera. Further support can be achieved by combining devices.
A CTS can be implanted without a dialing technique; therefore, these devices may be useful in eyes with an incomplete rhexis, anterior capsular tear, or posterior capsular tear. As it provides support in the transverse plane when sutured to the sclera, a CTS may be used temporarily to provide intraoperative support of the capsule in an area of zonular weakness. In this situation, it can be hung from an inverted iris retractor placed through the eyelet of the CTS.1,2
Despite the advantages and utility of modified CTRs and CTSs, in Korea we have limited access to these devices due to the use of a diagnosis related group/prospective payment system and to lack of approvals by our country’s regulatory body. Therefore, we have devised and performed alternative methods of stabilizing the capsule and IOL in eyes with large zonular dialysis of more than 4 clock hours and progressive zonulysis.
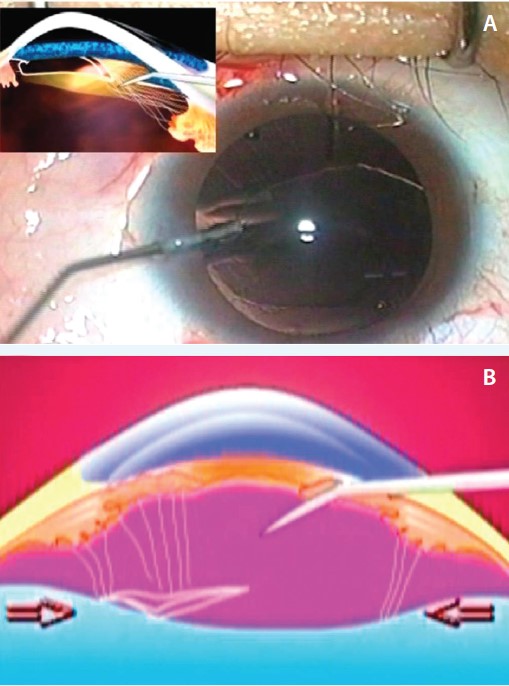
Figure 1. Transscleral IOL fixation with preservation of the anterior vitreous in the treatment of ectopia lentis in a patient with Marfan syndrome. An OVD is injected through the loose zonules to separate the posterior capsule from the anterior vitreous face (A). Because residual zonules and capsular remnants indicate the level of the anterior vitreous face (arrows), a needle can be passed across the anterior chamber to the ciliary sulcus on the opposite side without breaking the anterior vitreous face (B).
ALTERNATIVES TO SUTURED ENDOCAPSULAR DEVICES
Progressive severe zonulopathy: Marfan syndrome. Marfan syndrome is the most frequent congenital cause of ectopia lentis, which occurs in 80% to 90% of affected individuals. Zonular dialysis is known to be progressive and profound in this condition. In patients with mild to moderate lens subluxation, a CTR can be employed. However, posterior capsular opacification (PCO) and late IOL dislocation secondary to progressive fibrous adhesions between the zonular and capsular complexes can occur at a later date.
To manage severe lens subluxation, an IOL can be sutured to the scleral wall after intracapsular cataract extraction or pars plana lensectomy. However, postoperative vitreoretinal complications and severe astigmatism are known complications after such surgery. Therefore, we proposed a novel surgical technique in which the lens is removed through a small incision, without breaking the anterior vitreous face, and an IOL is sutured to the sclera.3
In this technique, after formation of two fornix-based conjunctival incisions at the 6- and 12-o’clock positions, half-thickness triangular scleral flaps are constructed 180° apart. A stab incision and a limbal incision of 2.8 mm are made in the quadrant where the zonules are intact. Using a bent needle, a puncture is made on the surface of the anterior capsule in the quadrant of the intact zonules. The capsulorrhexis is completed using capsulorrhexis forceps. Complete hydrodissection and hydrodelineation are then performed to minimize potential zonular damage during manipulation of the lens. Phacoemulsification and/or aspiration are performed with low bottle height and low vacuum settings.
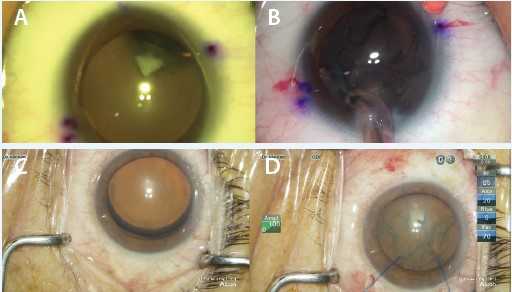
Figure 2. Iris retractors can be placed at the capsulorrhexis edge over the area of zonular weakness or defect to stabilize a loose capsular-zonular complex during surgery. Case examples: A zonular defect associated with lens coloboma was detected (A), and iris retractors were used to bridge the gap effectively and prevent vitreous prolapse through the zonular defect during surgery (B). Profound zonular dialysis and lens dislocation after blunt trauma was observed (C), and iris retractors could have been used to stabilize the capsularlens complex during the entire operation (D).
After complete removal of the lens material, a cohesive OVD is injected through the loose zonules behind the capsular bag to separate the posterior capsule from the anterior vitreous face (Figure 1A). A bent needle is used to create a puncture in the posterior capsule; intraocular scissors and capsulorrhexis forceps are then employed to remove the central part of the capsule.
In the process of pushing the vitreous face using OVD, the remaining elongated zonules and capsular remnants indicate the level of the vitreous face. A PC-7 needle (Alcon) is passed through the limbal incision, across the chamber, and above the vitreous face toward the ciliary sulcus at the 6-o’clock position under the scleral flap (Figure 1B). The location of the needle can be detected by elevation of the sclera as the needle tip is gently pushed toward the outside.
The needle is next passed to the exterior. The haptic of the IOL is sutured to the other end of the needle and then inserted into the anterior chamber. The trailing haptic is sutured to the other end of a PC-7 needle, and the needle sutures under the flap at the 12-o’clock position. Scleral and limbal incisions are secured with 10-0 nylon sutures, and scleral flaps and conjunctival incisions are closed with 10-0 nylon sutures.
Nonprogressive zonulopathy: congenital lens coloboma and traumatic crystalline lens dislocation. Zonulopathy in eyes with congenital lens coloboma and traumatic crystalline lens dislocation is known to be nonprogressive, although the amount of zonular defect or weakness varies according to disease entity and severity. These patients may be good candidates for the use of iris retractors instead of endocapsular devices.
At a Glance
• A standard CTR may not supply sufficient support in cases of profound or progressive zonular insufficiency such as advanced pseudoexfoliation or Marfan syndromes.
• Scleral fixation of a modified CTR or CTS can help to provide adequate intra- or postoperative support in eyes with profound zonular weakness.
• If a modified CTR or CTS is unavailable, alternative techniques can be used to successfully manage progressive and nonprogressive zonulopathy.
• One alternative technique is to remove the lens through a small incision, without breaking the anterior vitreous face, and suture an IOL to the sclera.
Iris retractors can be placed at the capsulorrhexis edge over the area of zonular weakness or defect to stabilize the loose capsular-zonular complex during surgery (Figure 2). However, close attention should be paid to the risk of inadvertent dislodging of the iris retractor and resultant anterior capsular tear. To reduce these risks when working with iris retractors, an adequately sized capsulorrhexis is of utmost importance. If the capsulorrhexis margin is small, the hook may drag on the capsulorrhexis edge and result in a capsular tear or dislodging of the hook.
Another strategy to minimize the risk of capsular tears is to use the iris retractor to hook the anterior capsule and the iris together. The iris stroma can be the buttress for the tension on the capsule by the tip of the retractor and, consequently, lessen the risk of capsular tears or dislodging of the retractor. An important factor in maintaining a stable position of the retractor is the location of the paracentesis used for its insertion. A paracentesis made near the limbus may be more advantageous for the iris retractor to be parallel to the iris plane and therefore maximize the stability of the retractor compared with one made far from the limbus (Figure 3).
After the lens is removed using retractors, a loose capsular-zonular complex can be stabilized by in-the-bag implantation of an IOL with rigid haptics, such as three-piece IOLs with acrylic or silicone optics and PMMA haptics. In eyes with a localized zonular defect, we prefer that the IOL haptics be oriented toward the zonular dialysis. The haptics can thus expand the capsular equator and buttress the weak area in a similar way to an endocapsular device. For larger defects, by contrast, orientation of the haptics toward intact zonules is more advantageous because this can help maintain healthy zonules in the event of late capsular contracture.
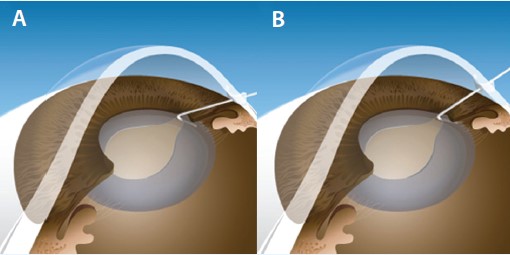
Figure 3. Possible positions of an iris retractor according to insertion site are shown. A paracentesis made near the limbus may be more advantageous for the iris retractor to be parallel to the iris plane (A), thereby maximizing the stability of the retractor, compared with one made far from the limbus (B).
risk of late IOL dislocation
Despite these steps, larger zonular defects still carry the risk of late in-the-bag dislocation. However, IOL dislocation can be treated by repositioning the dislocated lens using scleral or iris fixation.
Although IOL fixation to the iris has the advantage of requiring a shorter operation time, it also has several drawbacks, including increased rates of induced astigmatism, less stable refraction, and immediate and recurring postoperative inflammation.4 Therefore, scleral fixation is our preference in the event of in-the-bag IOL dislocation.
Additionally, we incorporate primary posterior continuous curvilinear capsulorrhexis creation during the operation in eyes with zonular dialysis in an attempt to minimize the risk of late capsular instability. The use of a posterior continuous curvilinear capsulorrhexis in cataract surgery can improve postoperative refractive stability by reducing IOL displacement during postoperative capsular bag fibrosis and shrinkage.5
CONCLUSION
In the setting of profound or progressive zonular weakness, scleral-fixated endocapsular devices such as modified CTRs or CTSs can provide adequate support for the capsule intraoperatively and postoperatively. However, when these devices are unavailable, other techniques can be used to successfully manage challenging cases of progressive and nonprogressive zonulopathy. n
1. Hasanee K, Butler M, Ahmed, II. Capsular tension rings and related devices: current concepts. Curr Opin Ophthalmol. 2006;17(1):31-41.
2. Weber CH, Cionni RJ. All about capsular tension rings. Curr Opin Ophthalmol. 2015;26(1):10-15.
3. Kim WS. Transscleral intraocular lens fixation with preservation of the anterior vitreous face in patients with Marfan syndrome and ectopia lentis. Cornea. 2010;29 Suppl 1:S20-24.
4. Kim KH, Kim WS. Comparison of clinical outcomes of iris fixation and scleral fixation as treatment for intraocular lens dislocation. Am J Ophthalmol. 2015;160(3):463-469.
5. Kim KH, Kim WS. Intraocular lens stability and refractive outcomes after cataract surgery using primary posterior continuous curvilinear capsulorrhexis. Ophthalmology. 2010;117(12):2278-2286.
Kyeong Hwan Kim, MD
• Assistant Professor, Department of Ophthalmology, Haeundae Paik Hospital, Busan, South Korea
• Assistant Professor, Department of Ophthalmology, Inje University College of Medicine, Busan, South Korea
• khkim@inje.ac.kr
• Financial disclosure: None acknowledged
Wan Soo Kim, MD, PhD
• Chairman and Professor, Department of Ophthalmology, Haeundae Paik Hospital, Busan, South Korea
• Chairman and Professor, Department of Ophthalmology, Inje University College of Medicine, Busan, South Korea
• wansookim@paik.ac.kr
• Financial disclosure: None acknowledged
