

All medical specialties and subspecialties have experienced cuts in reimbursement, but the reduction in the remuneration for refractive surgery—a group of procedures that has continually improved since the 1980s—seems onerous. The main reason for the cutbacks is that, around the world, government reimbursement for refractive surgery is either very low or nonexistent. In Europe, the wide disparity in techniques and rates charged from one refractive laser center to another may also be an important factor in the seemingly low level of reimbursement.
UNREGULATED PRICING AND UNCLEAR ECONOMIC MODELS
AT A GLANCE
• In deciding how to model their practices, physicians must focus on growth and value, their years in practice, their costs, and their expected return on investment.
• Offering low-cost surgery can damage one’s personal brand and product image; high rates must be associated with services that provide the distinctive and effective benefits expected by consumers.
• In order to compete against low-cost providers, practices must invest their intangible capital—the good name and reputation of the surgeon—and maximize flexibility for patients.
• Premium practices should expect to constantly offer innovative methodologies and technological breakthroughs.
In France, the country where I practice, the medical profession has an aversion to guardianship and economic management of medical care. Conversely, physicians attempt to fully maximize their profits through the remuneration systems available. The social health care system is free of charge for patients in the case of pathologic disease, but there is no reimbursement to patients for elective, nonmedically necessary care such as plastic surgery and refractive surgery.
In Europe, elective refractive surgery is unregulated in terms of price. Few surgeons have a clear and concise economic model for refractive surgery. The common trend for patients is to search for the most promising offerings without too much expense. Few surgeons have a full-time refractive surgery practice, with most also practicing anterior segment surgery. Such a setup does not allow these surgeons to spend time optimizing their refractive surgery offerings because most of their income comes from cataract surgery and other government-reimbursed procedures. In most European countries, ophthalmologists earn a sufficient living just through the public health system. As a result, refractive surgery is a complementary specialty for 95% of refractive surgeons.
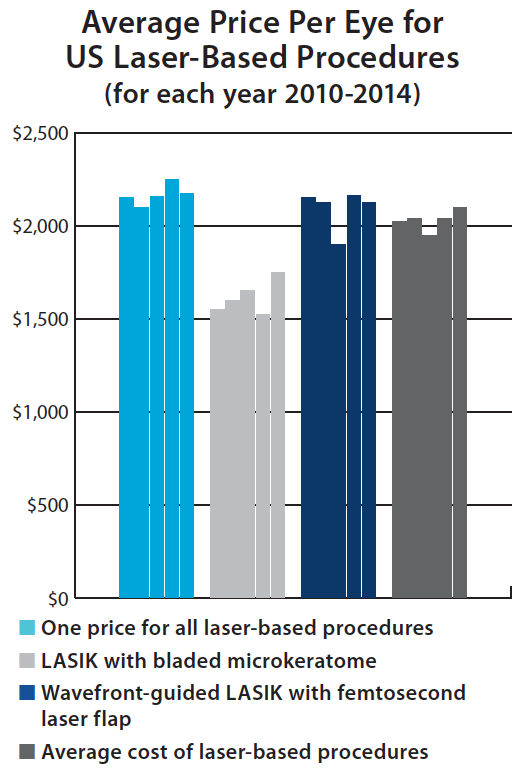
Figure 1. Prices have remained fairly flat in these four categories from 2010 through 2014.
It would seem, however, that the ability to bill beyond the extent of social insurance should attract practitioners, with the hopes of increasing volume of refractive surgery and, therefore, of increasing fees. There are two problems with this, at least in France: (1) the public puts premium value on its social insurance and (2) the lowest price is valued in today’s consumer society. In France, refractive surgery rates are relatively low compared with those seen in other countries with similar standards of living. The medical public accepts third-party payment as a right and, in general, expects no direct out-of-pocket payment for medical services.
For policymakers seeking to distribute scarce social resources, the advantage of cost-utility analysis is that the quality-adjusted life-year provides a common unit for comparing the effectiveness of health interventions across different medical conditions and specialties. This analysis does not help with refractive surgery, however, because most services exceed the limits of usual cost-utility. Out-of-pocket payment for refractive surgical care occurs in many countries because these interventions are not usually covered under publicly financed health care packages.
REFLECTED IN THE COST
The lowest price I have seen in 2016 in the European Union for LASIK is, all included, €780. The highest price is unknown, but €7,000 is nearly at the summit. Surface ablation procedures such as PRK and epi-LASIK usually carry prices similar to those of conventional LASIK or perhaps €200 less per eye. For a comparison, Figure 1 details the average price per eye that US surgeons charged for LASIK from 2010 to 2014. These figures, provided by a leading industry analyst, are available on www.allaboutvision.com.
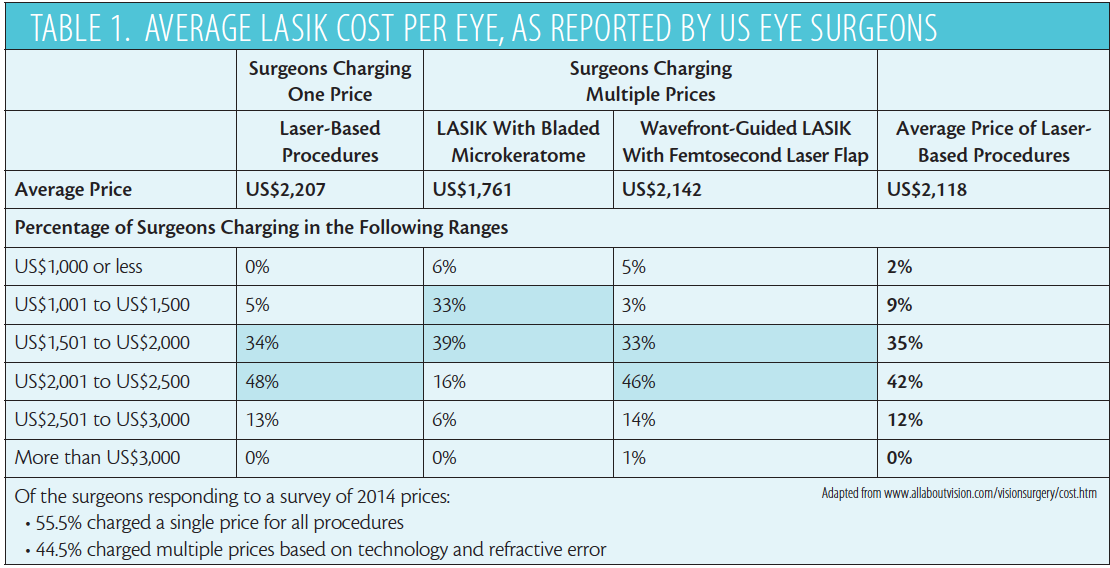
We may expect to see higher costs for newer LASIK options, such as femtosecond LASIK, than for traditional LASIK, but the truth is that the cost of LASIK can vary significantly from one provider to another. Prices depend on what technology the surgeon uses (Table 1) and sometimes other factors such as how much vision correction the patient needs, how difficult a particular procedure is, the degree of the established reputation of the operating surgeon, and the varying levels of preoperative testing performed.
Because proper screening can avoid postoperative problems, it is important to determine whether appropriate preoperative testing is included in a quoted price for LASIK. Technologies for eye tracking; tear film analysis; and measurements of corneal thickness, corneal topography, and pupil size may be available at various price points and can be reflected in the procedure fee. Pricing may also reflect which laser is used. Wide variation exists in the cost of equipment used for testing and surgery. Costs are computed in different ways at different centers.
Some surgeons turn the postoperative period into additional charges to the patient. The charge for a 1-year follow-up visit, for instance, may be between €500 and €2,000. Another variable is whether retreatments are included in the basic price. Many surgeons do not charge a separate fee for new technologies used in LASIK but instead quote their price as a single fee. However, prices may be higher when a femtosecond laser is used or when new software providing customized or aberrometry-based treatments is used.
As with any technical act, the proposed fee must take into account expenditures, investments, and training time and include a fair profit for the performer. The situation is not unique to LASIK, and the feedback modes depend on many parameters. One point is certain: In theory, nothing justifies an experienced surgeon earning more for a similar act than a beginner or a less-well-known practitioner. But this dogma may have little resemblance to reality. In real life, that which is renowned is generally more expensive. The discount of LASIK fees by beginning or less-well-known surgeons may be based on the concept that they are providing an identical service, all other things being equal. Unfortunately, this is uncertain because there is no tool for verifying individual qualifications.
LOW-COST MODELS
LASIK CHAINS
• Simplify supply issues
• Locate outside of high-rent areas
• Provide reduced ancillary services
• Use a high-volume model based on the organization of a network of franchisees
Several principles, listed in the graphic above, are used by those wishing to provide a low-cost service, such as a LASIK chain. Indeed, the low-cost model is initially based on extreme simplification of existing products and services. Such no-frills practices supply and perform only what is necessary. They pay employees well and expect more productivity, cut out the middleman and use the Internet to sell directly to the customer, and charge for a lot of things that people take for granted.
An alternative way to achieve a low-cost model is to be oriented toward particular goals by a mutually agreed system that gives its members a sense of purpose. Most social insurance does not cover refractive surgery because it is considered cosmetic. However, employers or other organizations may make arrangements with a given LASIK or refractive surgery center for a special price for their employees or members.
Costs of equipment, personnel, and fixtures are much the same everywhere. But competition is virtuous only when technological innovation exists. Savings are achieved in low-cost centers oriented toward the most profitable and least sophisticated actions. Reduction in prices is a result of the simplification of the product strategy. It presupposes acute analysis of several factors, of which the first is the expectations of patients and the second is their ability to pay.
With surgery, there is often a third factor: patient fear of surgery on the eyes. This is a key point because it involves consumers who do not think in absolute terms but in terms of a price-to-quality ratio (value for money) when they are choosing between two options. These consumers will compare price differentials with quality differentials.
Some patients participate in medical tourism and fly to places such as Eastern Europe, Asia, or Africa for surgery. It is possible to find financially attractive packages that include travel, hotel, surgery, and early postoperative care. Many centers in these locations and elsewhere have proven their expertise in providing world-class products and services at low cost. Because surgical complications are rare with LASIK, the risks are acceptable for many patients. Low-cost promotions allow these centers to run their operating theaters at nearly full capacity.
However, cheap means cheap. If a patient needs more care, or care for an increased duration, low cost may mean no service and no help free of charge.
Most LASIK surgery centers and private medical practices work with one or more insurance companies to offer financing plans to their patients. This is rarely used in France, but it is far more frequent in other countries, especially for high-cost procedures.
PROVIDING QUALITY
Research is the backbone of patient choice. However, differences among practices may not be obvious to most consumers, who believe that a high price guarantees impeccable delivery. High rates must be associated with services that provide the distinctive and effective benefits expected by consumers. The so-called evidence that can be found on the Internet and through word-of-mouth is not a reliable indicator. The surgeon must learn to take the opportunity to be great and to believe in the LASIK service that he or she delivers. Price is a reflection of the attitudes of the surgeon and the center.
In deciding how to model their practices, physicians must focus on growth and value, their years in practice, their costs, and their expected return on investment. Most important is the impact of price. A surgeon in private practice works for him or herself and for the facility, and these qualities determine his or her brand. To increase patient flow, it is important for the qualities and attributes of the brand’s service to have a high level of value in patients’ minds. To offer low-cost surgery can damage one’s personal brand and product image: As noted previously, cheap means cheap.
The premium practice can offer only quality services, but these can be fragile and difficult to maintain. Because it is impossible to offer low-cost premiums for sophisticated technologies, research is needed to determine appropriate level of pricing. Low cost is characterized by a stripping-down of services toward basic functionality. For a premium practice, it is important, paradoxically, to emphasize the existence of operative risk, the practice’s obligation to perform precise preoperative testing, and, finally, the importance of postoperative care. One can work perfectly with fairness and serenity if prices are not devalued.
Patients must know that the postoperative course includes help when needed and, of course, ample time for questions and follow-up. Evolution is inevitable, and premium practices should expect to constantly offer innovative methodologies and technological breakthroughs. This marketing principle must be based on strong public demand.
An eternal question in the minds of refractive surgeons is this: What is preventing higher acceptance of refractive surgery? Correction of vision by external prostheses—glasses and contact lenses—continues to increase, but we do not observe this same increase in refractive surgery in any advanced country. In 2014, 20.6% of the French population bought at least one piece of optical equipment in the form of new glasses or contact lenses. The increased use of equipment may indicate two phenomena: (1) an increase in the need for correction among a given population and/or (2) increased consumption of optical products per person. Nothing in the consumption of optical goods, therefore, indicates a reduction in need for optical correction or a reduction in spending. Complications of refractive surgery are rare, and there should be strong theoretical demand. Who will benefit? The practice offering the lowest rate? Perhaps, but then surgeons will no longer be in control. Most surgeons would prefer to offer a high-quality solution for their patients’ visual needs.
CONCLUSION
In order to compete against low-cost providers, practices must invest their intangible capital—the good name and reputation of the surgeon—and maximize flexibility for patients. They must provide facilities for payment, ease of scheduling, and other amenities. The philosophy of a dynamic center run by a traditional structure will be, first, to lower costs, and, second, not to reduce profit margins for the center. Consumers must be informed that choosing a surgeon based only on the fee charged may be unwise. It is better to suggest that patients seek the best and most appropriate surgeon.
Dan Alexandre Lebuisson, MD
• Medical Director, Visya group-Clinique de la Vision Paris, American Hospital of Paris
• dalebuisson@gmail.com
• Financial interest: None acknowledged
