



As I write this article, my companions and I are flying over the Nubian Desert and approaching South Sudan. Looking out the window over the vast Sud below, I remember a mission trip down there in 2011 that was beset by civil war, flooded roads, and failed logistics of moving supplies. On this flight today, we are bound for Kenya with an exemplary team of doctors, nurses, students, and laypeople to provide eye care to some of the world’s poorest people.
I am a man of faith who felt a calling early in life to serve the poor, and mission work has always been a career priority. This trip marks my 11th in East Africa. I have had the pleasure of serving with hundreds of team members, working together to see on average 1,000 patients in 3 days and perform sight-restoring manual small-incision cataract surgery.
We do not use phacoemulsification because most patients have grade 6 cataracts with no corneal specialists available to manage pseudophakic bullous keratopathy. We have, however, been able to adapt modern technology to improve outcomes. My favorite hack idea is to connect a CapsuleGuard I/A handpiece (Bausch + Lomb Storz) to a bag of lactated Ringer’s solution and a 10-mL syringe for aspiration instead of a Simcoe cannula for cortical cleanup (Figure 1). This technique reduced our rate of posterior capsular rupture to zero for irrigation and aspiration over 60 consecutive cases.1
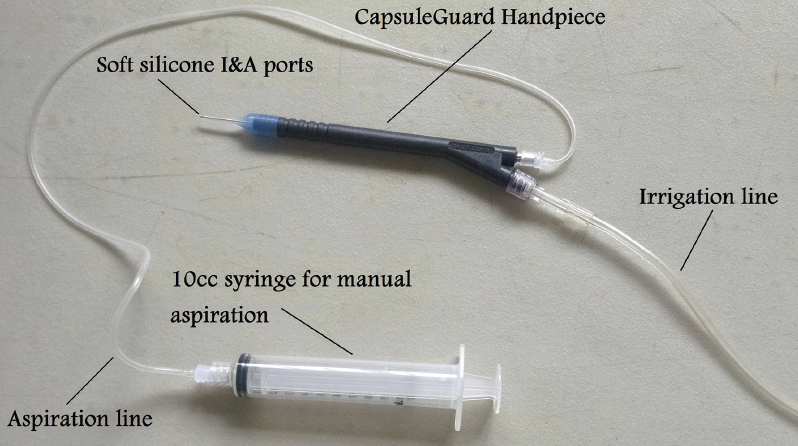
Figure 1. The CapsuleGuard I/A system reduced the complication rate during cortical removal to zero. The irrigation line was attached to an intravenous bag of lactated Ringer’s solution. Dr. Page used a 10-mL syringe for aspiration.
CHALLENGES
Working in East Africa can present major challenges. For starters, supplies and equipment are not easy to obtain. Instead, supplies are donated by generous companies and then taken, one bag at a time, by each team member. We carefully distribute the supplies among bags so that, if one goes missing in Nairobi, we don’t lose all the lens implants, OVDs, and other materials.
Our equipment is also donated. I have found that nothing sharpens my ophthalmology skills more than working with microscopes and slit lamps that are older than I am. The optics and parts are not up to the standard to which I have become accustomed, and sometimes we simply don’t have the equipment or supplies we need.
On one mission, for example, our wet-field cautery broke, and our last cautery pen had died. Our Kenyan colleagues showed us how to create a type of Bunsen burner on the back table by punching a hole in the metal cap of a medicine bottle with a screwdriver and threading packing gauze soaked in acetone into the bottle (Figure 2). Igniting the gauze provided a continuous burn for hours, allowing us to heat a muscle hook and use it to cauterize the conjunctiva. It took a while to get used to having an open flame in the OR. We don’t use any oxygen or sedation, so the open flame cautery was slightly safer than if we did. Hacks like this one get the job done, and they make us grateful for what we have in the United States.

Figure 2. When electrocautery was not available, surgeons in Kenya created makeshift burners to heat a muscle hook to cauterize blood vessels. Extreme caution was used, and plenty of cautery pens were brought the following year.
Our power supply has improved significantly over the past decade. I find myself having to finish far fewer cases by flashlight because our generators can power the microscopes during the power outages that frequently occur in rural Kenya. One particularly memorable power outage occurred when a lightning strike rocked the entire clinic with a sonic boom as I was entering the anterior chamber with a sharp keratome.
REWARDS
The challenges of mission work are great, but the rewards are greater. The most memorable occurred 5 years ago when a young mother traveled by bus and foot from Tanzania to obtain care for her 2-year-old son, who had fallen head-first into a cooking pot full of boiling liquid in their hut 6 months earlier (Figure 3A). A lack of access to care had delayed the initial assessment. The severe third-degree burns had taken off more than 50% of the child’s scalp and brow. With no medical treatment whatsoever, he developed an orbital cellulitis with massive proptosis (Figure 3B). After hearing that a team of US doctors was in the neighboring country, the mother made the long journey. Unfortunately, the repair was beyond what our team could perform, so we arranged to have the mother and child taken to Nairobi for care and moved on to the next patient.

Figure 3. The child in this figure presented 6 months after falling into a boiling pot of water used for cooking. The author and his colleagues were the first doctors the child saw. Severe proptosis due to orbital cellulitis prompted the family to travel hundreds of kilometers to receive care (A). The eye was not visible, and the eyelid had been burned away (B). Doctors at Tenwek Hospital performed grafts from the child’s thigh (C). The child had a remarkable recovery, and the eye was saved.
After returning to the United States, I contacted our clinic to find out what had happened to the boy. The staff tracked down his mother and learned that the hospital in Nairobi did not admit the boy but instead sent him home with antibiotics. At first, I thought this information was incorrect, so I asked them to check again. The account was confirmed.
That day, through contacts in global outreach, I found a hospital in Israel that seemed willing to take him. At first, it appeared that the ear, nose, and throat service would admit him, but they wanted neurosurgery to take the boy. Then neurosurgery said they wanted pediatric ophthalmology to take him. After weeks elapsed without his placement, I looked to my own hospital in Michigan.
I spoke to burn care doctors, neurosurgeons, plastic surgeons, and anesthesiologists. We assembled a team to take care of the boy, and everyone involved agreed not to charge fees. It was estimated that the boy would require 2 months of care in the intensive care unit and recovery, and the hospital wanted $400,000 upfront before admitting him. I knew this was not a realistic goal and gave up on my local hospital.
I reached out to the doctors at Tenwek Hospital in Bomet, Kenya. They said they could try to save the boy and that it might be achieved at a cost of $5,000. I shared the situation on social media and raised sufficient funds in 1 day. News reached the mother, and transportation was sent. The boy underwent a series of successful skin grafts from his thigh that resolved his pain, infection, and proptosis (Figure 3C).
A year later, I returned to Kenya and was finishing a case when the staff asked me to come outside. There was Dennis, held in his mother’s arms. He was healthy and looked nearly like the accident had never happened. The pair had traveled from Tanzania to thank me and give me a live chicken, an original gift indeed (Figure at outset; watch the video of the reunion below).
CONCLUSION
As I finish writing this article, our team is in the gathering space of our mission house, where they are sharing stories. Tomorrow, we will see hundreds of patients with blindness and eye disease, and we will work ourselves to the bone. When I get home next Monday and sit down at my femtosecond laser platform and high-performance phaco machine, I will remember this mission and be grateful for how good I have it in the United States as a citizen and a surgeon.
Two Ways to Get Involved
To donate to Kenya Relief, visit www.kenyarelief.org, click on Make a Donation, and select Brase Clinic/Medical from the dropdown menu. To inquire about serving on a team, contact Dr. Page at tpagemd@yahoo.com.
1. Page T. Cortex removal method to reduce posterior capsule rupture during manual nuclear expression small-incision cataract surgery. Paper presented at: ASCRS Annual Meeting; May 6-10, 2016; New Orleans.
