


Dr. Safran presents the case of a 14-year-old patient with bilateral ectopia lentis who was referred for cataract surgery. Dr. Safran’s decision to enlarge the capsulotomy after implanting the IOL in the capsular bag created a nightmare he had to resolve.
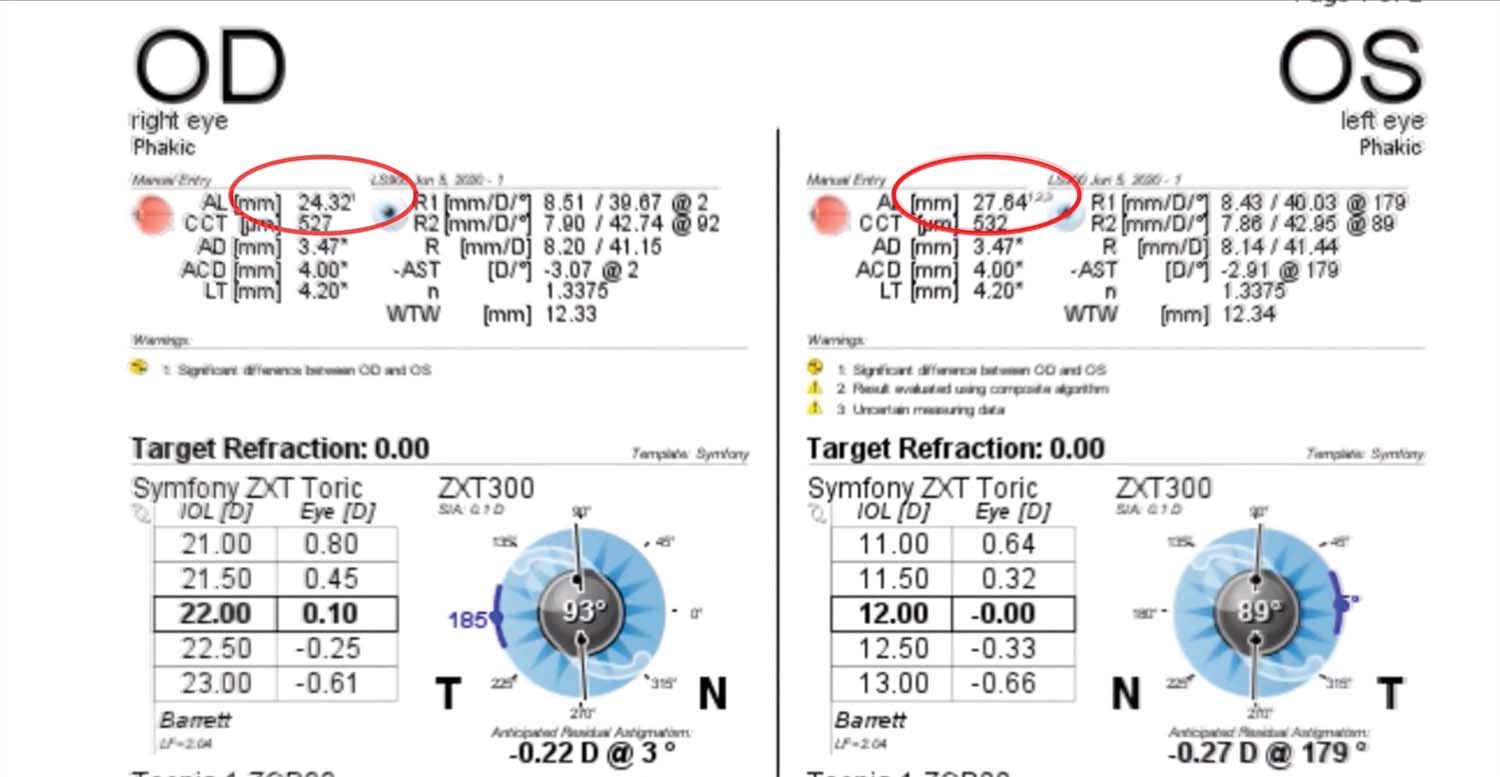
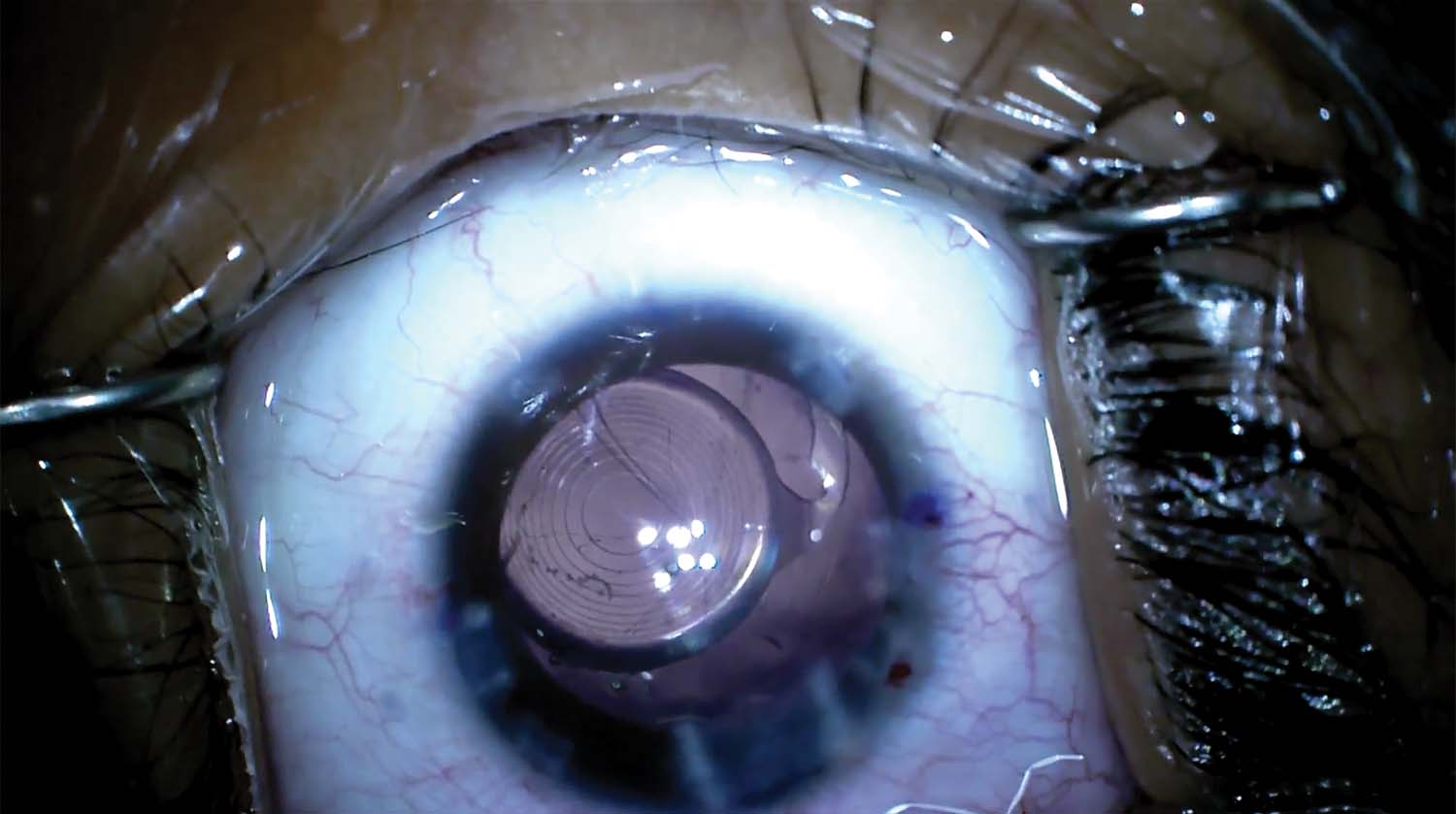
1. A 14-year-old boy with familial bilateral ectopia lentis is referred from 500 miles away for cataract surgery. Optical biometry finds asymmetry in the axial lengths of the patient’s two eyes (27.64 mm OS vs 24.32 mm OD). Implantation of a Tecnis Symfony Toric IOL (Johnson & Johnson Vision) on the steep axis is planned to correct the patient’s astigmatism and give him good depth of focus.
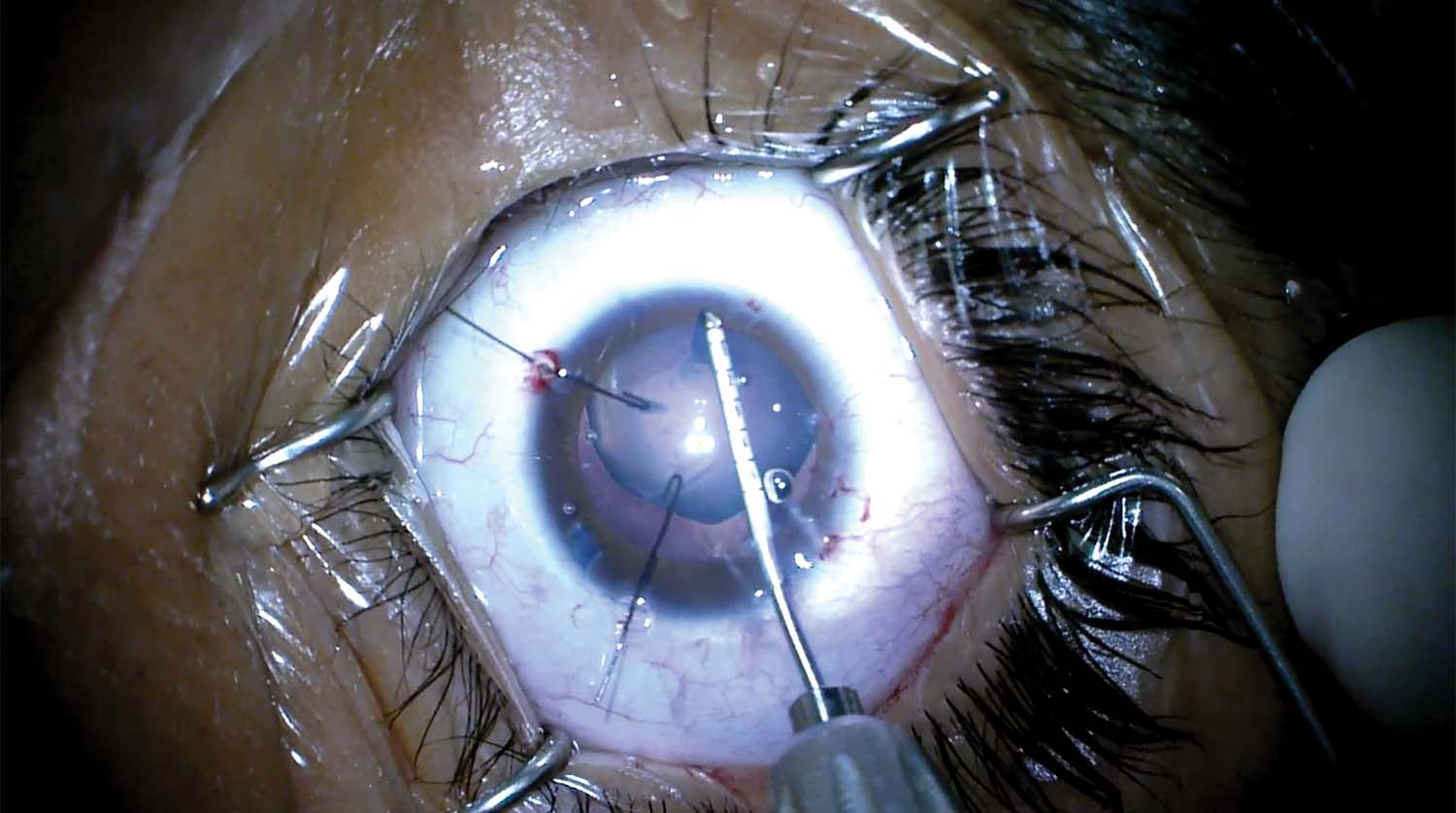
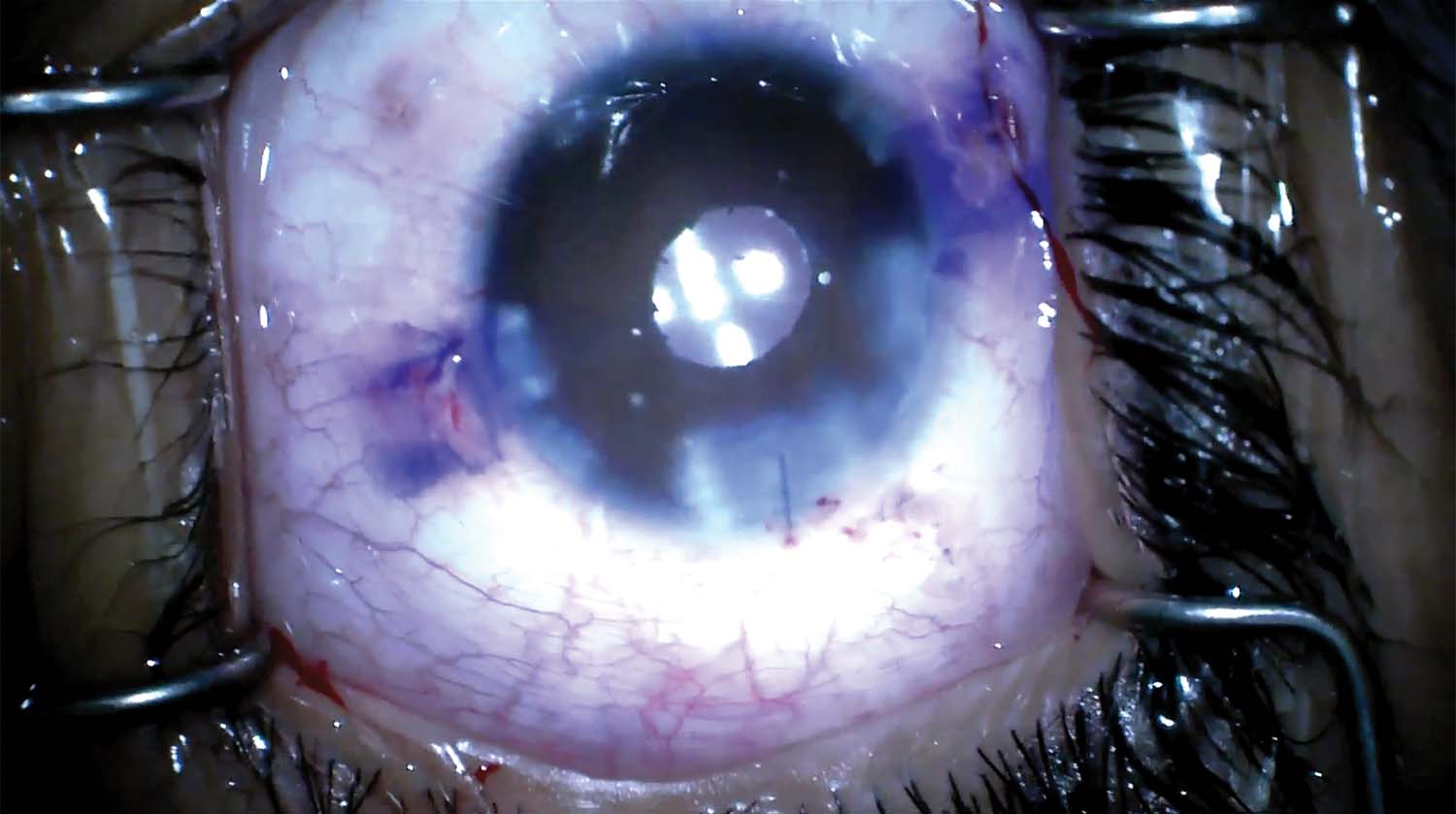
2. The capsulorhexis is initiated with a cystotome under trypan blue dye (VisionBlue, DORC). Iris retractors are used to provide countertraction and assist with the capsulorhexis.
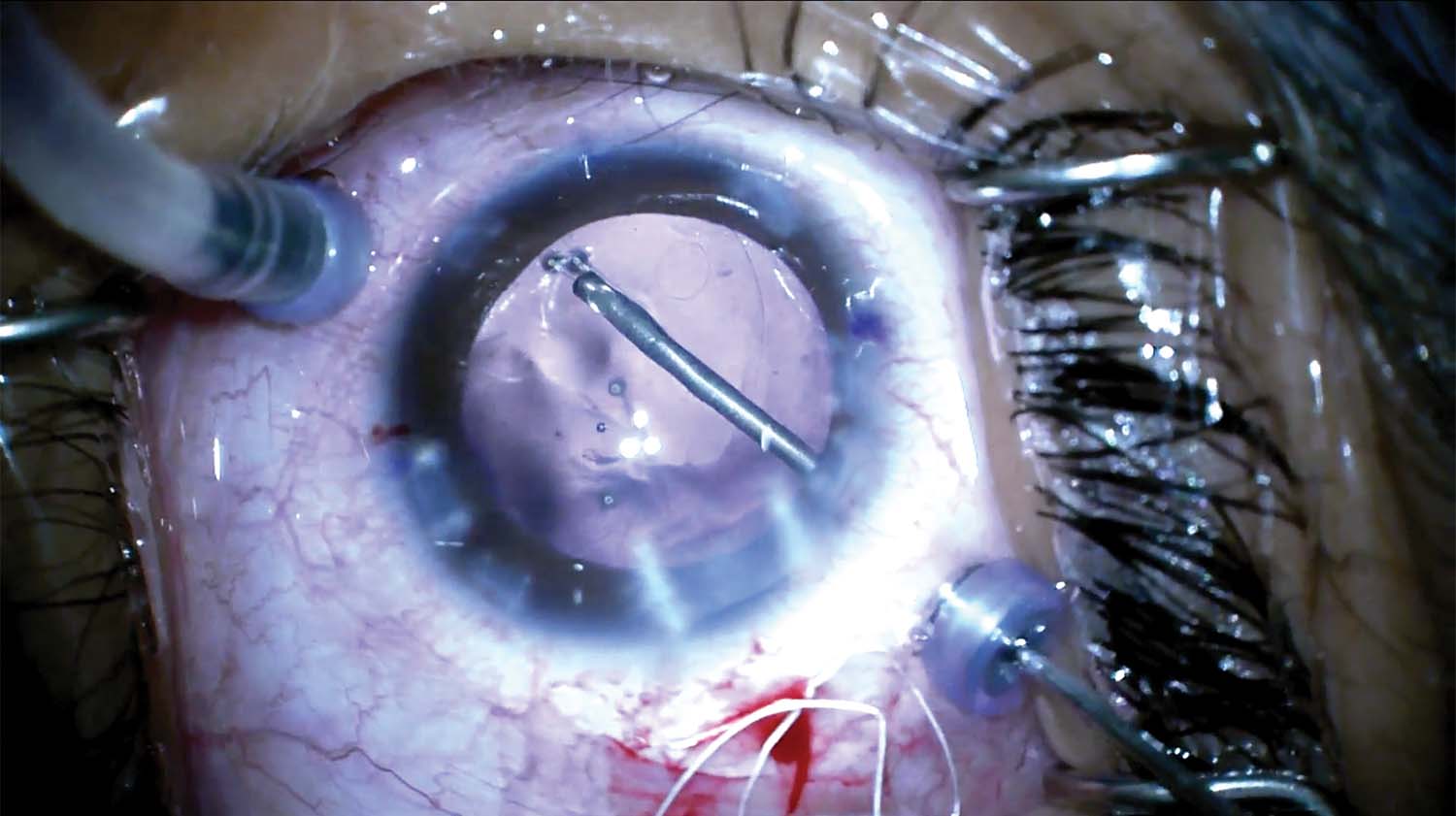
3. The iris retractors are replaced with capsular retractors to stabilize the capsular bag. The lens is aspirated, the capsular bag is inflated with an OVD, and a modified capsular tension ring (CTR; Malyugin Modified Capsular Tension Ring, Morcher) is placed in the capsular bag.
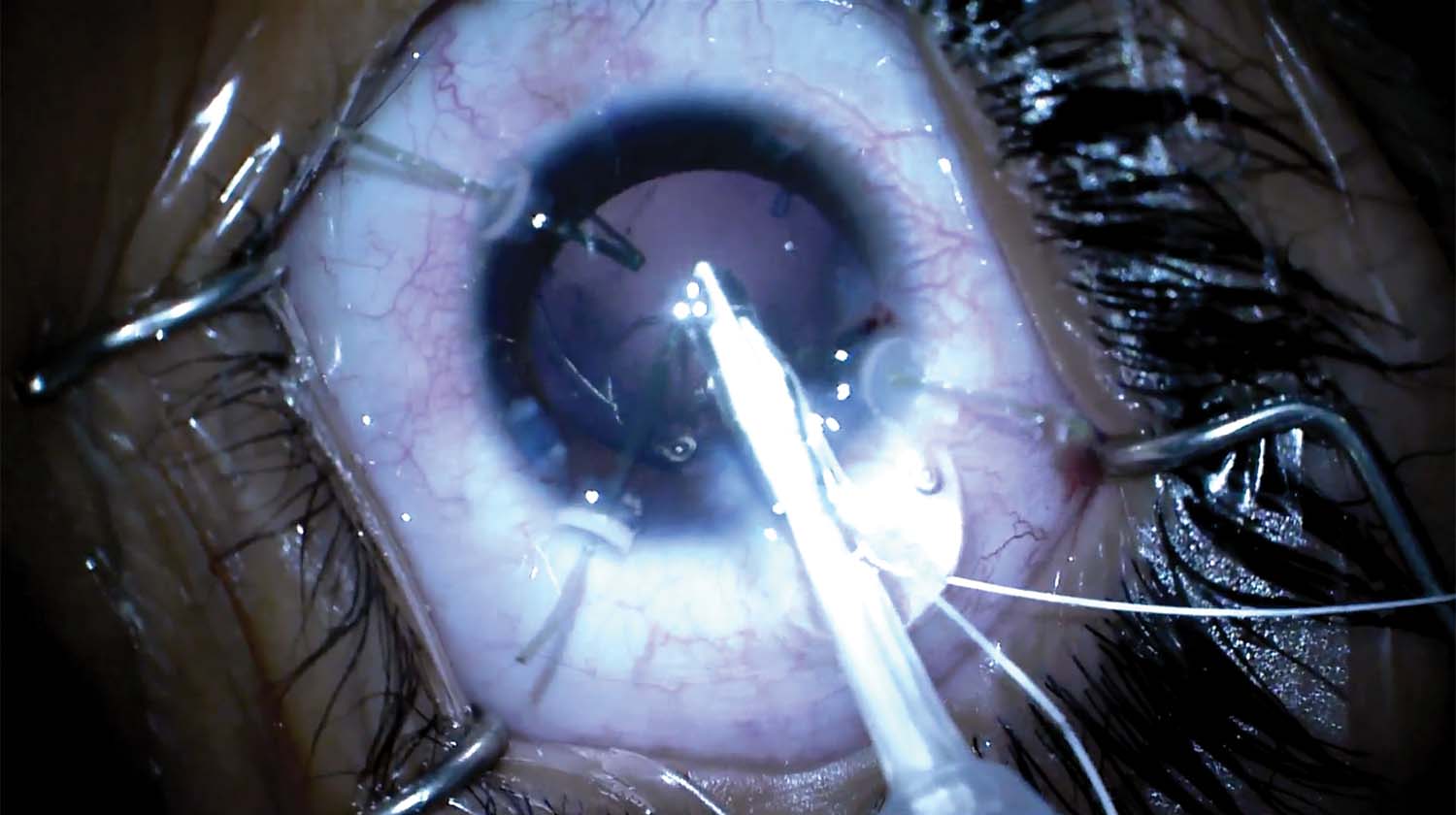
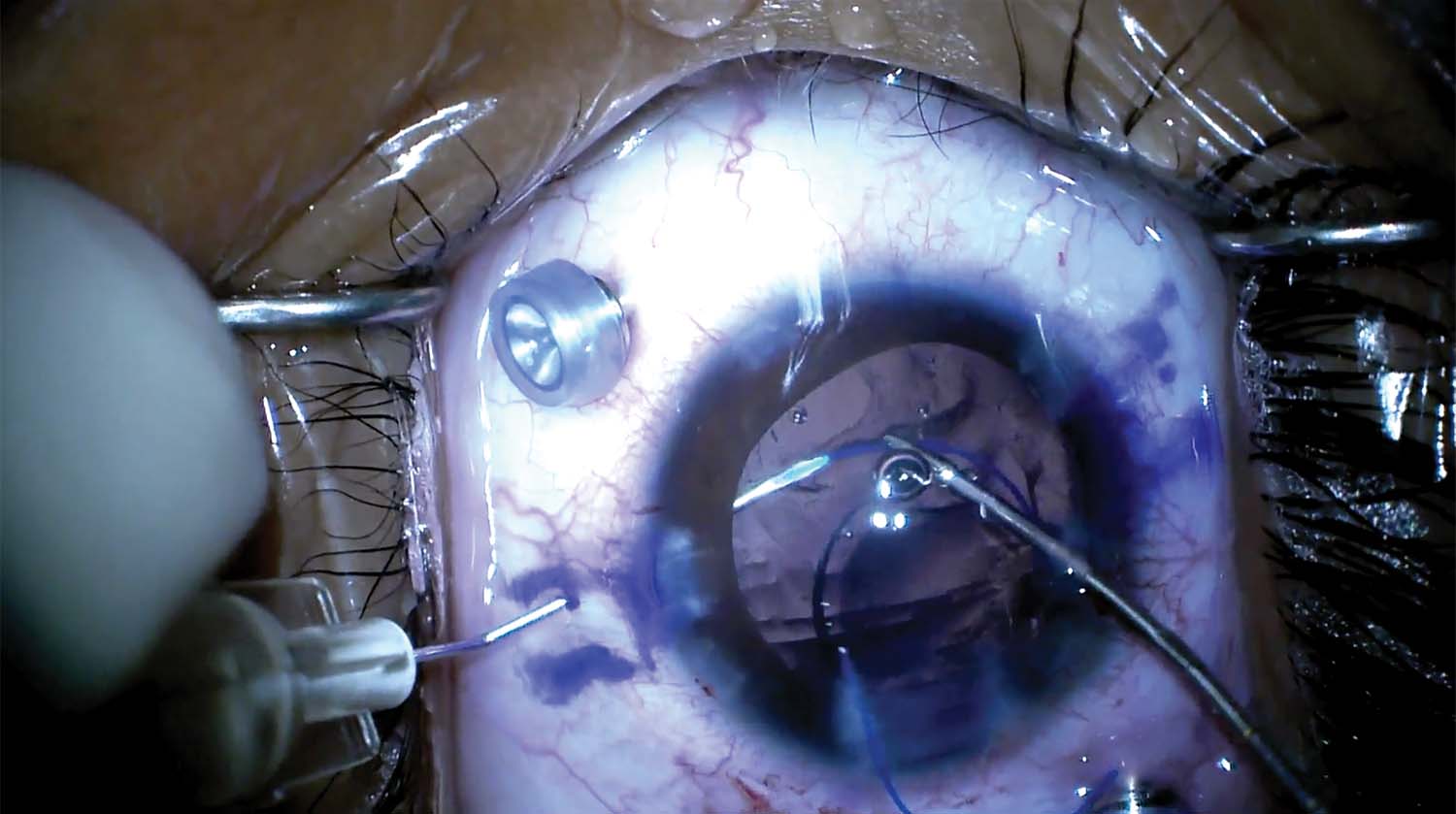
4. A PTFE suture is passed through the eyelet and sutured to the sclera.
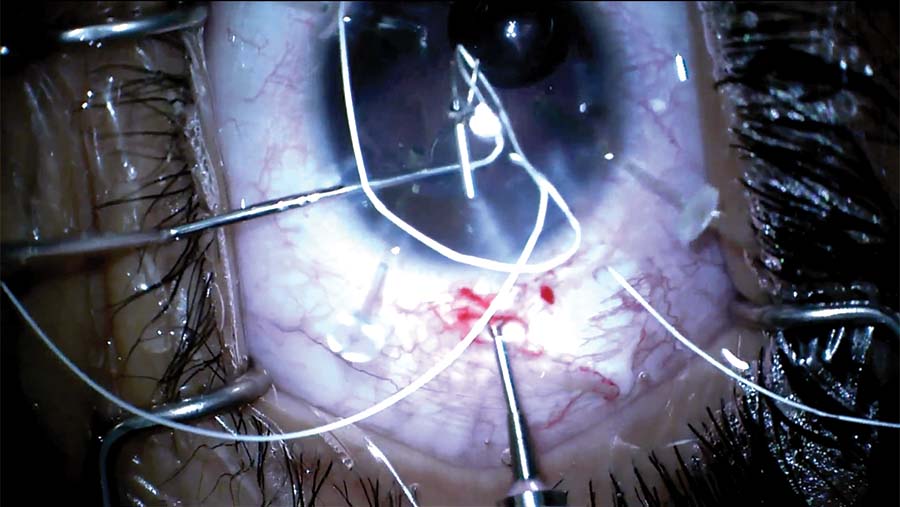
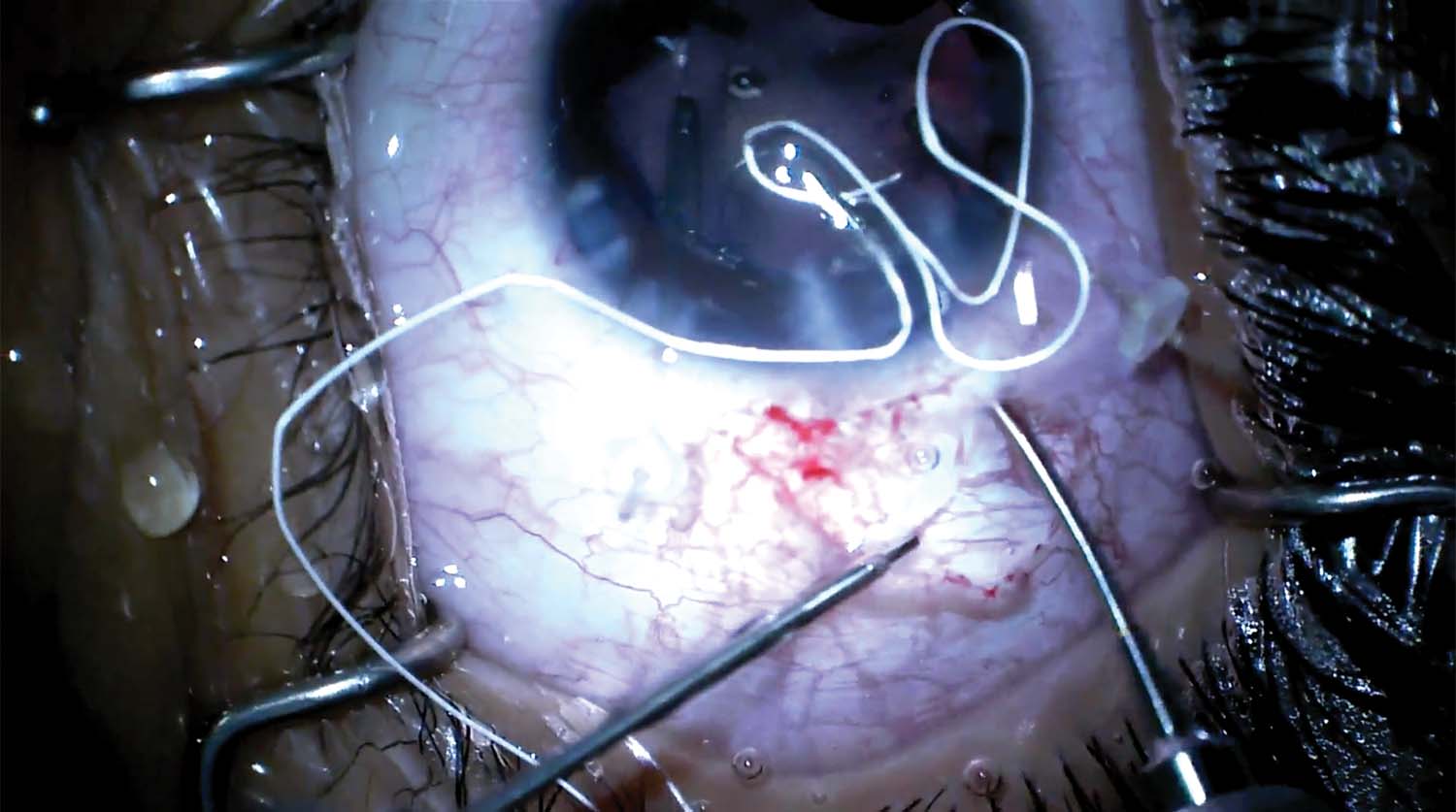
5. Two sclerotomies are made, and each end of the PTFE sutures is pulled through the respective sclerotomy.
6. A scleral groove is constructed to connect the sclerotomies. The scleral groove is undermined to create a shelf, and the suture is tucked underneath it.
7. The correct toric axis is marked, and the IOL is injected into the capsular bag and rotated into position.
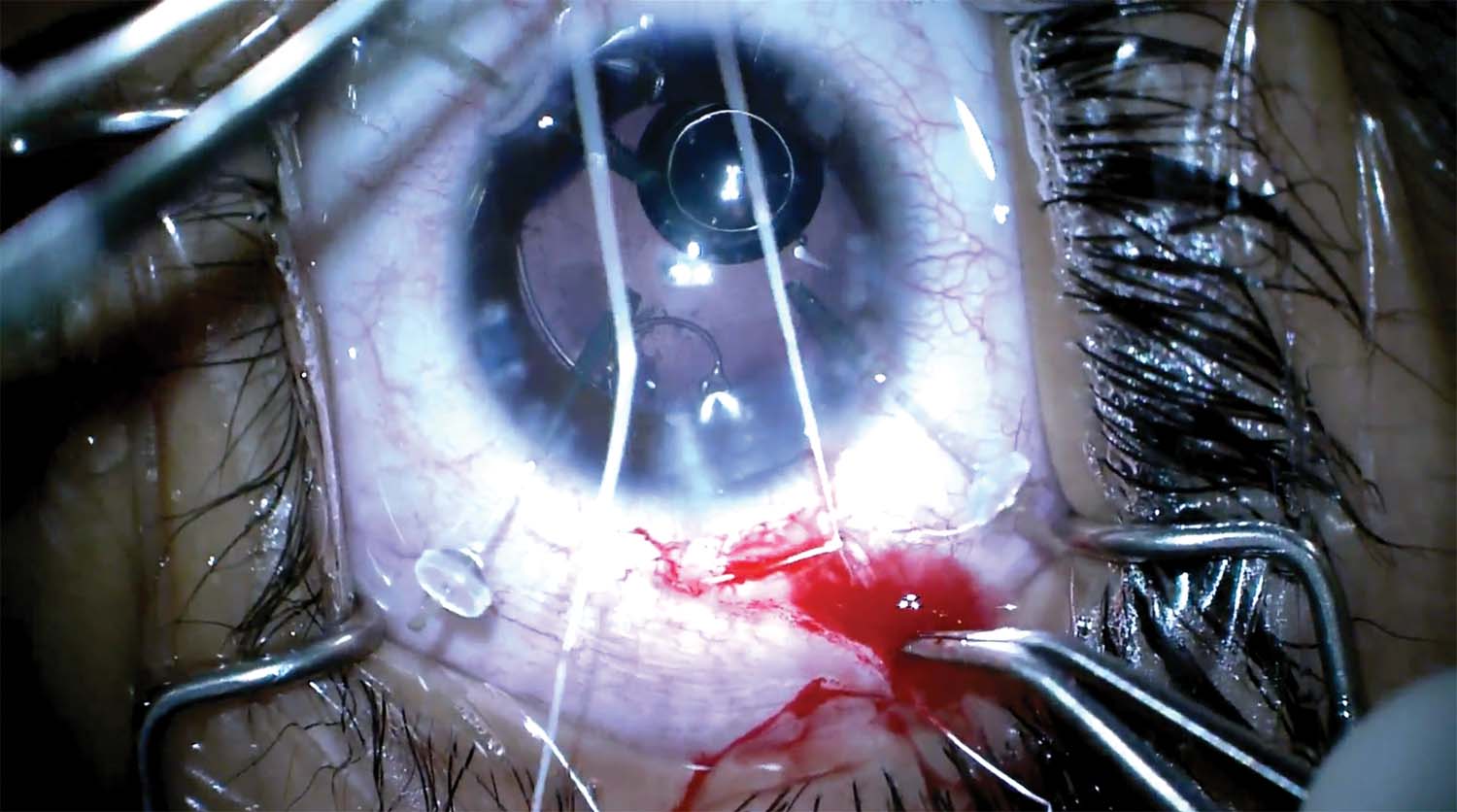
8. The capsulotomy is retorn to fix a slight overlap. After the first nip, the capsulorhexis begins to tear out. Another nip is made on the opposite side and then is connected to the first to complete the tear.
9. The capsular tear extends around the CTR and into the posterior capsule. An OVD is injected into the capsular bag. The capsule splits, the tear extends through the bag, and the IOL sinks into the vitreous.
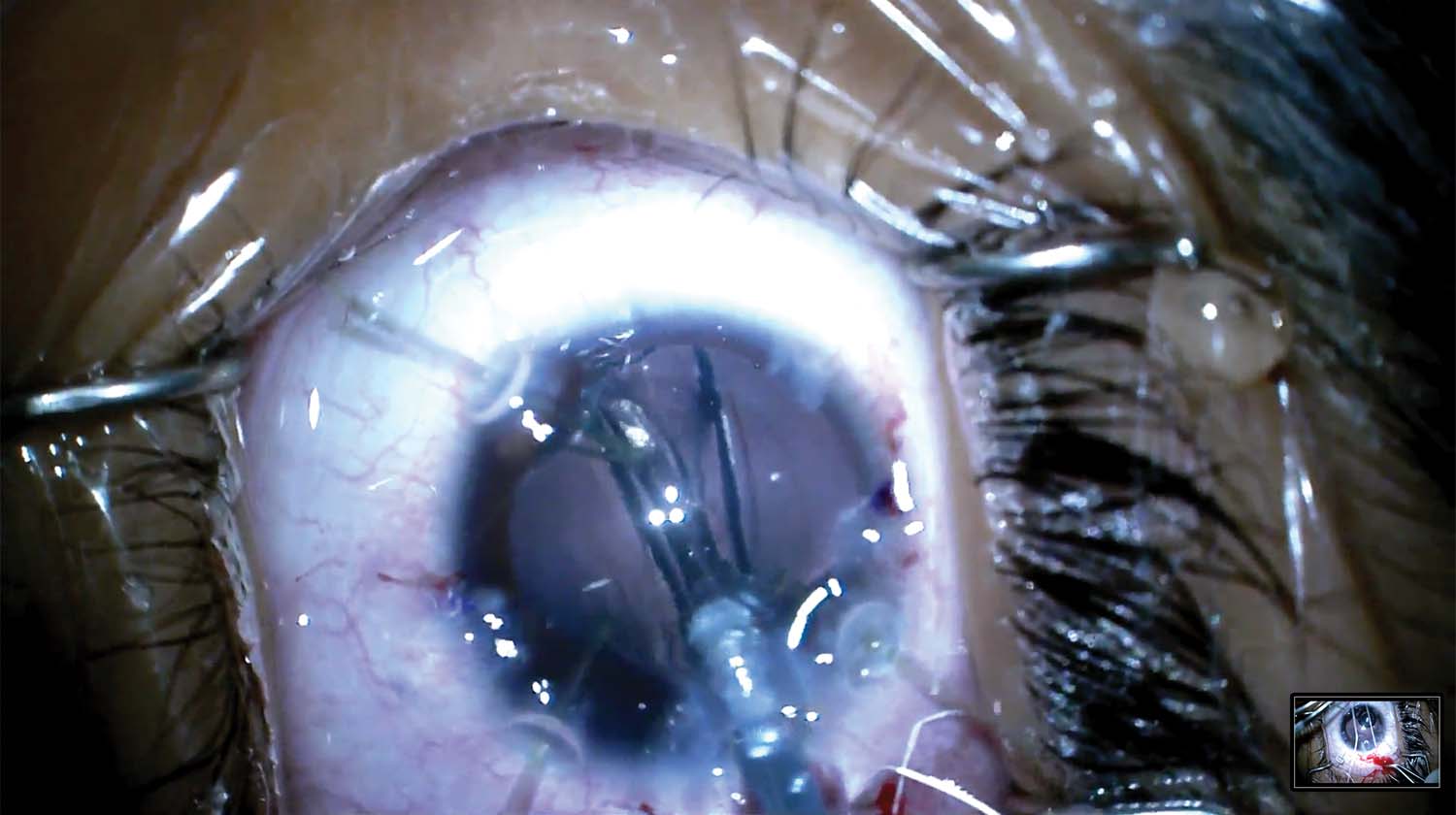
10. The IOL is removed. Two trocars are placed, and a pars plana vitrectomy is performed. The CTR is removed.
11. The eye is marked with an Agarwal Glued IOL Marker, and the Yamane technique is used to fixate the IOL. The first haptic of a CT Lucia IOL (Carl Zeiss Meditec) is captured with a TSK 30-gauge needle. The second haptic is captured 180º away, and both haptics are externalized.
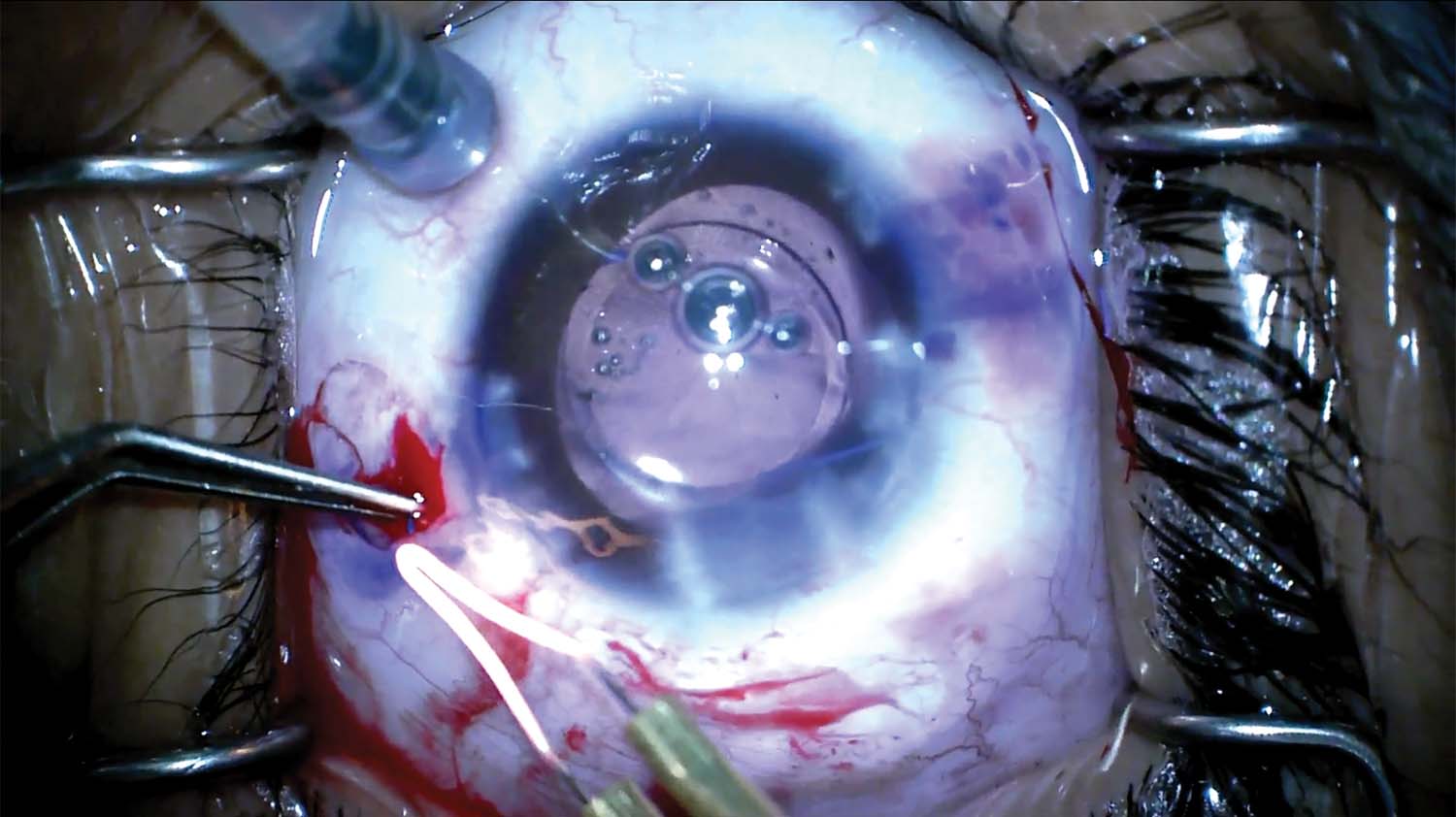
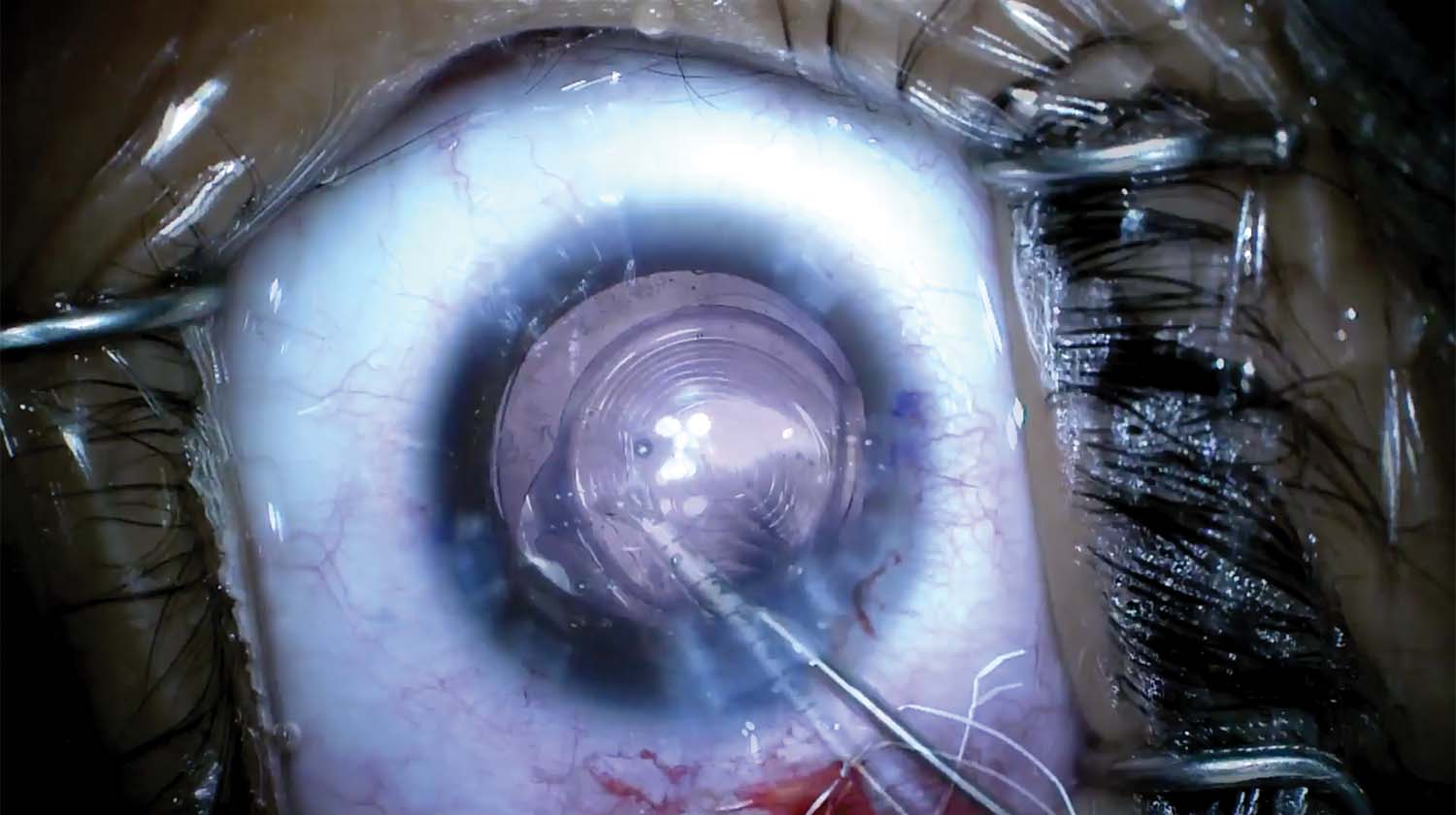
12. The tips of the haptics are melted into flanges and pushed into the scleral tunnels, and the lens is centered.
13. The OVD is aspirated, and acetylcholine chloride intraocular solution is injected to constrict the pupil. The trocars are removed, and the case is completed.
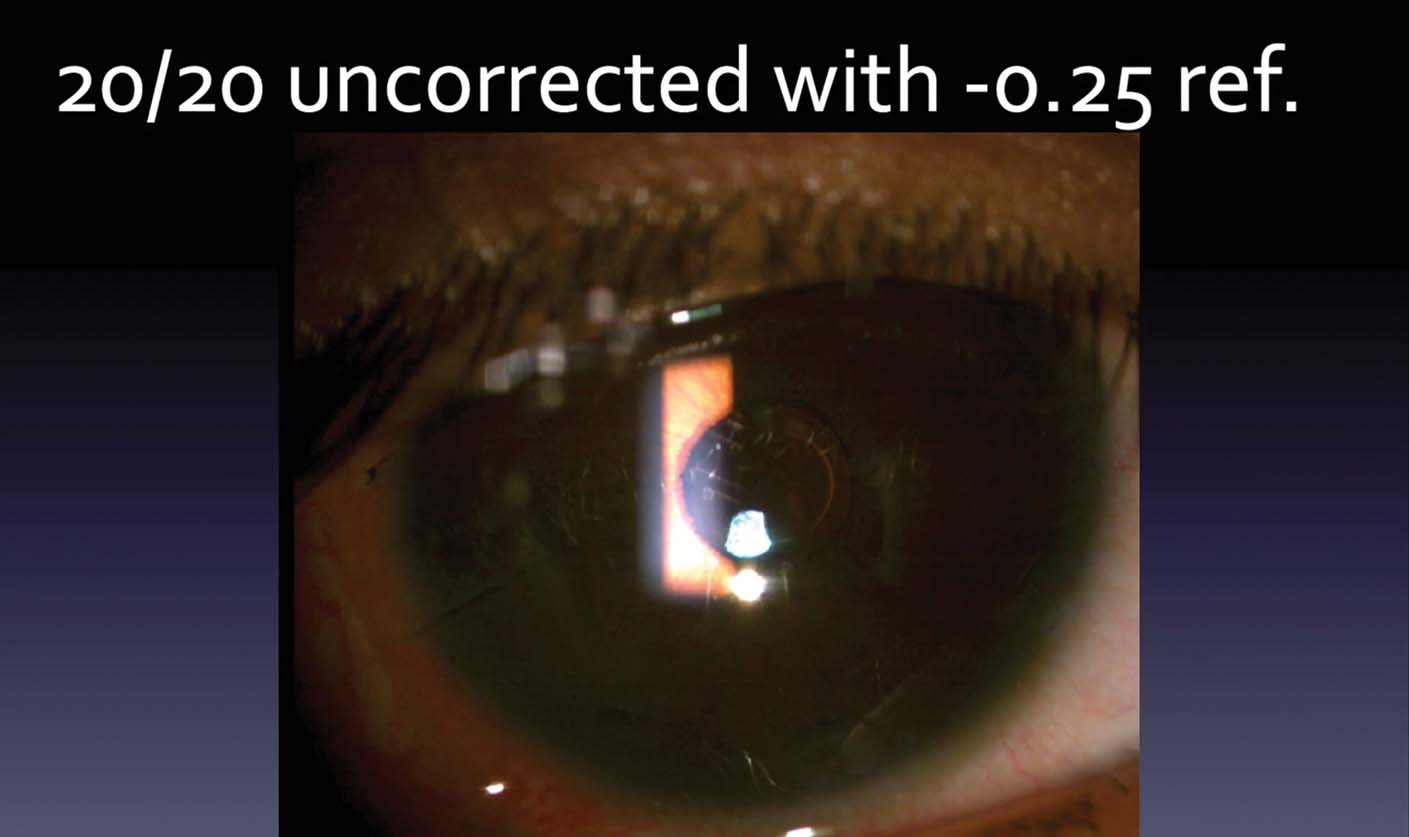
14. One week after surgery, the patient’s UCVA is 20/40 OS with a refraction of plano -2.25 x 180º correcting him to 20/25. One month later, cataract surgery is performed on the other eye with a scleral-fixated modified CTR. A Tecnis Symfony Toric is implanted in the capsular bag. On postoperative day 1, the patient’s UCVA is 20/20 with a -0.25 D refraction. The patient achieved spectacle independence and was happy with the vision in both eyes.

