


Dr. Devgan provides a tutorial on how to fix the haptic, flip the lens, and rescue the case.

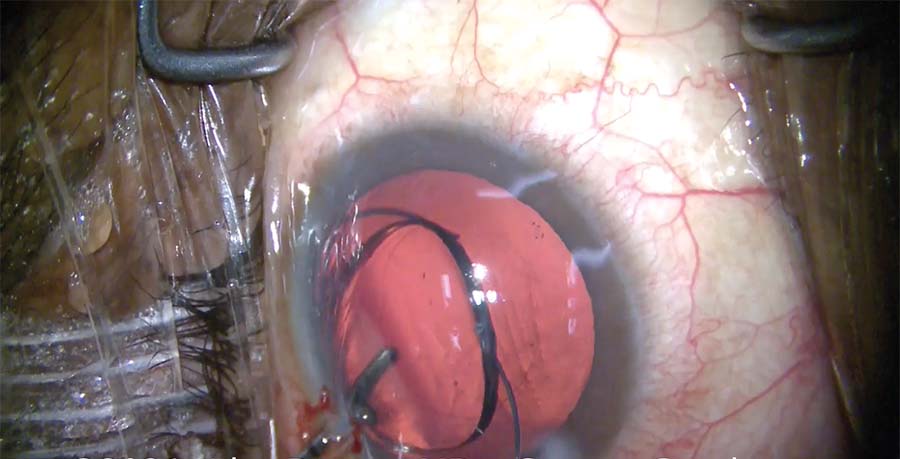
1. The cataract has been removed, and the empty capsular bag is filled with a cohesive OVD. The three-piece IOL is loaded into the cartridge, the injector tip is placed inside the eye, and the IOL is delivered into the capsular bag. The first haptic is released from the injector completely bent and in the wrong direction.
2. The IOL is flipped and pushed down into the capsular bag using a two-handed technique before the lens fully unfolds.
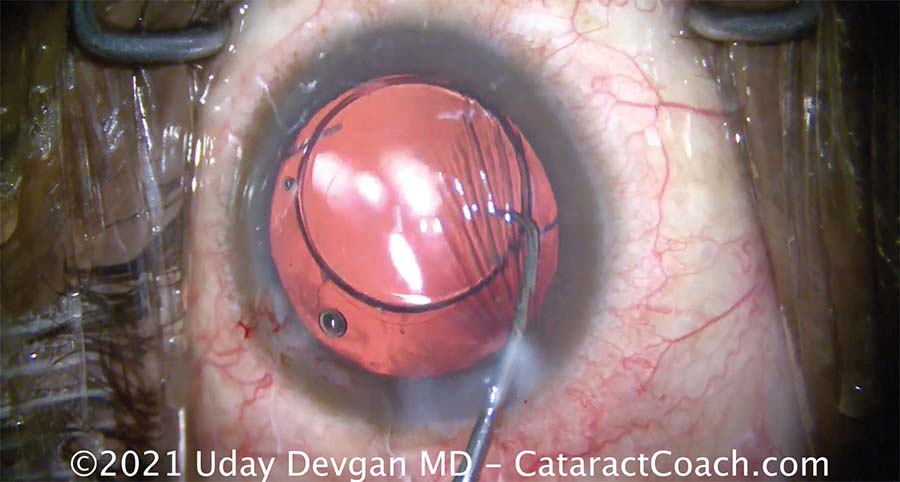
3. The IOL with the bent haptic is oriented correctly in the capsular bag.
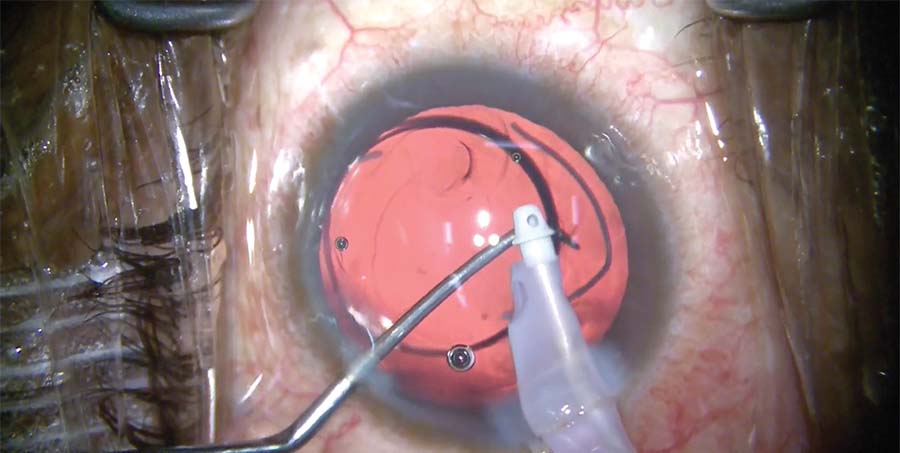
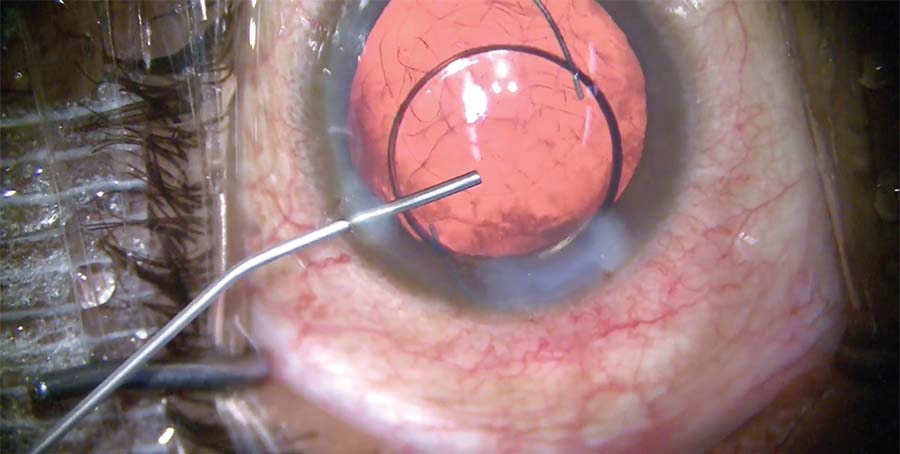
4. The bent haptic is brought toward the incision. An additional amount of OVD is injected into the eye. Infusion from the I/A tip is used to deepen the capsular bag.
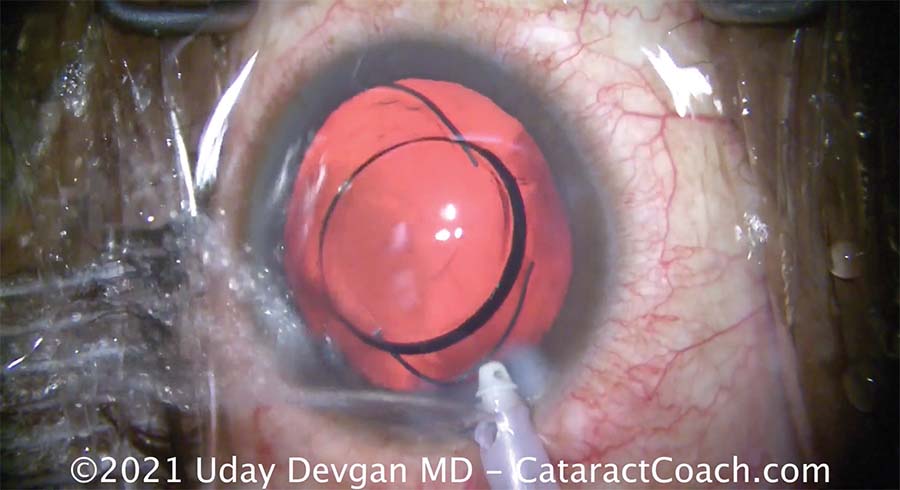
5. The IOL is lifted to prepare the haptic for retrieval from the capsular bag through the main incision.
6. The eye is filled first with irrigation fluid and then with a cohesive OVD to prevent it from collapsing and the IOL from moving in the bag. The wound is hydrated between maneuvers.

7. The haptic is grasped with forceps and pulled outside the eye.
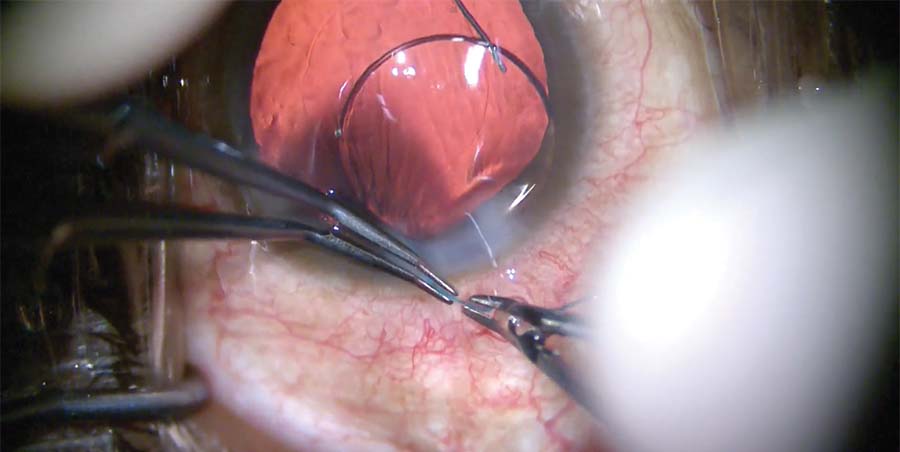
8. The kink in the haptic is straightened using two pairs of forceps and then bent back to its normal shape and orientation.
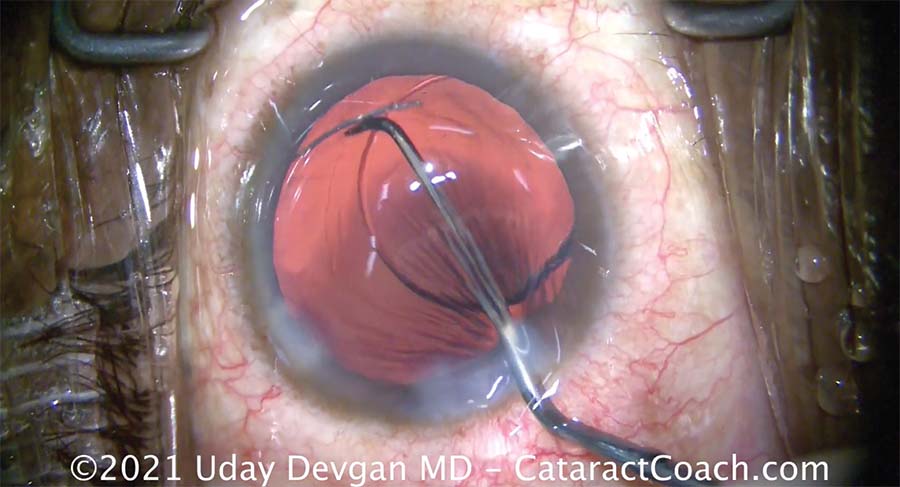
9. Additional OVD is instilled. The haptic is dialed back into the eye.
10. The haptic is in the sulcus. Additional OVD is injected, and the haptic is coaxed into the capsular bag.
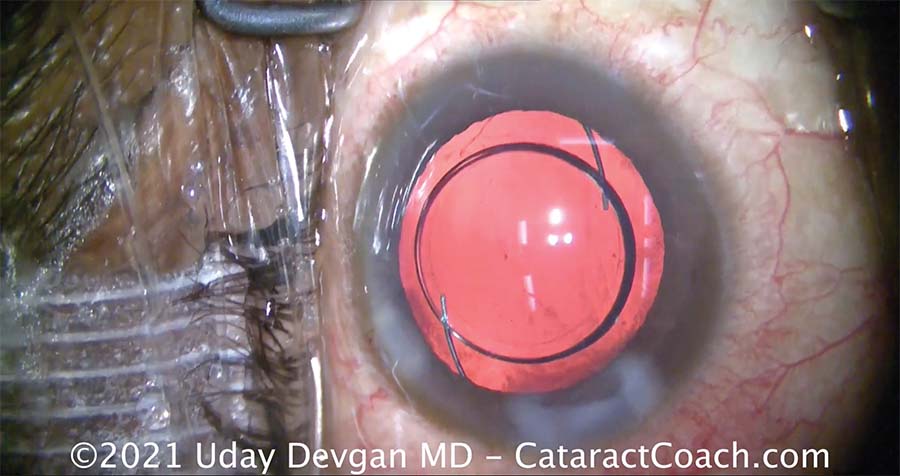
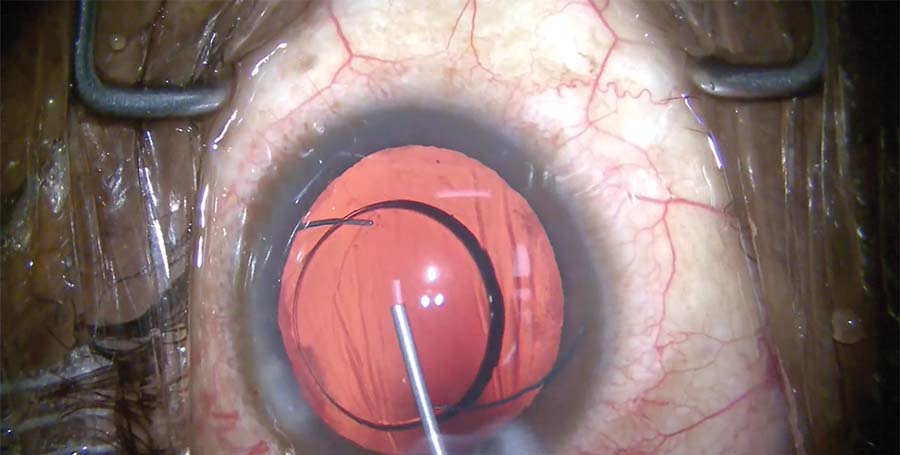
11. At the end of the case, both haptics and the optic are in the capsular bag, the IOL is well centered, and there is proper overlap of the capsulorhexis and optic. The incision is hydrated. The bag is reinflated with an OVD.

