


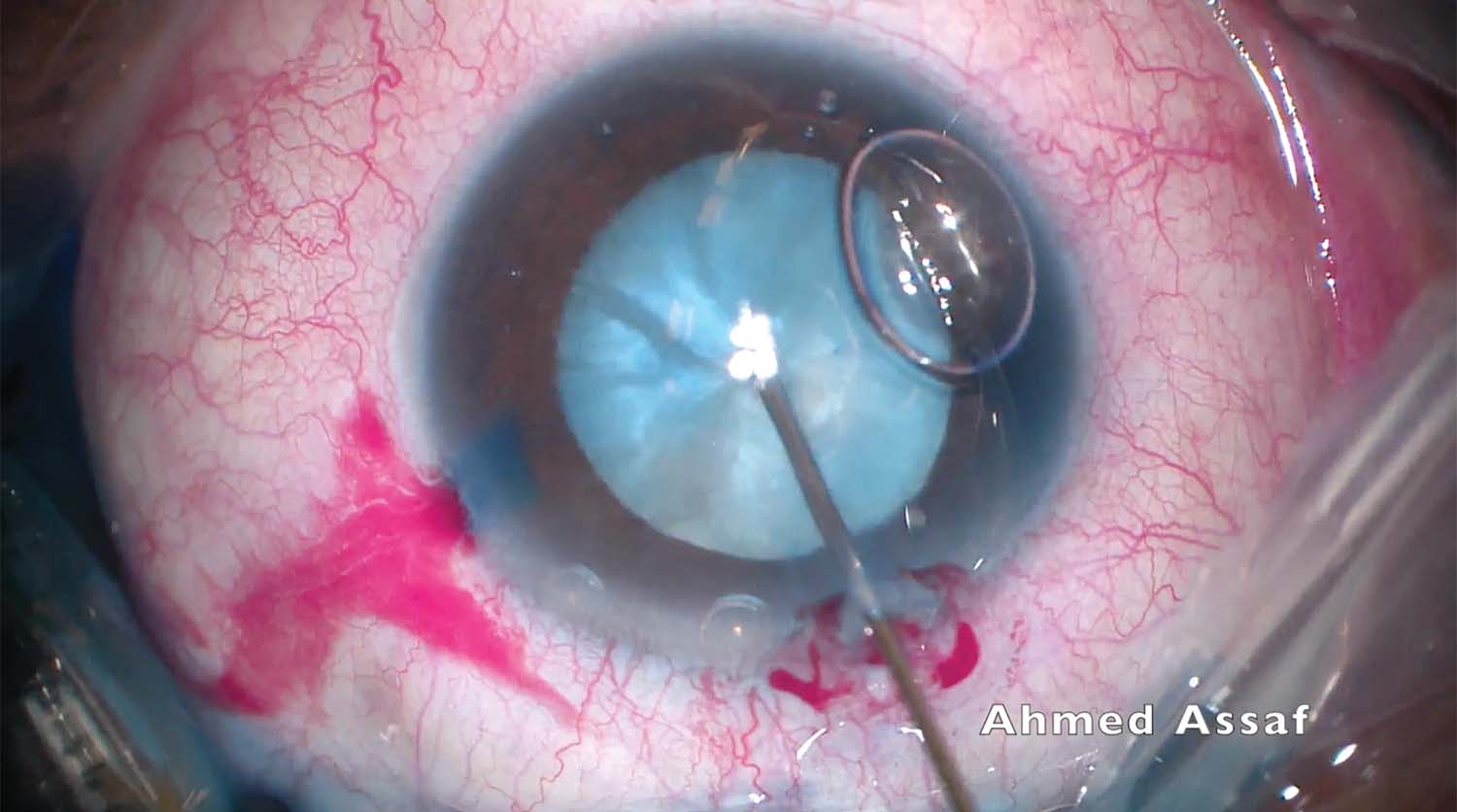
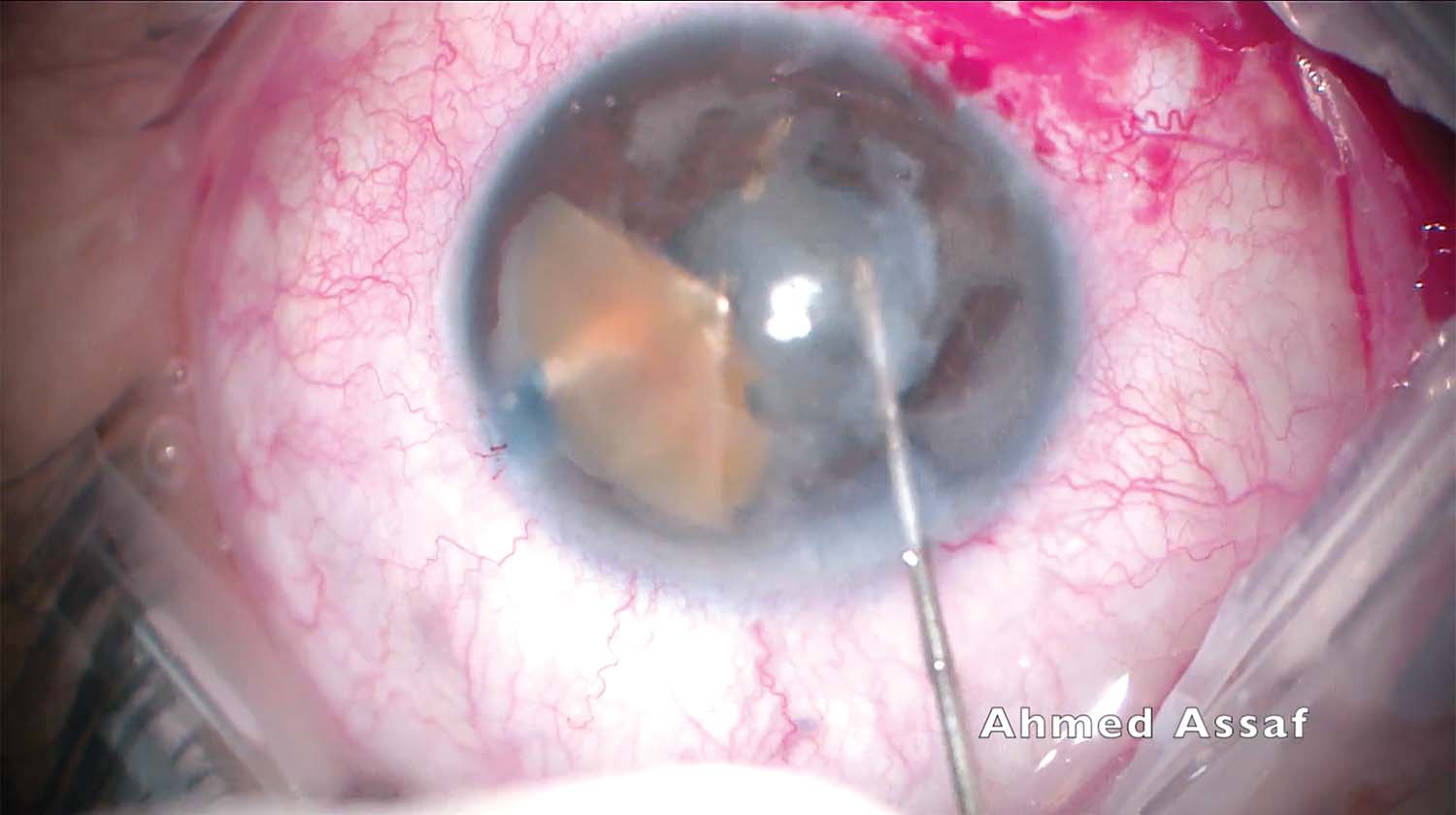
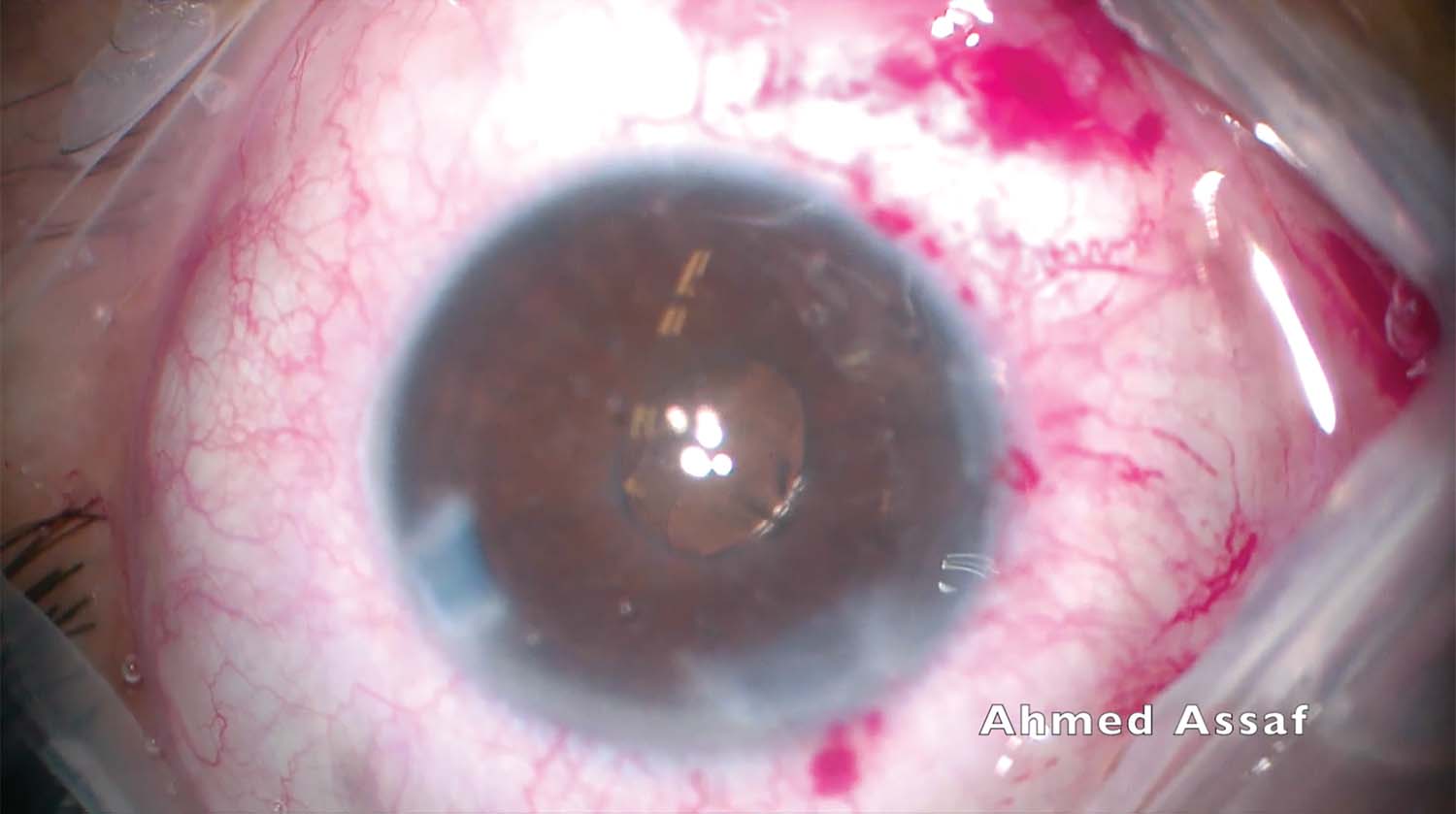
1. Conventional phacoemulsification is planned for a moderately dense white cataract. Trypan blue dye is instilled, and the anterior capsule is punctured with a 27-gauge needle to aspirate the emulsified cortex. The capsulorhexis is completed.
2. The nucleus is divided with a quick chop phaco technique. The posterior capsule is gripped and torn by the phaco tip. A significant piece of the nucleus falls into the anterior vitreous, likely through an area of zonular dehiscence inferiorly rather than through the break in the posterior capsule. A dispersive OVD is injected to prevent collapse of the anterior chamber just before the phaco tip is removed from the eye.
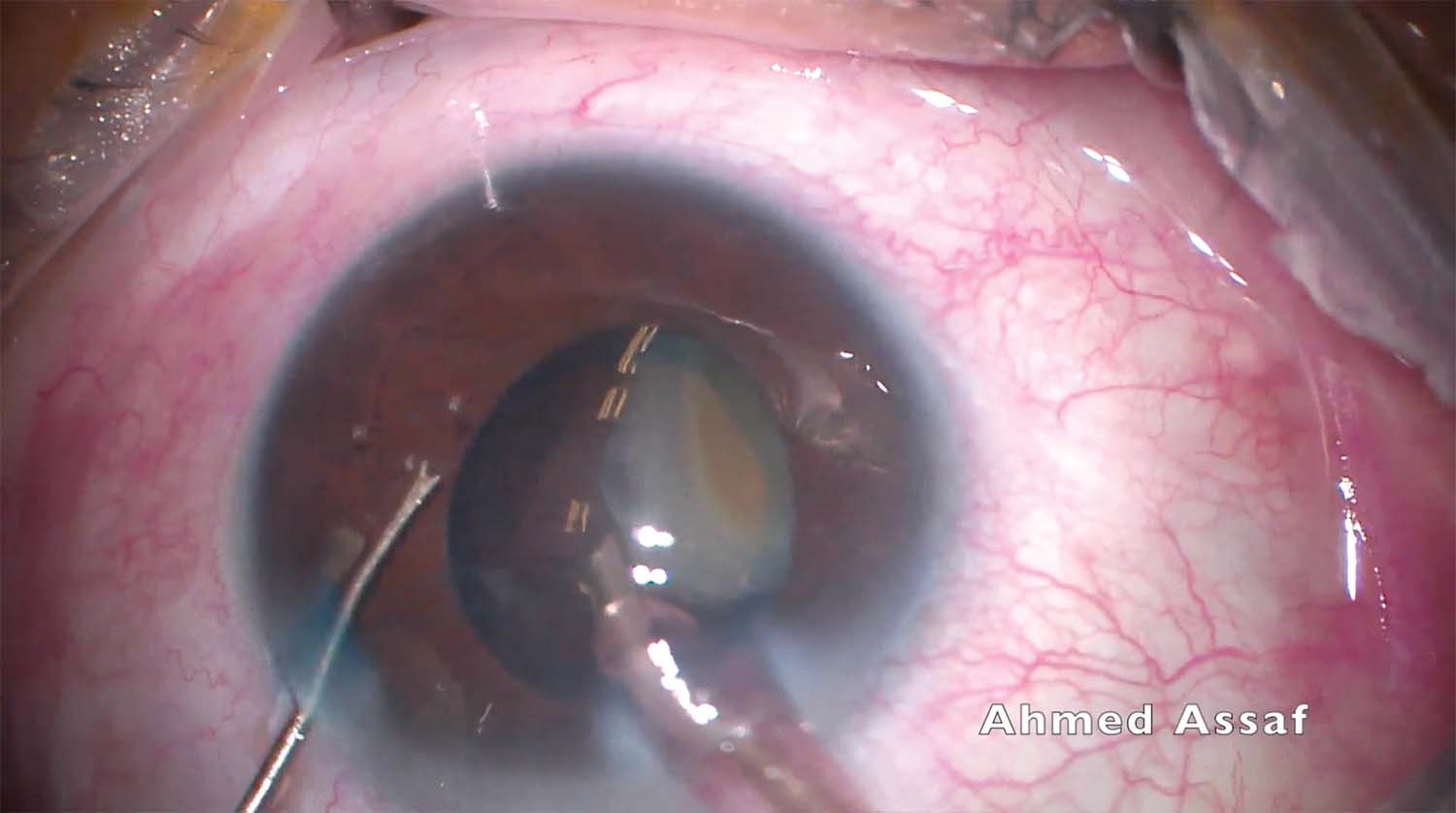
3. A Tobias Neuhann Chopper and a Thomas Neuhann Nucleus Rotator (both from Geuder) are used in an attempt to retrieve the fallen nuclear fragment. The intact posterior capsule over the fragment prevents the maneuver.
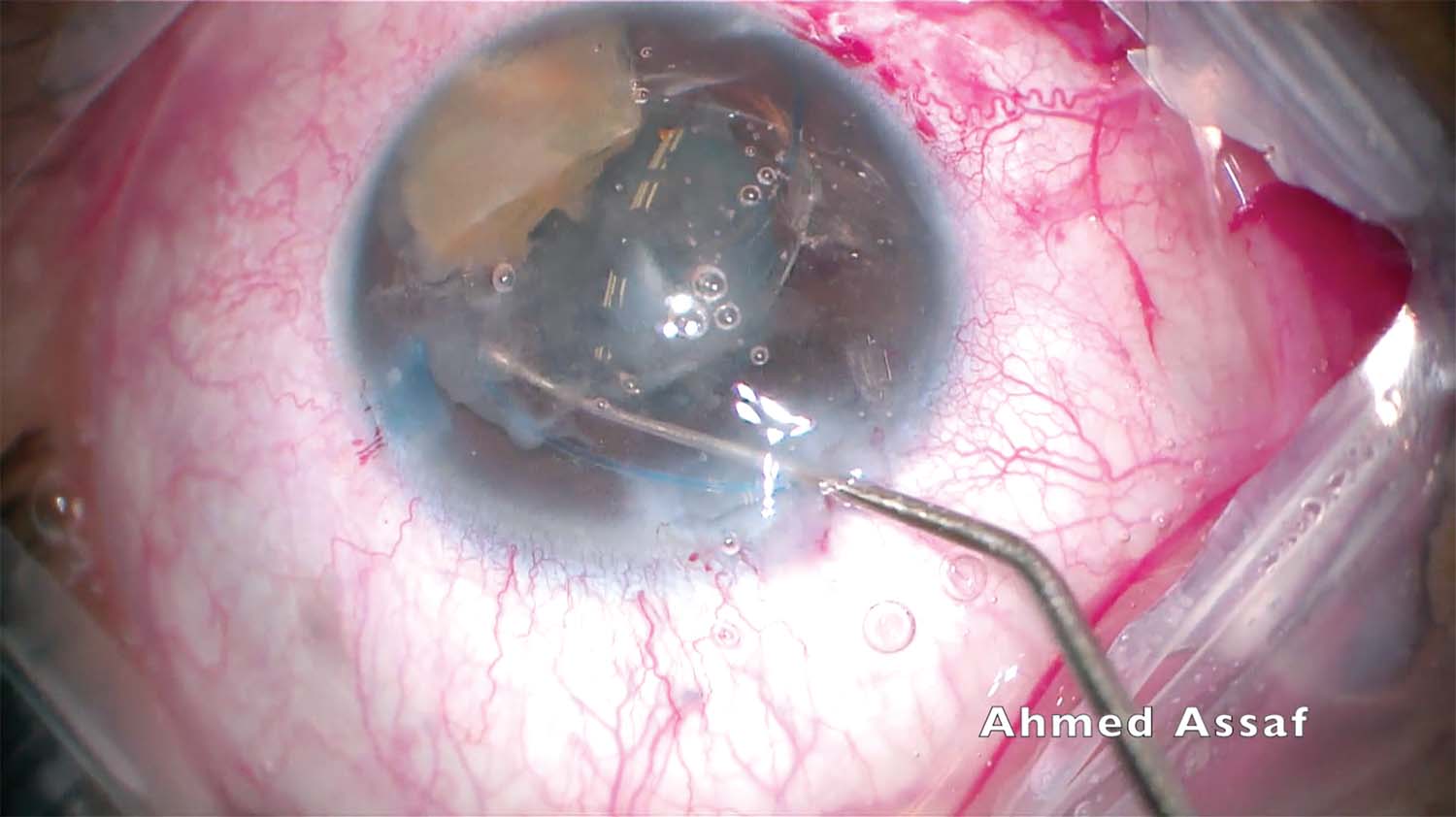
4. The posterior capsule is opened with a microvitreoretinal blade. A dispersive OVD is injected to tamponade the vitreous. An attempt is made to turn the iatrogenic puncture into a posterior capsulorhexis, but zonular weakness prevents the maneuver.
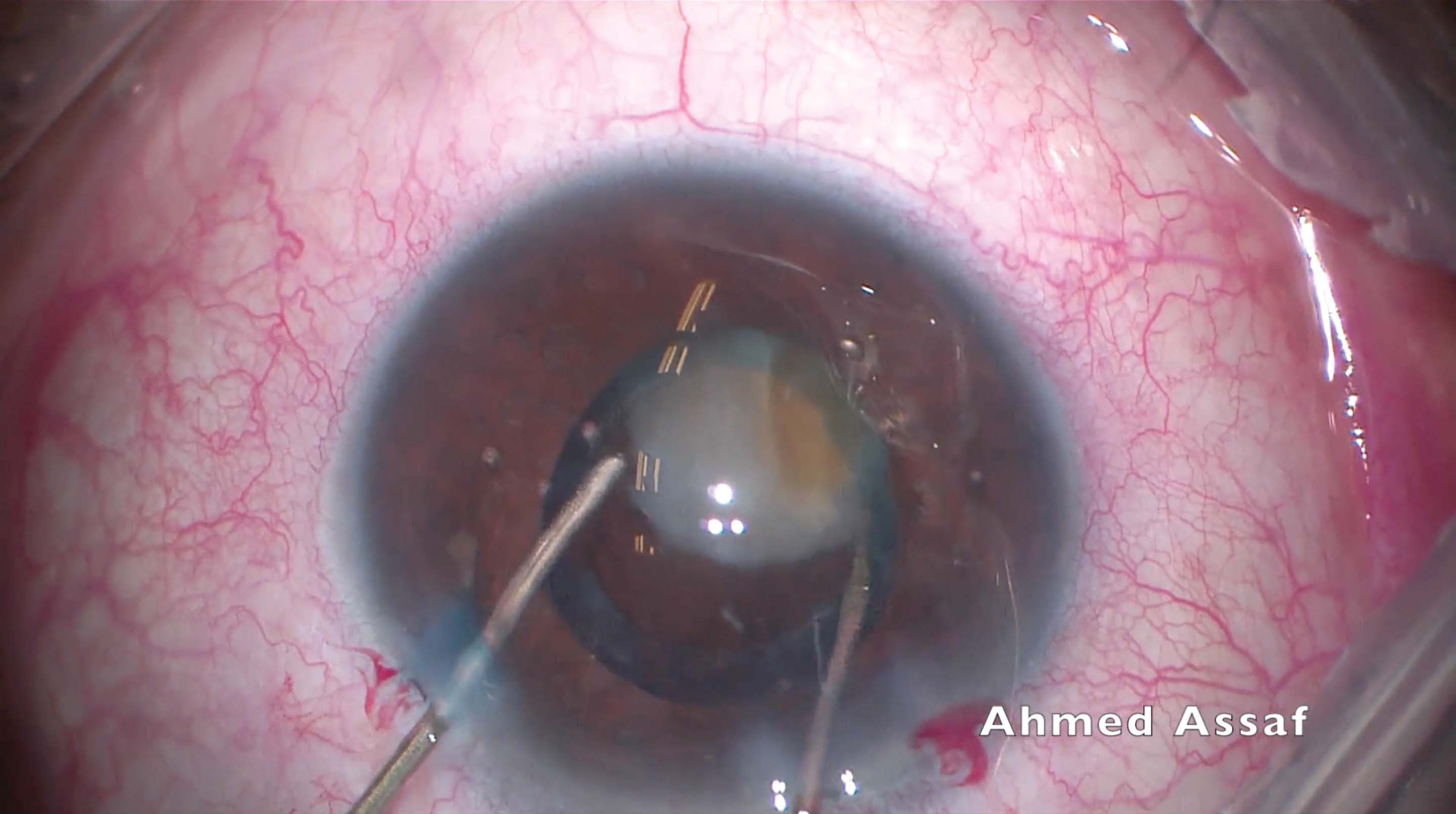
5. A posterior-assisted levitation technique is used to bring the fallen nuclear fragment into the anterior chamber, above the iris plane, and a three-piece IOL is implanted in the anterior chamber to act as a scaffold.
6. The bottle height is lowered, fluidics and ultrasound settings are reduced, and phacoemulsification is completed. A generous amount of OVD is injected to protect the corneal endothelium.
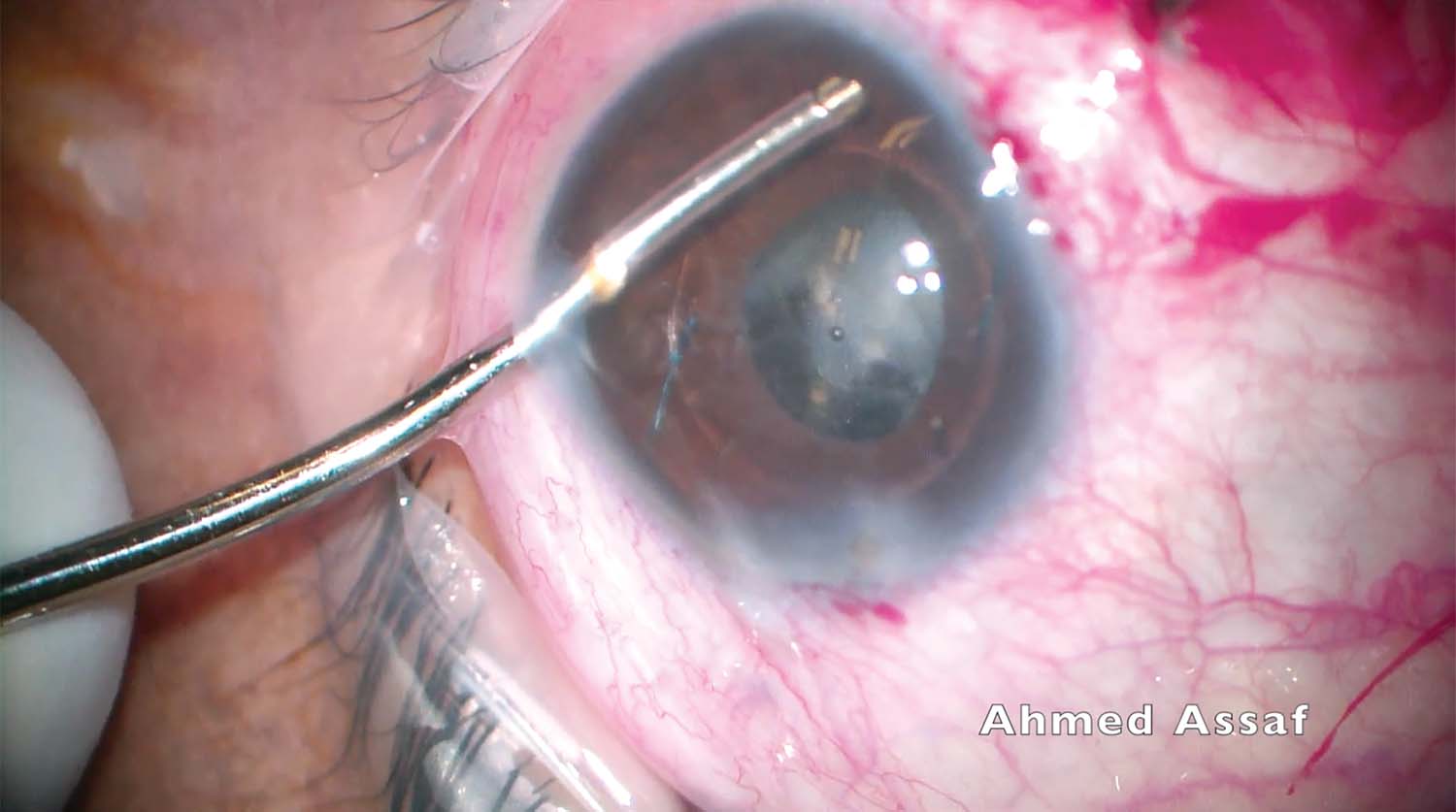
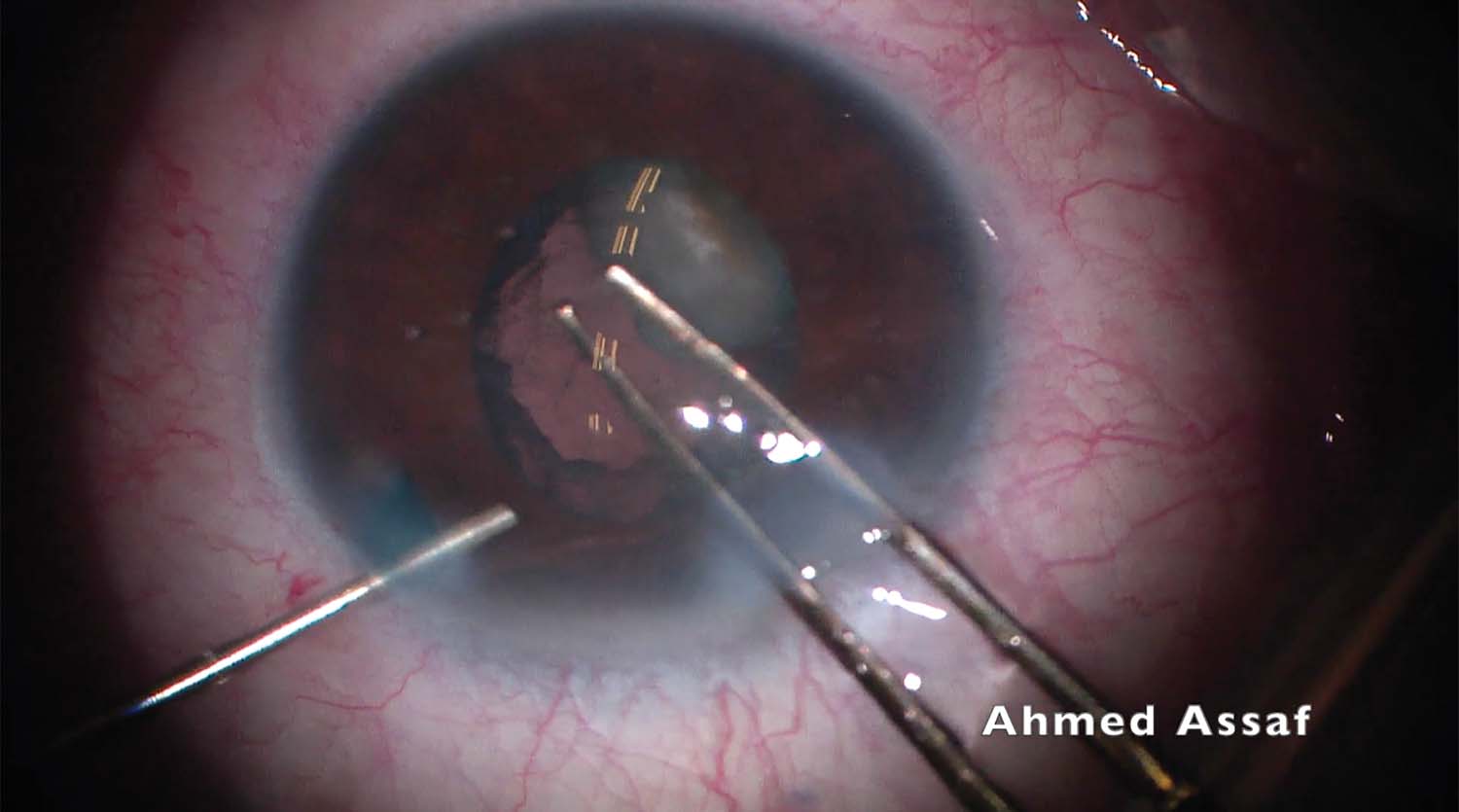
7. A pars plana anterior vitrectomy is performed through the inferior sclerotomy to remove cortical remnants from the posterior capsule. A limbal approach provides greater access to the cortex in some locations.
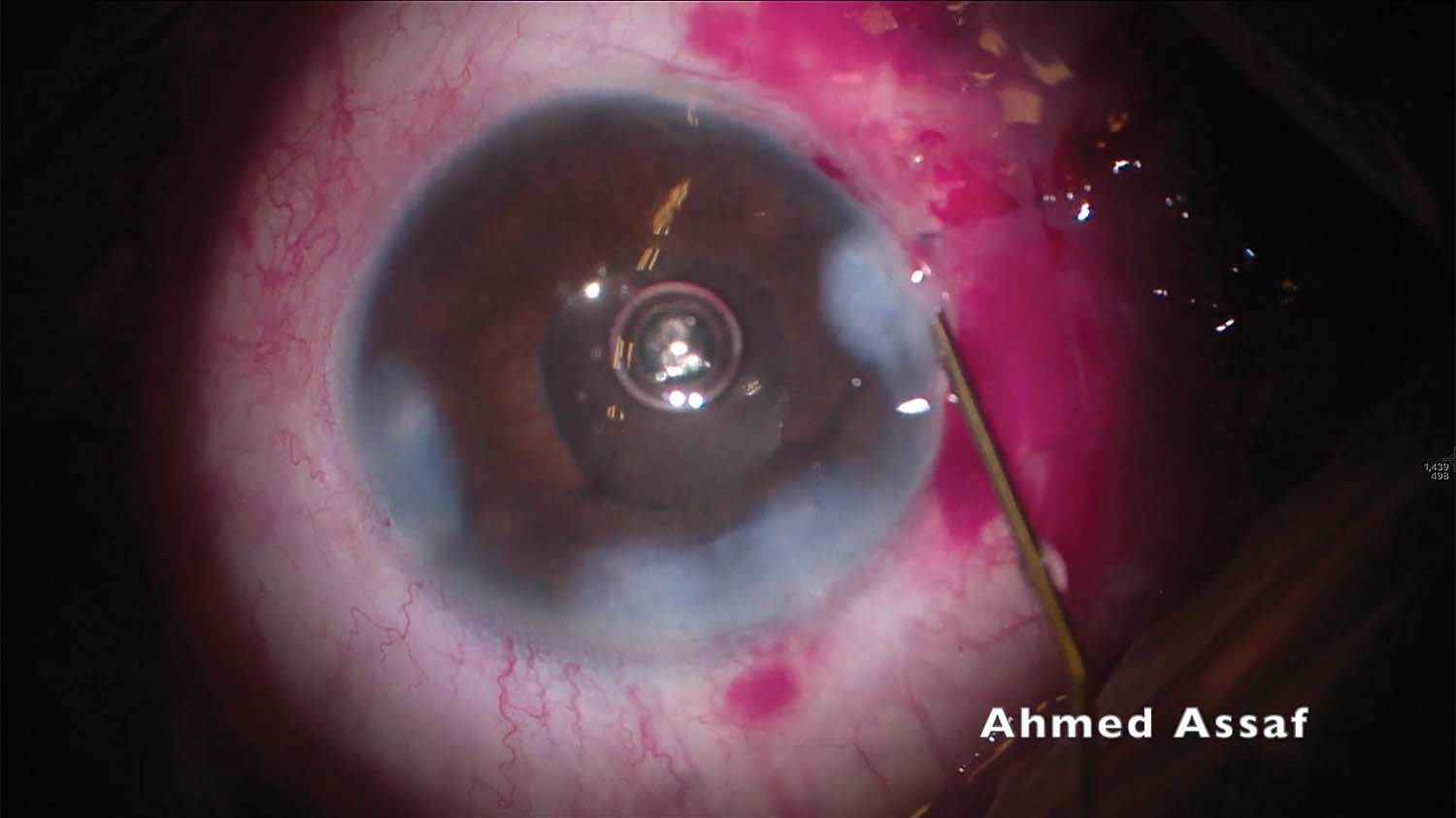
8. An IOL is implanted in the sulcus. The capsule, however, is flaccid. The IOL haptics are placed into the sulcus one at a time followed by optic capture of the lens.
9. At first glance, the IOL appears to be stable in the sulcus. On closer inspection, however, the optic edge can be seen through the narrow pupil, indicating that the IOL has tilted considerably.
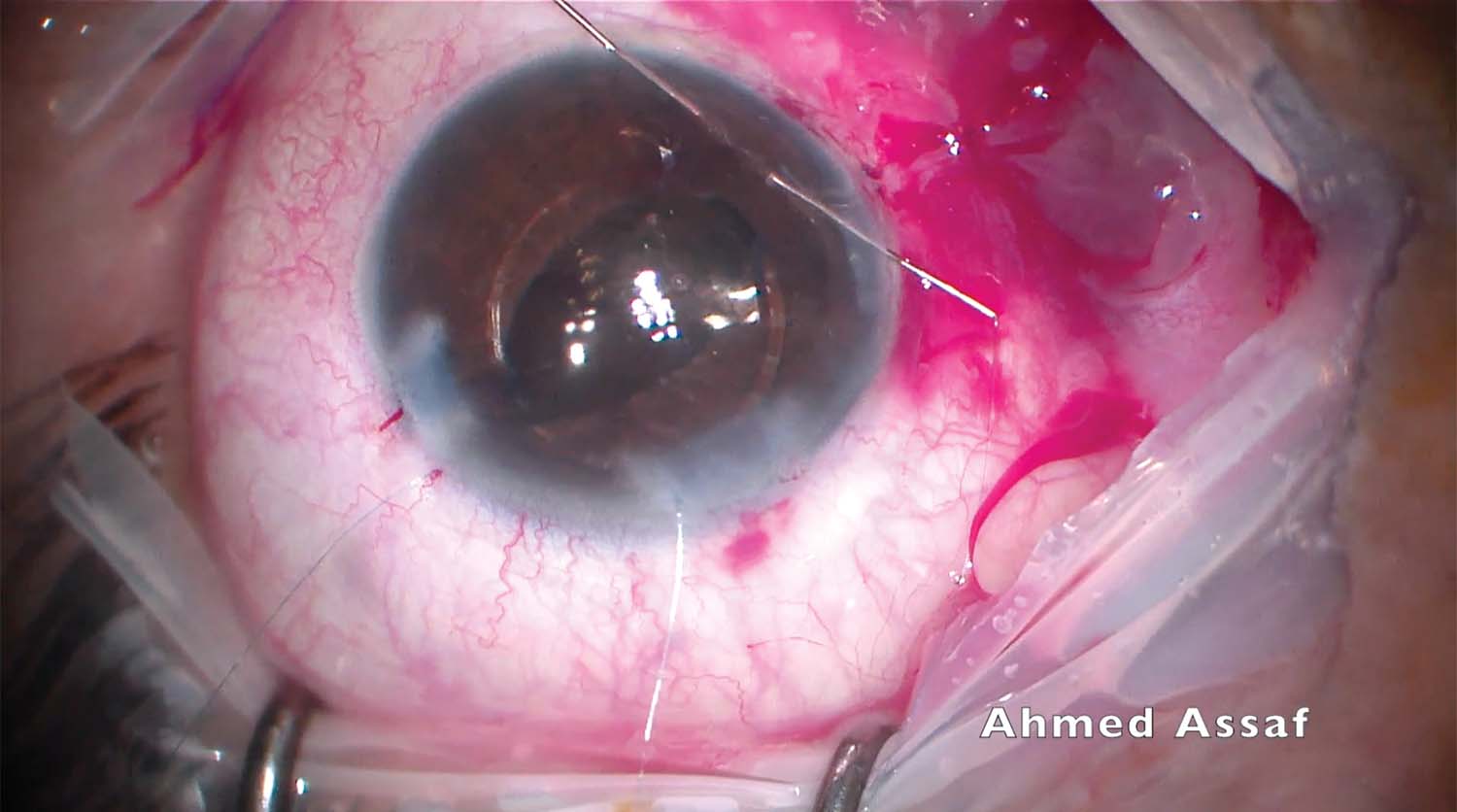
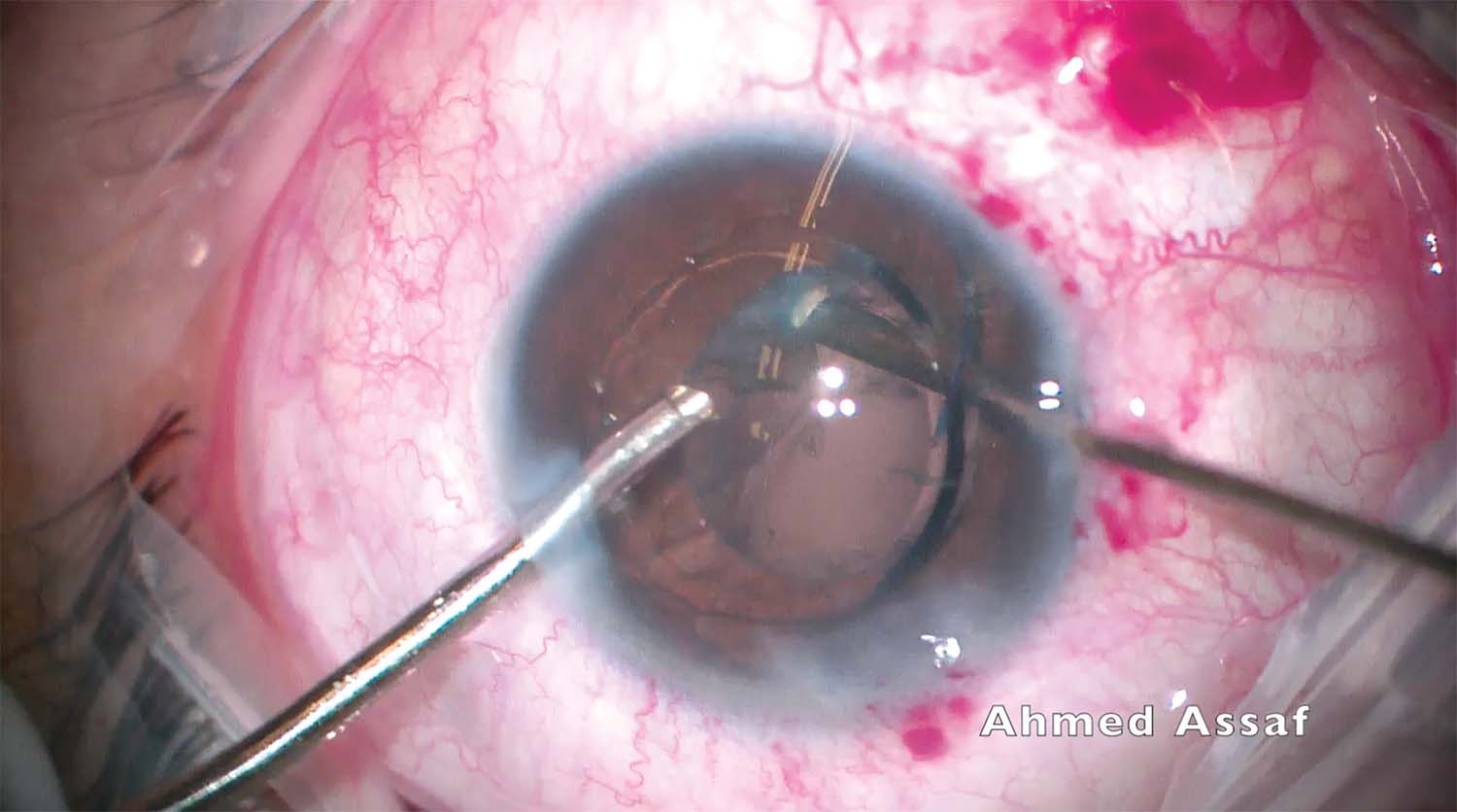
10. The IOL remains tilted despite several attempts at repositioning it. The IOL optic is pushed above the iris plane, and a modified Siepser sliding knot technique with 10-0 polypropylene (Prolene, Ethicon) sutures is used to fixate the haptics to the iris.
11. The suture knots are tied after the IOL optic is secure and the pupil is round. The sclerotomies are closed, the conjunctiva is sutured, and the corneal wounds are hydrated.

