


Any surgeon who uses a coaxial I/A tip has likely had difficulty removing subincisional cortex at one time or another. This step of cataract surgery can be challenging because the position of the I/A tip can obscure visualization of the cortical material underneath. Employing several strategies in a stepwise fashion can facilitate the removal of subincisional cortex in most situations.
1. Identify the Cause of Difficulty
If removing the subincisional cortex is challenging, identify the reason and determine whether and how best to continue maneuvering. If the cause of difficulty is a long incision tunnel, an anterior capsulotomy with a narrow diameter, or a small amount of residual cortex at the periphery, I use an OVD to move the cortex. This strategy is outlined in fundamental No. 4. Otherwise, the strategies outlined in fundamental Nos. 2 and 3 should be effective. Remember that unintentional movement of the I/A tip can cause corneal damage such as endothelial cell loss, corneal deformation, and even posterior capsular rupture.
2. View the Subincisional Cortex
Many surgeons prefer to remove the subincisional cortex first, but it is reasonable to begin by removing cortex from areas where it is most accessible. Even if you start aspiration in the subincisional area, a small amount of cortex may be left behind. If you think the amount and location of the residual cortex is manageable, you can continue to remove it in the usual manner.
If, however, the I/A tip is not aspirating the residual cortex, don’t hesitate to remove the instrument from the eye in order to confirm the position and amount of residual subincisional cortex (Figure 1). You can then reposition the I/A tip accordingly. I prefer to reinsert the I/A tip in the anterior chamber without irrigation to avoid pushing cortex away.
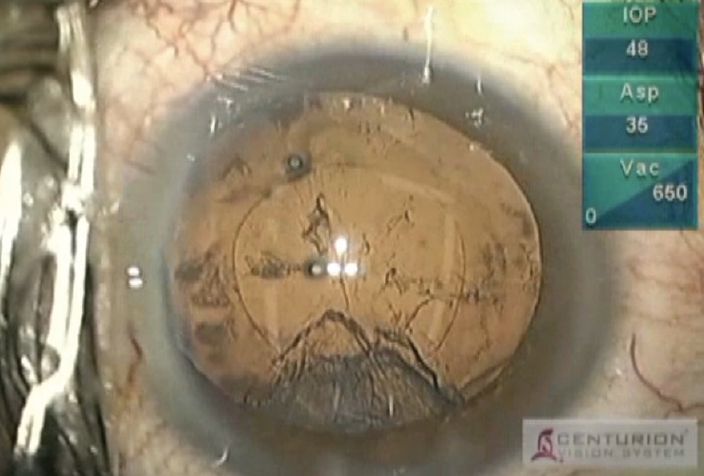
Figure 1. Posterior capsular opacification in a uveitic eye.
3. Position the Aspiration Port and I/A Tip
I use an angled I/A tip (Figure 2) because it allows me to visualize the cortex beneath it and I find it easier to place the aspiration port under the anterior capsule.
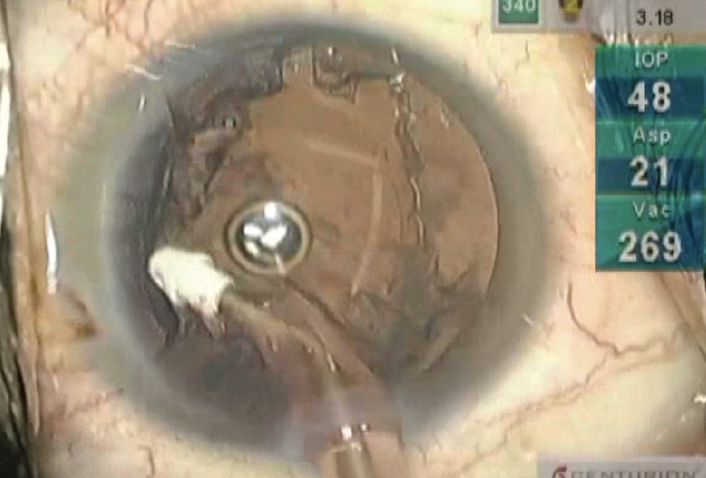
Figure 2. An angled I/A tip.
Keep in mind that there is space between the posterior capsule and the aspiration port when the I/A tip is in a vertical position (Figure 3). Aspiration can begin when the aspiration port is in direct contact with the cortex. If direct contact is lacking, rotate the I/A tip clockwise or counterclockwise to catch the cortex. This movement is easier to learn by watching video demonstrations by experienced surgeons or by assisting the surgeon directly under the operating microscope. In the latter situation, you can also observe the movement of the surgeon’s hand with the I/A tip while it is aspirating the cortex that is the most difficult to reach.
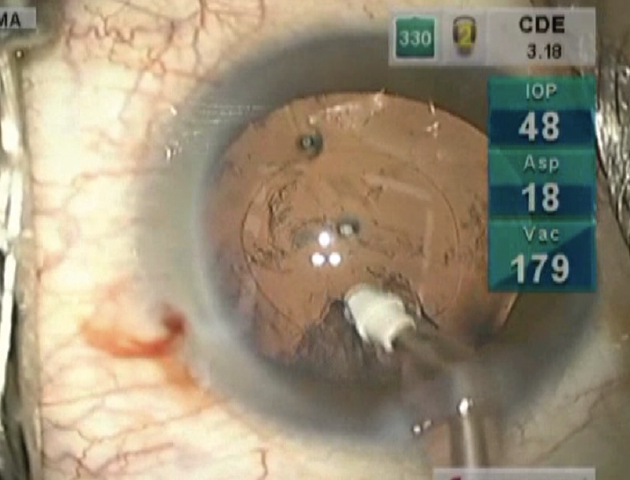
Figure 3. The I/A tip in a vertical position.
Surgeons in training tend to push the I/A tip toward the posterior capsule instead of rotating the I/A tip or their placement of the I/A tip is too shallow, leaving the aspiration port over the anterior capsule. In both scenarios, aspiration of the residual cortex is likely to be incomplete, and the posterior capsule may be inadvertently engaged and subsequently rupture. If cortical cleanup seems to be exceedingly difficult or if folds are observed in the posterior capsule, remove the I/A tip from the eye and employ the strategy described in fundamental No. 4.
4. Use OVD to Move the Subincisonal Cortex
OVDs can be useful tools for removing cortex from any location that is difficult to reach. Injecting an OVD can move cortex to a location where the material is easier to aspirate. A prime example is when cortex is located under the main incision.
The position of the irrigating cannula attached to the OVD syringe is integral to the successful relocation of cortex. A poorly oriented needle may push the OVD to an undesired position. I prefer to insert the needle from the sideport and place it behind the anterior capsule, under the subincisional area. I then inject the OVD to release the cortex from the peripheral area, which can make cortical aspiration with the I/A tip much easier.
5. Remove the Subincisional Cortex After Implanting the IOL
If the strategies outlined earlier do not work, the last resort is to remove the cortex after IOL insertion. There are two ways to do this.
No. 1: Remove the cortex immediately after inserting the IOL. The OVD and IOL widen the capsular bag, facilitating placement of the I/A tip near the subincisional cortex. It’s important to insert the I/A tip with irrigation flow shut off and to place the aspiration port close to the residual cortex. This step should be complete before aspiration begins to avoid washing the OVD out through the incision.
No. 2: Use the haptics of the IOL to move the subincisional cortex. After inserting the IOL, rotate it inside the capsular bag so that the tip of the haptics pushes the cortex away from the peripheral area. I do not often use this technique because the cortex can stick to the haptics.



