


Dr. Hannan details the steps he took to achieve a near-anatomical result in a patient with a previous grinder blade injury to the globe.
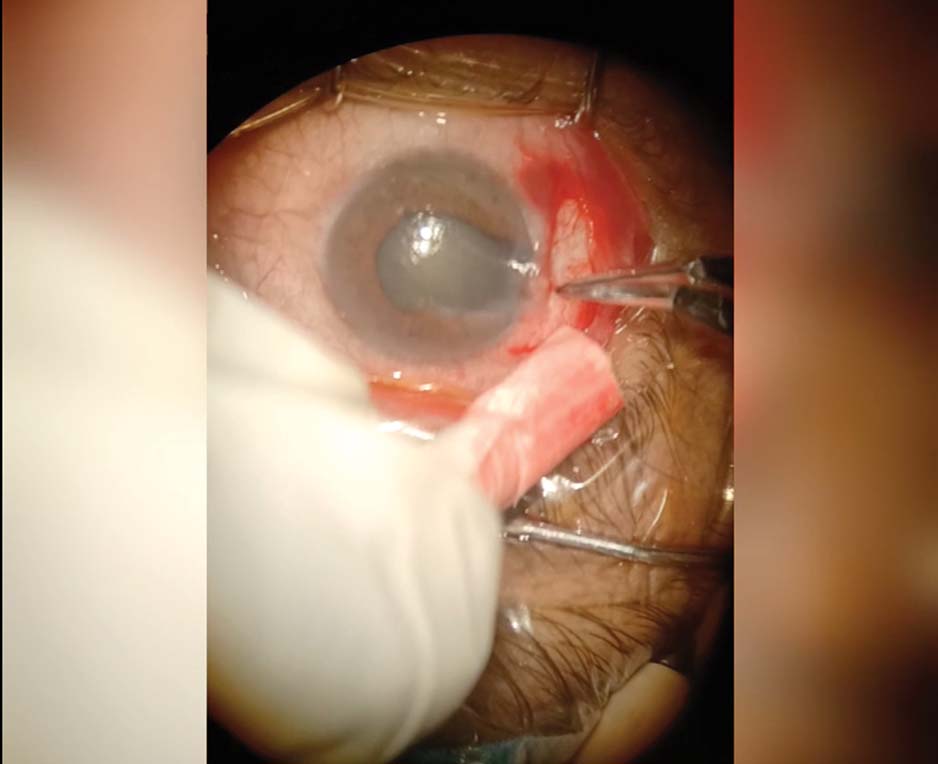
1. The patient presents with a history of a grinder blade injury to the globe; the primary repair was done elsewhere. An examination reveals a temporal iris defect that extends 2 to 3 clock hours and a nuclear sclerotic grade 3 cataract. The iridodialysis extends from the root. Three clock hours of damaged iris tissue was removed from the eye previously during a primary repair. An incision is created near the current iris defect and iridodialysis, and the wound is cauterized to keep the field clear for surgery.

2. A 3.2-mm main incision is created first, followed by a sub–3.2-mm incision near the iris defect to increase accessibility to the area of iris repair.

3. A capsulorhexis is created, and phacoemulsification is performed. Bimanual irrigation and aspiration are used to provide increased control over the floppy iris. A hydrophilic IOL is then implanted in the capsular bag.

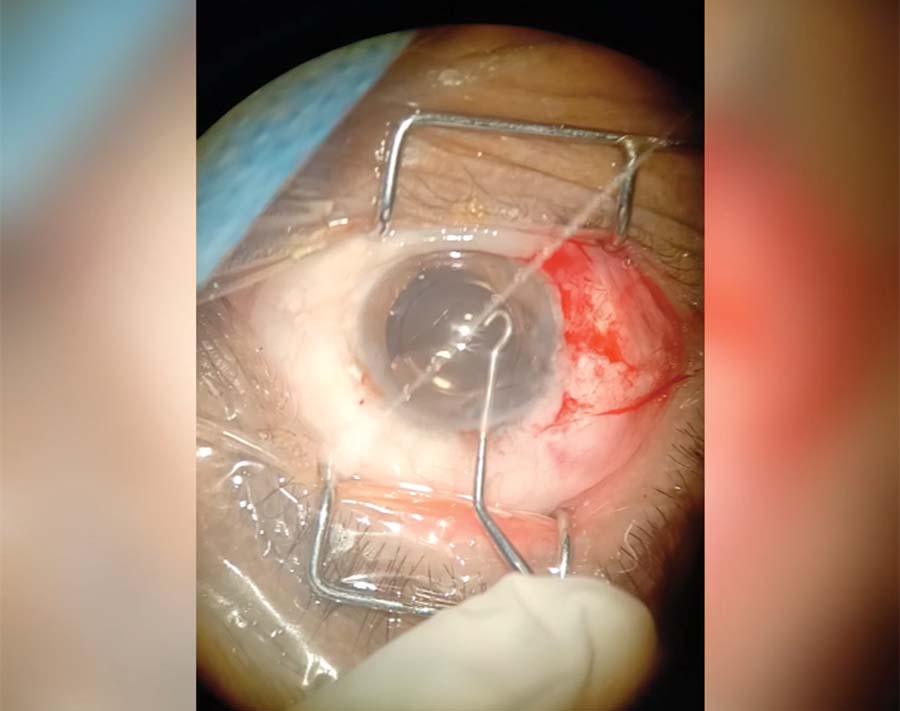
4. A straight needle threaded with 9-0 polypropylene is wiggled into the wound to prevent a corneal tissue bite and pierces the leading edge of the iris. A pair of end-grasping forceps provides countertraction for the needle to enter the iris.

5. The needle is passed through the anterior chamber to the other side of the iris and then pulled through along the direction of the bite to prevent cheesewiring of the iris tissue that can be caused by the lateral movements of a long needle barrel. A sub–3.2-mm incision is created directly in front of the exiting pathway of the needle, and the needle enters the docking irrigation cannula so that it does not bite into the cornea while it exits the eye.
6. A hook-shaped instrument is used to pass the suture from inside the eye, through the primary incision, and outside the eye. Extraocular Siepser knots are used to tie both ends of the suture.

7. The iris is slowly tied together. The force applied to the sutures is titrated to prevent cheesewiring of the already atrophic iris tissue. Close attention is paid to the site of the iris bite.
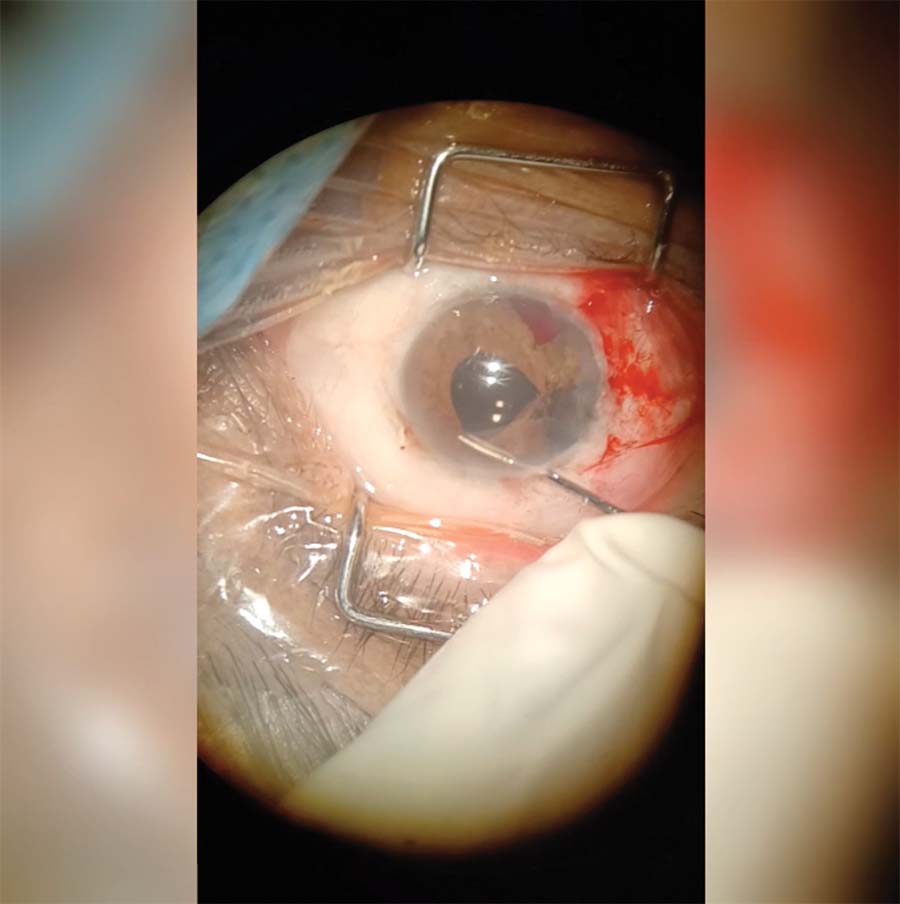
8. The end-grasping forceps are used to pull the healthy iris tissue toward the center, relieving the tension from the area under the most stress. Multiple bites are taken and subsequently closed with a Siepser knot.

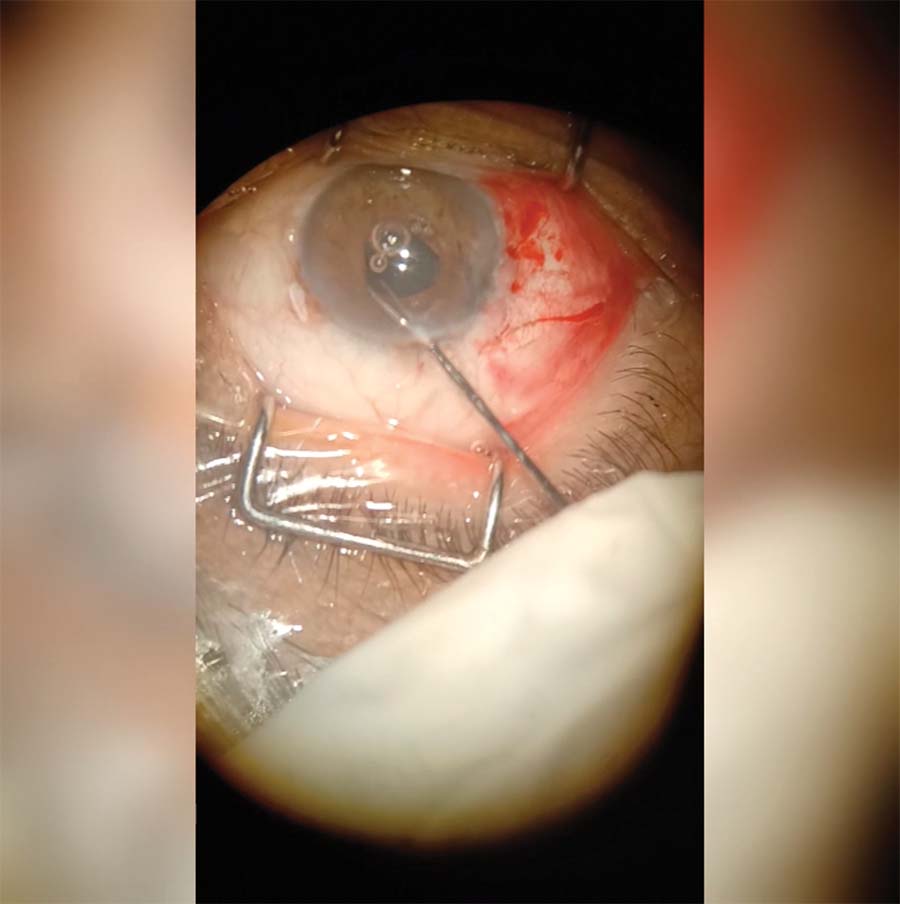
9. The pupil is decentered. Several bites are taken from the iris root. The needle is passed first extraocularly to intraocularly and then intraocularly to extraocularly. The knot is tied and then rotated and buried in the sclera to round out and center the pupil.

10. A 27-gauge needle is inserted into the eye at the margin of the uprooted iris to provide countertraction and an exit pathway for the needle. This trick is used to avoid having the needle travel blindly through the eye.

11. The suture ends are tied carefully and slowly to avoid uprooting the iris from the other side, and the knot is rotated and buried in the sclera.

12. The hemorrhages and remaining OVD are removed from the anterior chamber with bimanual irrigation and aspiration.

13. A final bite is taken out of the iris to shorten the pupillary structure and to ensure its roundness.
14. The shape of the pupil is checked. The sutures are cut with Vannas scissors, the wounds are hydrated, and 0.1 mL moxifloxacin is instilled intracamerally. Lastly, the conjunctival wound is sutured with an inverted 7-0 polyglactin suture.

