


Dr. Christenbury removes a dense posterior capsular plaque with retinal microforceps while preserving the posterior capsule after extracting an intumescent white cataract.
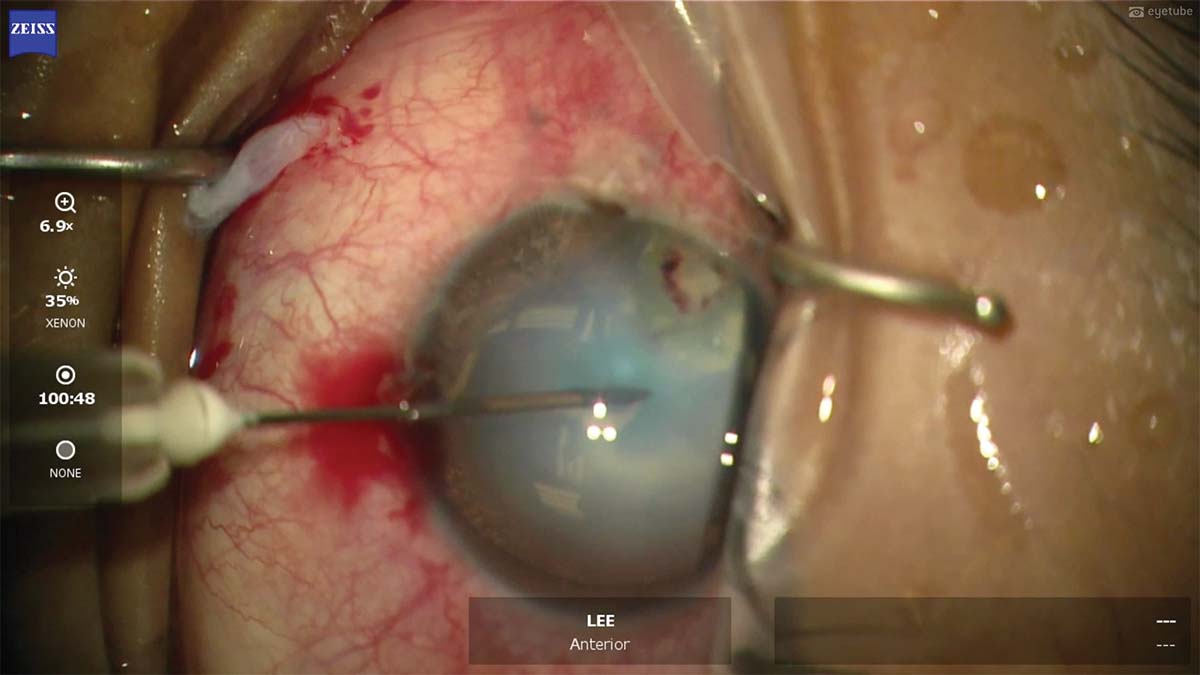
1. The patient presents for cataract surgery 3 months after undergoing ruptured globe repair elsewhere. The capsule is stained with trypan blue dye, and a 27-gauge needle is used to decompress the intumescent white cataract.
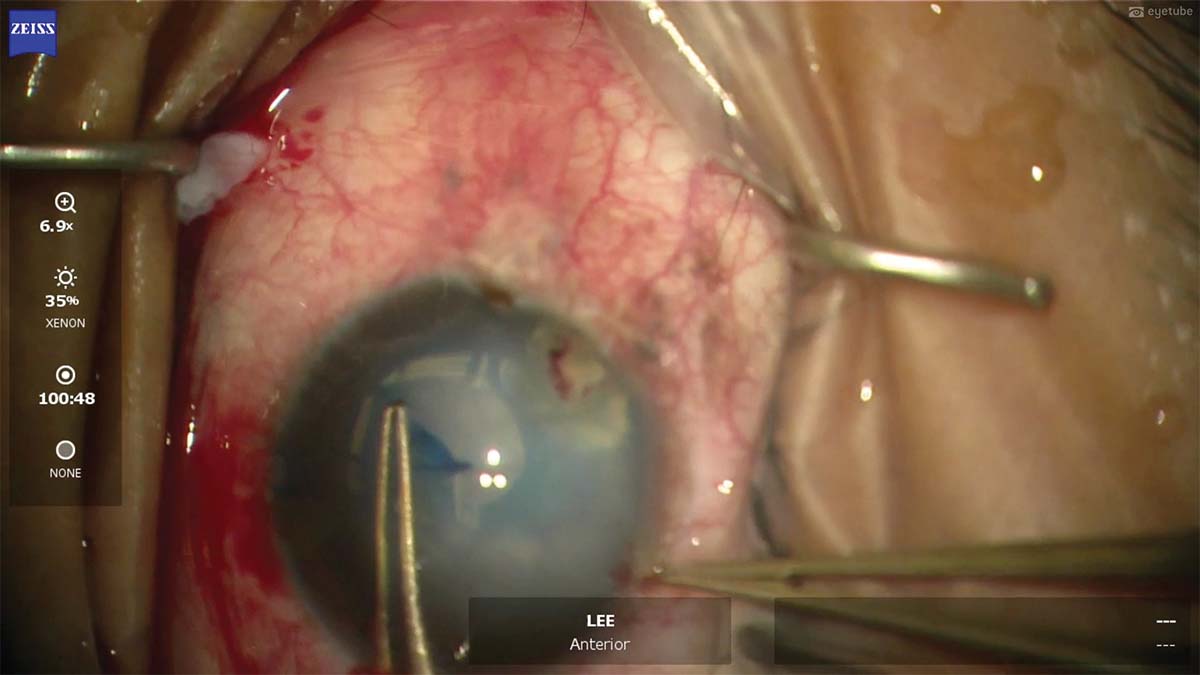
2. As the capsulorhexis is created, a second pair of forceps is used to grasp the sclera to provide countertraction and better grasp the anterior capsule.
3. The capsulorhexis runs out beneath the incisions. A cystotome is used to make another nick in the anterior capsule, and the capsulorhexis is completed from the other side. The anterior capsulorhexis is still intact.
4. An opacity in the nasal-posterior area of the lens raises suspicion that the posterior capsule has been violated. Viscodissection is performed, and the nucleus comes out easily with little phaco energy.
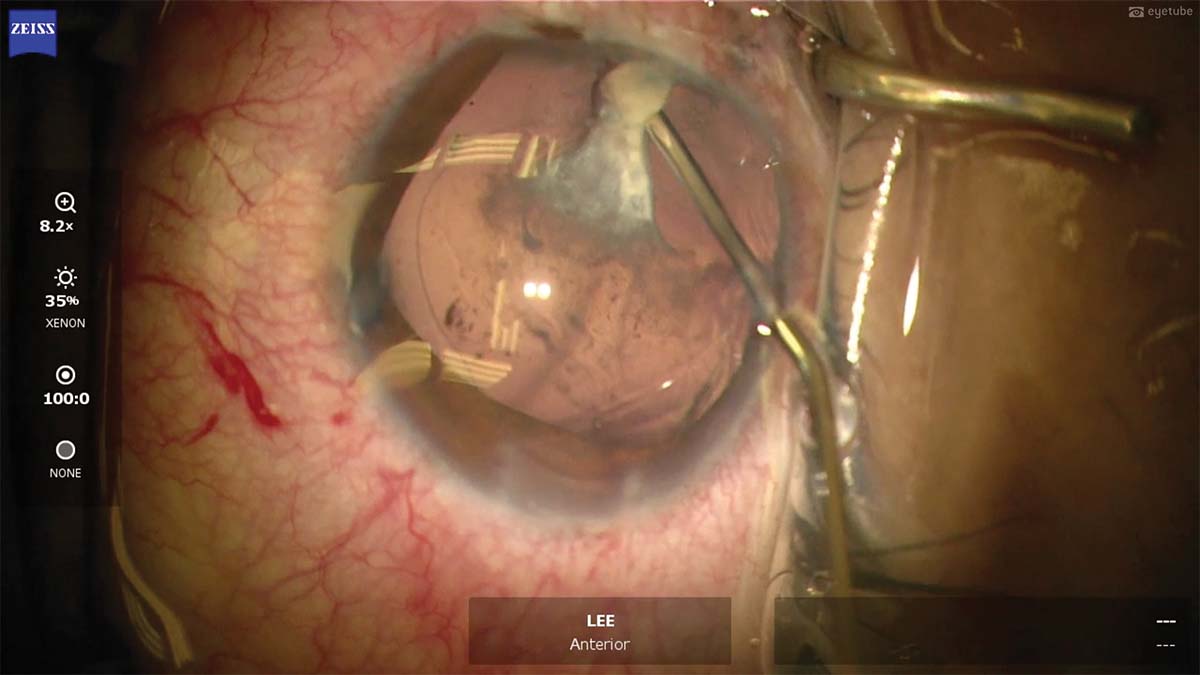
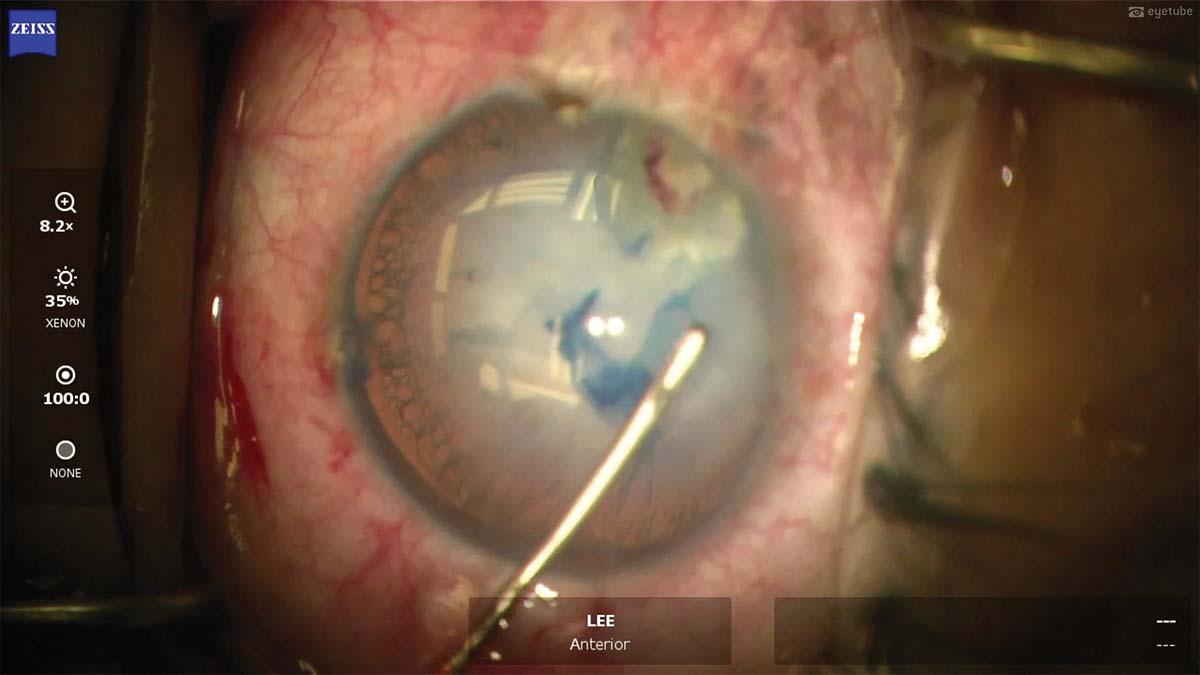
5. A dense posterior plaque is adherent to the intact posterior capsule. An OVD is injected behind the plaque, dissecting it from the posterior capsule.
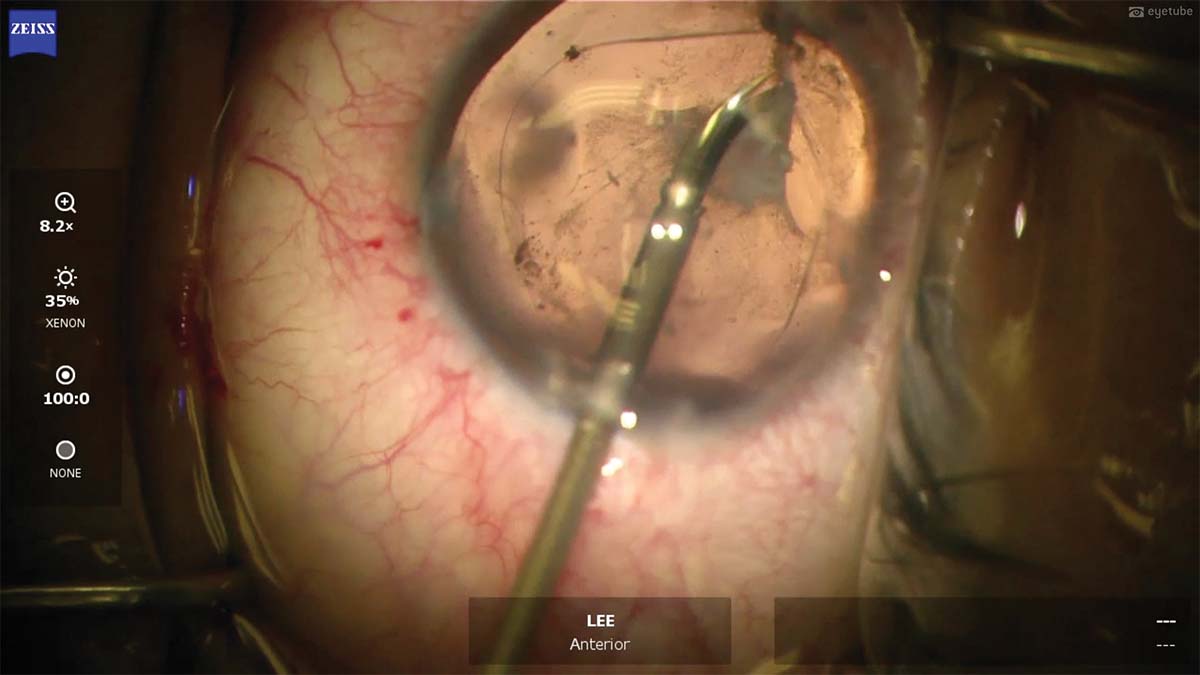
6. Intraocular scissors are used to detach the plaque from the equator and the anterior portion of the lens capsule.
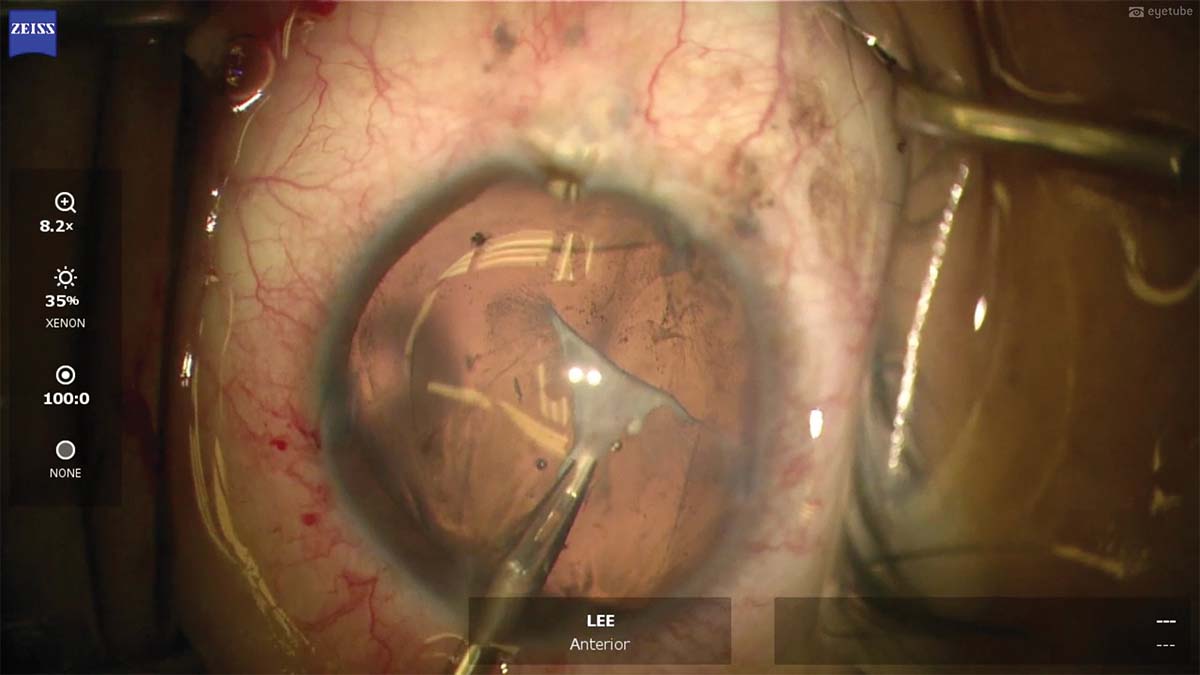
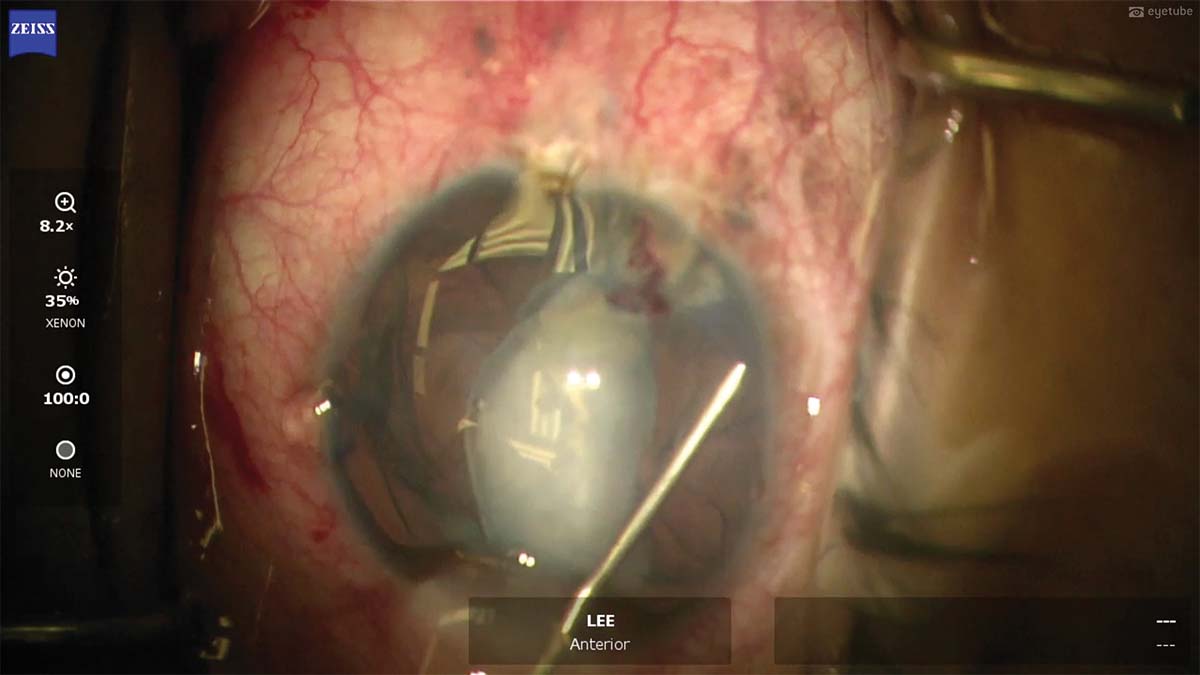
7. The dense plaque is peeled from the posterior capsule with 25-gauge forceps. The maneuver is performed slowly and gently to remove all of the plaque.
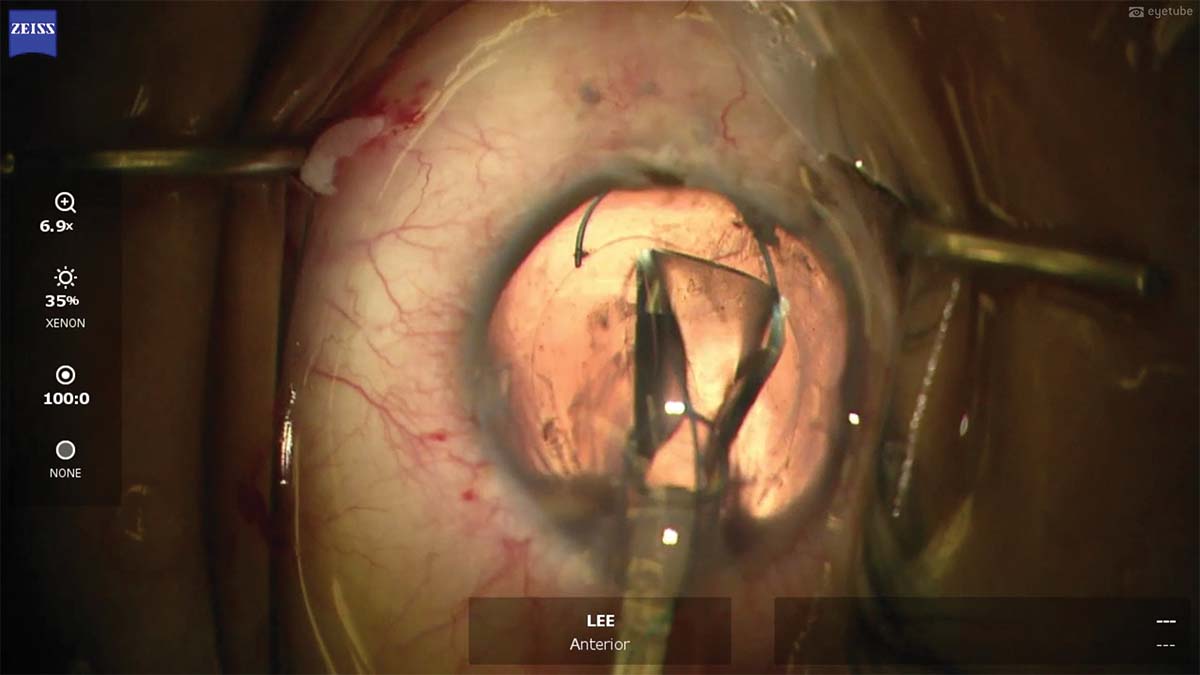
8. A three-piece IOL is implanted and rotated into the capsular bag. The lens centers nicely. The OVD is removed from the eye, and the main incision is closed with 10-0 nylon sutures to ensure proper wound closure.

