
Surgical management of ectopia lentis is one of the major challenges faced by cataract surgeons today. Ectopia lentis signifies a displacement or malposition of the crystalline lens, irrespective of cause. It may occur congenitally or as part of developmental anomalies, as found in Marfan syndrome, homocystinuria, Ehlers-Danlos syndrome, hyperlysinemia, sulfite oxidase deficiency, simple primary ectopia lentis, and congenital aniridia syndrome.1,2 Pseudoexfoliation syndrome (PXF) is probably the most common cause of adult-onset zonular dehiscence. Subluxation may also result from blunt external trauma or iatrogenic zonular dehiscence during complicated cataract surgery.3,4 This article offers five pearls for managing these challenging cases.
At a Glance
• Ectopia lentis signifies a displacement or malposition of the crystalline lens.
• Pseudoexfoliation syndrome is probably the most common cause of adult-onset zonular dehiscence.
• In patients with subluxated lenses, a comprehensive ophthalmic examination should assess both the anterior and posterior segments.
• In ectopia lentis, the phacoemulsifcation technique used depends on the degree of zonulopathy and its underlying pathophysiologic origin.
CLINICAL EVALUATION
Proper evaluation of patient history—including family history, relevant trauma history, and history of onset with vision-related symptoms—is the first step in the clinical evaluation of patients with ectopia lentis. Phacodonesis, an important sign of subluxation, is best evaluated in undilated or fully dilated pupils. The ophthalmic examination should be comprehensive and assess both the anterior and posterior segments.
Hoffman et al5 classified the degree of subluxation into three broad groups: (1) minimal to mild subluxation, in which the lens edge uncovers 0% to 25% of the dilated pupil; (2) moderate lens subluxation, in which the lens edge uncovers 25% to 50% of the dilated pupil; and (3) severe subluxation, in which the lens edge uncovers more than 50% of the pupil.
It is best to examine a patient with a severely subluxated lens in both upright and supine positions. The change in the position of the lens with different head positions helps to indicate the severity of subluxation.
The degree of zonular loss may be localized, as in focal trauma or congenital defects, or there may be an extensive generalized weakness of zonular fibers, as in Marfan syndrome or PXF. A round lens edge indicates total loss of zonules or lax zonules.
The already difficult situation of lens subluxation may become more challenging in the presence of a hard cataract, a rigid pupil, an iris coloboma, vitreous in the anterior chamber, anterior subluxation of the lens with a very shallow anterior chamber, or a very deep anterior chamber as in myopia.
SURGICAL PLANNING
In these types of cases, local anesthesia is preferable over topical anesthesia. Preoperative intravenous mannitol (1,000 to 2,000 mg/kg of body weight) can reduce vitreous-associated complications during surgery.
In eyes with ectopia lentis, the phacoemulsification technique used depends on the degree of zonulopathy and its underlying pathophysiologic origin. When the zonular abnormality is less than 3 contiguous clock hours, slow and careful surgery may be sufficient for a successful surgical outcome, with adjunctive support from capsule retractors. When the area of zonular dialysis is small, with otherwise strong zonular attachment elsewhere, as in trauma, a capsular tension ring (CTR) may not be routinely required.
On the other hand, the use of a CTR is mandatory even in mild cases of zonular laxity that have a progressive pathologic nature, as in PXF, Weill-Marchesani syndrome, Marfan syndrome, or retinitis pigmentosa. These are cases in which the zonular pathology worsens with time, and the CTR can be helpful for secondary fixation of the bag if necessary. It is wise to implant a CTR in every case in which zonular disturbance is suspected.
In younger patients with such risk factors, bag fixation to the sclera with a capsular tension segment (CTS) is advisable from the beginning. The operating surgeon is the ultimate judge, but he or she should remain flexible in these cases and be prepared to handle a greater degree of difficulty than anticipated during the preoperative assessment.
The remainder of this article focuses on five pearls for this challenging surgery.
Fundamental 1. INCISION
The modern cataract surgeon is likely accustomed to using a clear corneal temporal incision. The dictum in eyes with lens subluxation is that the main incision should not lie directly over the area of zonulopathy when possible. The paracentesis wound for a second instrument should be more corneal to prevent injury to the rhexis margin, which tends to be slightly anteriorly tented after fixation of iris hooks.
Management of preexisting vitreous prolapse in the anterior chamber must be done at the beginning of surgery. This can be accomplished with triamcinolone-assisted two-port anterior vitrectomy. In this situation, the capsular bag must be supported with hooks, even if the area of subluxation is small.
Fundamental 2. CAPSULORRHEXIS
The capsulorrhexis is the most challenging step of cataract surgery in eyes with ectopia lentis because capsulorrhexis completion and bag preservation are mandatory for successful phacoemulsification. Both initiation and completion of the capsulorrhexis are more demanding in this setting than in standard cases. Making the first puncture is difficult due to a lack of zonular countertraction and to the highly elastic capsules seen in comparatively young eyes.
Staining of the capsule with trypan blue dye can aid in this situation, as the dye reduces the elasticity of the capsule and makes penetration of the capsule easier.6 Caution is needed in the event of a loss of the anterior-posterior barrier due to zonular deficiency, as trypan blue can stain the vitreous, leading to a loss of the red reflex after simple irrigation of the dye into the anterior chamber. It is safer to paint a few drops of dye directly across the anterior capsule under an ophthalmic viscosurgical device (OVD).
The first capsular puncture can be made with a standard cystotome or a straight 25-gauge needle (Figure 1). If this cannot be done easily, the crossed-swords capsule pinch approach using two 180° opposing 30-gauge needle tips can be used to pierce the capsule and create a starting point for the capsulorrhexis.
In most unstable lenses, microforceps or a hook may be used to provide countertraction during the continuous tear of the capsule. This second instrument should be placed at least 2 to 3 clock hours from the leading edge of the capsulorrhexis to avoid runaway (Figure 2). An eccentric rhexis can be made according to the shape of an eccentric lens to ultimately achieve a round, central rhexis. In extreme situations, microincision forceps can be useful to access the capsule from multiple microincision paracenteses around the circumference.
The ideal capsulorrhexis should have at least a 2-mm margin between the capsulorrhexis edge and the lens equator to adequately support the CTR, Cionni ring, or Ahmed CTS (all available from multiple manufacturers) in the capsular bag.
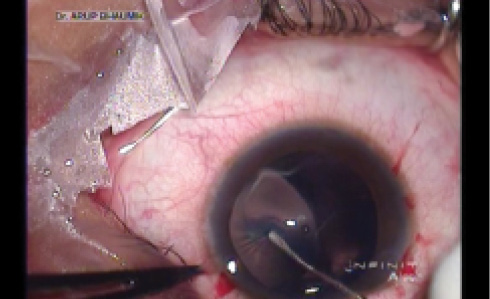
Figure 1. Puncture of an elastic anterior capsule with a longtipped cystotome.
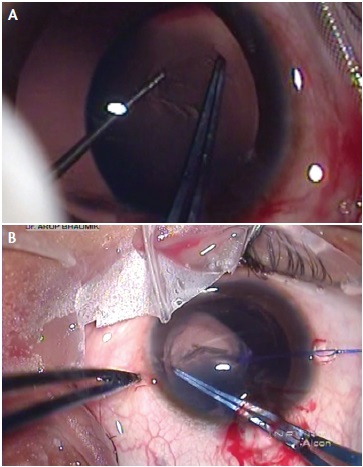
Figure 2. Countertraction with a Kuglen hook during capsulorrhexis creation (A) and countertraction with an iris hook and centration of a subluxated lens (B).
Fundamental 3. STABILIZATION OF THE CAPSULAR BAG
If zonular dysfunction involves a large area, for instance in the range of 3 to 6 clock hours, then the capsule must be supported during surgery. This can be done using flexible iris retractors strategically placed through limbal stab incisions to hook the capsulorrhexis edge and support the bag (Figure 3).7 The disadvantage of this approach is that the hook ends can inadvertently tear the rhexis edge. They also tend to bring the capsular bag into a more anterior plane, and sometimes in extreme subluxation the lens itself can be in the anterior chamber. Capsular hooks, therefore, are a better alternative, as they support the bag by its equator and keep it distended, reducing the risk of aspiration of the bag equator (Figure 4).
The capsular bag can be stabilized with an Ahmed CTS by hooking the fixation eyelet with an iris retractor (Figure 5). In patients with deep anterior chambers, a capsular hook may be placed through a prelimbal stab incision to reduce the chance of the hook slipping (Figure 6).
The best way to stabilize a compromised capsular bag is to place a CTR; this approach maintains an expanded capsular bag, supports the zonular apparatus, and can facilitate safe phacoemulsification. The primary question, however, is when to place the CTR. Some surgeons prefer to put it in early so that the weak bag is supported from the beginning. However, putting the CTR in with the lens still in the bag is challenging. Sometimes the obstructed progress of the CTR through the bag may lead to more damage to zonular fibers,8,9 and a larger area of zonular weakness may result. Additionally, cleaning of the cortex from the equator can be hampered by the CTR. Most surgeons would ideally prefer to follow this rule: Place the CTR as late as you can, but as soon as you must.5
Segmental designs with eyelets, such as the Cionni or Ahmed CTS, can be sutured to the sclera to stabilize focal defects. Alternatively, the CTS can be fixed by passing an iris hook through an eyelet.
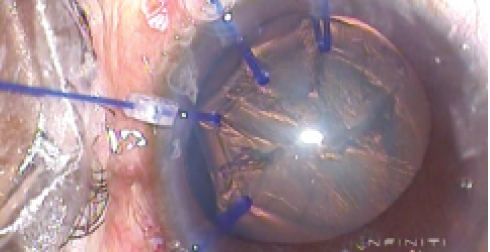
Figure 3. Capsular bag stabilization using multiple capsular hooks.
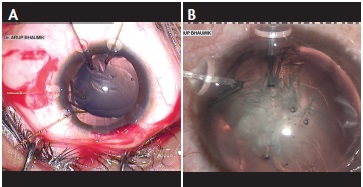
Figure 4. Capsular bag stabilization with Mackool capsular hooks (A) and MicroSurgical Technology capsular hooks (B).
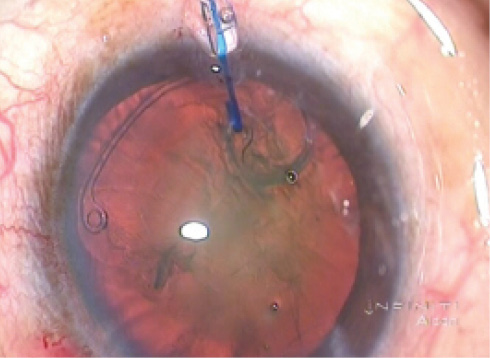
Figure 5. Stabilization of a subluxated lens is accomplished using an Ahmed CTS by hooking the fixation eyelet with an iris hook.
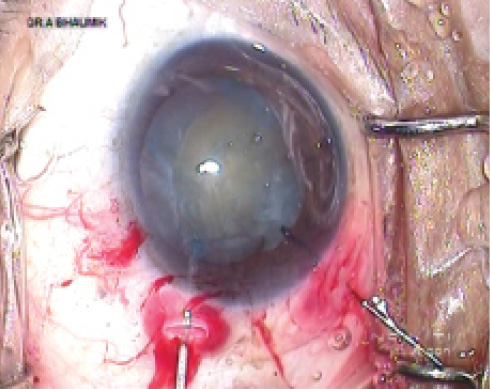
Figure 6. Capsular bag stabilization using a capsular hook placed through a prelimbal incision in a deep anterior chamber.
Fundamental 4. PHACOEMULSIFICATION
The next important phase of surgery is phacoemulsification of the cataractous lens. Zonulopathy makes the situation more difficult, as mobilization of the nucleus in the bag is nearly impossible due to a lack of countertraction. The risk of damaging the bag can be reduced with meticulous and repeated hydrodissection and viscodissection, crucial steps in this procedure. Slow-motion phacoemulsifcation with low parameters is mandatory. In this mostly younger population, cataracts tend to be soft and easily aspirated with irrigation and aspiration only. Harder cataracts are more difficult to crack. If chopping can be successfully initiated, removal of the first pie segment creates more space in the bag, thereby reducing zonular stress during subsequent chopping.
In our clinic, repeated injection of hydroxypropyl methylcellulose in the bag and anterior chamber is facilitated with the use of the Visco pump (available in India). This simple, motorized, footpedal-controlled device can be used to continuously inject OVD through a second sideport at the desired site with an irrigating cannula (Figure 7).
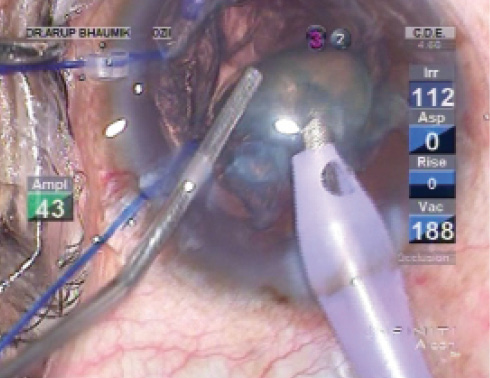
Figure 7. Injection of an OVD with a cannula placed through a second sideport incision.
Fundamental 5. LONG-TERM BAG FIXATION
Available tools for bag fixation include standard CTRs, the Cionni ring, and the Ahmed CTS. The process of selecting which tool to use is ruled by the degree of zonular damage and its chance of progression.
In the case of a small area of dialysis, a standard CTR will suffice, inserted manually or with an injector system with the vector forces directed toward the area of zonular weakness (Figure 8). If the damage is larger than 4 clock hours, with a grossly decentered bag, a standard CTR may be augmented with a CTS. This combination of a standard CTR with a CTS is likely a better option than using a Cionni ring because of their ease of insertion and fixation with less zonular stress involved. A Cionni ring should be the primary choice only if the capsulorrhexis is larger than planned.5
For long-term fixation of the bag, additional CTS anchorage over a standard CTR is necessary.
Placement of a Cionni ring, which is done in a clockwise direction, is more technically challenging. Preloading the leading eyelet with a 10-0 nylon suture makes placement around the first few clock hours much easier, adding tension to the leading suture to reduce the arc of curvature and prevent the device from hanging up in the capsular fornix.
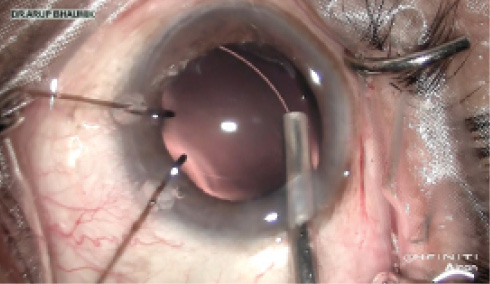
Figure 8. CTR insertion with an injector, maintaining the arc of the capsular bag.
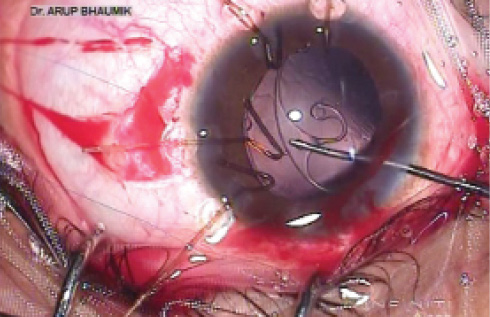
Figure 9. Implantation of an Ahmed CTS at the capsular bag equator with a hook.
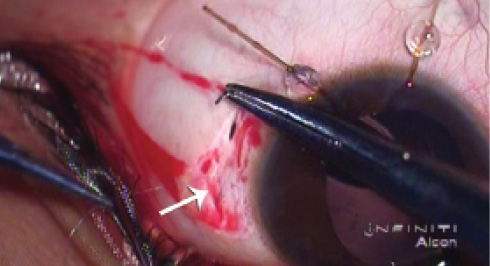
Figure 10. A Cionni ring or Ahmed CTS can be fixed to the sclera by taking multiple suture bites without a flap or knot.
An Ahmed CTS can be placed directly into the bag fornix in the desired clock hour (Figure 9). The fixation device should overhang the capsular margin anteriorly and be placed directly over the area of greatest weakness. The sutures may be placed ab interno through the scleral wall or exteriorized by making scleral pockets. Some surgeons prefer to use an ab externo technique. A temporary knot is made, and, after making the eyeball tight with an OVD, suture tension is further titrated to achieve maximum IOL centration. The final knot can be buried under a corneoscleral pocket or scleral flap. The suture can be fixed to the sclera by multiple horizontal bites without a knot (Figure 10).
Watch it Now
Watch a series of pearls for managing ectopia lentis, one of the major challenges faced by cataract surgeons.

Suture material with a more permanent nature is preferable for fixation. Whereas 10-0 polypropylene has a tendency to hydrolyze in 5 to 10 years and, thus, should be avoided,10 9-0 polypropylene has a longer survival record. However, the exact time interval of degradation is yet to be documented. Polytetrafluoroethylene (Gore-Tex CV-8; W.L. Gore and Associates) sutures have excellent longevity. Some surgeons prefer to suture a Cionni ring or Ahmed CTS to the sclera after IOL implantation to achieve better centration.
FINAL THOUGHTS
IOL selection will depend on how successfully the surgery is completed. If everything goes as planned, no rhexis damage or posterior capsular rupture occurs, and the bag is fixated centrally with a CTR or CTS, then in-the-bag implantation of a one- or three-piece foldable IOL can be performed. In the case of an absolutely centrally fixated bag, a multifocal or toric IOL may be considered. In eyes with PXF, the IOL may be implanted in the sulcus with the optic captured in the anterior capsulorrhexis.
If damage to the rhexis or a posterior capsular rent occurs, the use of a CTR or CTS should be avoided. These are extreme situations, and IOL selection must be modified, as anterior chamber, scleral- or iris-fixated, or glued IOLs are then the only appropriate options.
For a video demonstration of management of subluxated cataracts, visit http://eyetube.net/?v=apodi.
1. Merriam JC, Zheng L. Iris hooks for phacoemulsification of the subluxated lens. J Cataract Refract Surg. 1997;23:1295-1297.
2. Santoro S, Sannace C, Cascella MC, Lavermicocca N. Subluxated lens: phacoemulsification with iris hooks. J Cataract Refract Surg. 2003;29:2269-2273.
3. Ton Y, Michaeli A, Assia EI. Repositioning and scleral fixation of the subluxated lens capsule using an intraocular anchoring device in experimental models. J Cataract Refract Surg. 2007;33:692-696.
4. Cionni RJ, Osher RH. Endocapsular ring approach to the subluxed cataractous lens. J Cataract Refract Surg. 1995;21:245-249.
5. Hoffman RS, Snyder ME, Devgan U, Allen QB, Yeoh R, Braga-Mele R. Management of the subluxated crystalline lens. J Cataract Refract Surg. 2013;39:1904-1915.
6. Cionni RJ, Osher RH, Marques DMV, Marques FF, Snyder ME, Shapiro S. Modified capsular tension ring for patients with congenital loss of zonular support. J Cataract Refract Surg. 2003;29:1668-1673.
7. Vasavada V, Vasavada VA, Hoffman RO, Spencer TS, Kumar RV, Crandall AS. Intraoperative performance and postoperative outcomes of endocapsular ring implantation in pediatric eyes. J Cataract Refract Surg. 2008;34:1499-1508.
8. Ahmed II, Cionni RJ, Kranemann C, Crandall AS. Optimal timing of capsular tension ring implantation: Miyake-Apple video analysis. J Cataract Refract Surg. 2005;31:1809-1813.
9. Dietlein TS, Jacobi PC, Konen W, Krieglstein GK. Complications of endocapsular tension ring implantation in a child with Marfan’s syndrome. J Cataract Refract Surg. 2000;26:937-940.
10. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31:1320-1326.
Arup Bhaumik, MD
– Senior Consultant, Department of Cataract, Cornea and Refractive Services, Disha Eye Hospitals and Research Centre, West Bengal, India
– arupbhaumik_cal@yahoo.co.in
– Financial disclosure: Inventor (Visco pump)
Santanu Mitra, MBBS, DOMS
– Senior Consultant, Department of Cataract, Orbit & Oculoplasty, Disha Eye Hospitals, Barrackpore, West Bengal, India
– santanu_mitra60@yahoo.co.in
– Financial disclosure: None



