
When modern phaco technology is used in combination with proper surgical technique, postoperative corneal decompensation is rare. There are several patient-based factors, however, that increase the likelihood of corneal decompensation. With patients electing to have cataract surgery and refractive lens exchange at increasingly younger ages, protecting the endothelial cell layer at all times is essential to avoid the potential for an epidemic of pseudophakic bullous keratopathy (PBK) in the future. Patient expectations after cataract surgery continue to increase, and patients now anticipate perfect vision from as early as the first postoperative day. The main determinant of a patient’s visual acuity on postoperative day 1 is the extent to which the endothelium has been protected.1
SURGICAL MEASURES TO IMPROVE OUTCOMES
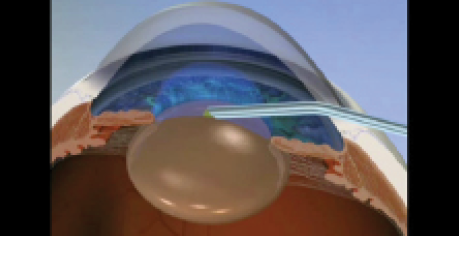
Technique. I use a soft-shell technique in cases in which I am particularly concerned about endothelial protection (http://eyetube.net/?v=pifos). Before creating the capsulorrhexis, I place a small amount of a dispersive ophthalmic viscosurgical device (OVD) such as Viscoat (Alcon) in the anterior chamber. Next, I place a larger amount of cohesive OVD such as Healon (Abbott Medical Optics) or Provisc (Alcon) under the dispersive OVD and watch the dispersive OVD spread upward over the endothelium. If necessary, this maneuver can be repeated before starting phacoemulsification and/or before inserting the IOL.
Care must be taken not to overfill the anterior chamber with a dispersive OVD before phacoemulsification, as this type of viscoelastic material can block the phaco probe and cause wound burn. If necessary, I aspirate some OVD before commencing phacoemulsification. At the end of the case, I ensure that all of the OVD is aspirated due to the risk of a postoperative IOP spike.
I do not use a soft-shell technique in all cases because of the threat of a spike in pressure with dispersive OVDs. I may preemptively treat with oral acetazolamide if IOP rise is a concern, but I do not feel that this is necessary for all patients.
Fuchs endothelial dystrophy. This common corneal dystrophy is characterized by central corneal guttata. Anticipating the likelihood of significant corneal decompensation postoperatively is challenging, even for corneal specialists. For patients in whom there are significant confluent central guttata, it is prudent to seek a corneal specialist’s opinion, as many of us now choose to combine phacoemulsification with a selective endothelial transplantation procedure such as Descemet-stripping automated endothelial keratoplasty, Descemet-stripping endothelial keratoplasty, or Descemet membrane endothelial keratoplasty. I assess the cataract and guttata to determine which is responsible for patients’ symptoms. In most cases, both are. The combined technique preempts an occurrence of PBK. Surgical outcomes of endothelial keratoplasty are significantly better with Fuchs dystrophy than they are with PBK; therefore, surgeons must not wait for or cause PBK because permanent corneal scarring and haze can ensue.
Even more common than confluent central guttata is the appearance of early Fuchs dystrophy with a few guttata. They are unlikely to be visually significant, and in such cases it is safe to proceed carefully with phacoemulsification using a soft-shell technique.
Shallow anterior chamber. A hyperviscous OVD such as Healon GV (Abbott Medical Optics) allows as much deepening of the anterior chamber as possible. Chopping the nucleus is helpful to reduce phaco energy. I use a soft-shell technique to protect the endothelium in eyes with a dense nucleus or previous surgery (especially previous corneal transplant surgery) and in any case in which greater surgical complexity and manipulation are expected, such as with weak zonules or small pupils.
At a Glance
- A soft-shell technique is particularly useful in cases in which one is concerned about endothelial protection.
- The endothelial cell layer responds more favorably to surgically induced injury when the inflammatory system is preemptively downregulated.
Watch it Now
In the soft-shell technique, a small amount of dispersive OVD is placed in the anterior chamber, followed by a larger amount of cohesive OVD placed underneath the dispersive. This causes the dispersive OVD to spread upward over the endothelium.
IMPROVING VISION ON the first POSTOPERATIVE DAY
Donnenfeld et al evaluated the effect of preoperative topical steroid pulsing on endothelial protection.1 The endothelial cell layer is neuroectoderm-derived and, like all neurological tissue, responds more favorably to surgically induced injury when the inflammatory system is preemptively downregulated. According to the study authors, difluprednate (Durezol; Alcon) reduced inflammation more effectively than prednisolone acetate, resulting in more rapid return of vision postoperatively. Because difluprednate is not available in the United Kingdom, my patients receive four doses of dexamethasone 0.1% 1 hour before surgery.
CONCLUSION
We continually strive to raise the bar for what can be achieved with modern cataract surgery. To ensure that patients not only achieve rapid visual recovery but also enjoy long-term excellent vision, it is essential that we properly respect and protect the endothelial cell layer during surgery. n
1. Donnenfeld ED, Holland EJ, Solomon KD, et al. A multicenter randomized controlled fellow eye trial of pulse-dosed difluprednate 0.05% versus prednisolone acetate 1% in cataract surgery. Am J Ophthalmol. 2011;152(4):609-617.
Allon Barsam, MD, MA, FRCOphth
- Consultant Ophthalmic Surgeon, Luton & Dunstable University, The Western Eye Hospital, Imperial College Healthcare NHS Trust, London
- Consultant Ophthalmic Surgeon, Focus Clinics, London
- eyes@allonbarsam.com
- Financial disclosure: None
