


Dry eye disease (DED) is a common ocular condition with a complex and multifactorial etiology, resulting in inconsistency and discordance between clinical signs and symptoms in a percentage of patients.1,2 Therapeutic options for severe DED are limited, and the clinical development of new treatments has been hindered, at least in part, by a lack of standardized diagnostic criteria for determining disease severity.3-5
In all existing DED classification systems, including guidelines published by the Dry Eye WorkShop (DEWS),6 the presence of severe signs and symptoms is prerequisite for the diagnosis of severe DED. However, such classification may be unsuitable for patients with discordant signs and symptomatology, highlighting the need for a more individualized, patient-tailored diagnostic approach to DED.
To this end, the multinational Ocular Dryness Disease Severity (ODISSEY) European Consensus Group has published recommendations for a practical two-step algorithm to evaluate disease severity in DED.7
A panel of 10 ophthalmologists, including one American, met in September 2012 with the aims of reviewing clinical and scientific challenges in the diagnosis and management of severe DED and developing a simplified approach to severe DED evaluation. The panel appraised a total of 14 criteria commonly used to assess DED severity. These included corneal fluorescein staining (CFS), tear hyperosmolarity, Schirmer testing, impression cytology, filamentary keratitis, conjunctival staining, impaired visual function, meibomian gland disease or eyelid inflammation, blepharospasm, tear breakup time (TBUT), aberrometry, in vivo corneal confocal microscopy, inflammatory biomarkers (ie, human leukocyte antigen-DR [HLA-DR], matrix metalloproteinase 9 [MMP-9], cytokines, tear proteomics), and patient refractory to standard disease treatments.
EVALUATING DED SEVERITY IN TWO STEPS
The ODISSEY panel agreed on a two-step scoring system for DED diagnosis that is specifically designed to address the discordance between signs and symptomatic evaluation (Figure 1). In all cases, a diagnosis of DED must be first confirmed with TBUT before the algorithm is applied.
Step No. 1: Establish fundamental criteria. In the first step, disease severity is established through patient-reported assessment of symptoms via the Ocular Surface Disease Index (OSDI) questionnaire8 and signs of ocular surface damage as assessed by CFS. The OSDI is a widely used, well-validated questionnaire that correlates moderately well with disease severity. An OSDI score of 30 or more generally indicates severe DED. In terms of assessment of DED signs, CFS is considered a reproducible, reliable, and inexpensive test that can be used to evaluate cornea health.
At a Glance
• The ODISSEY panel agreed on a two-step scoring system for DED diagnosis that is specifically designed to address the discordance between signs and symptomatic evaluation.
• According to the scoring system, a diagnosis of severe DED can be made if the OSDI score is 33 or greater and the CFS score is 3 or less on the Oxford scheme.
• In case of discordance between DED signs and symptoms, consideration of determinant or contributory diagnostic criteria is recommended in order to improve diagnostic specificity.
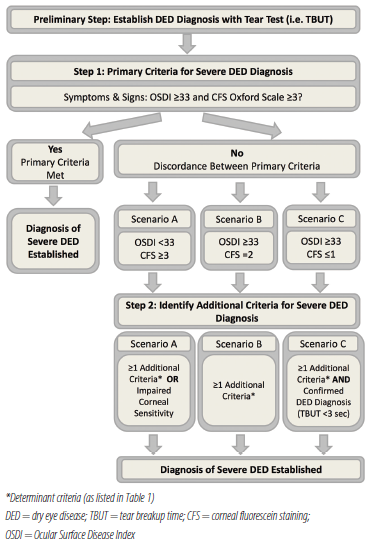
Figure 1. Consensus-derived scoring algorithm for severe DED diagnosis.
The panel determined that, for most patients with good correlation between signs and symptoms, the combination of OSDI and CFS is sufficient as a frontline assessment to establish DED severity. Thus, if the OSDI score is 33 or greater and the CFS score is 3 or less on the Oxford scheme, a diagnosis of severe DED can be made.
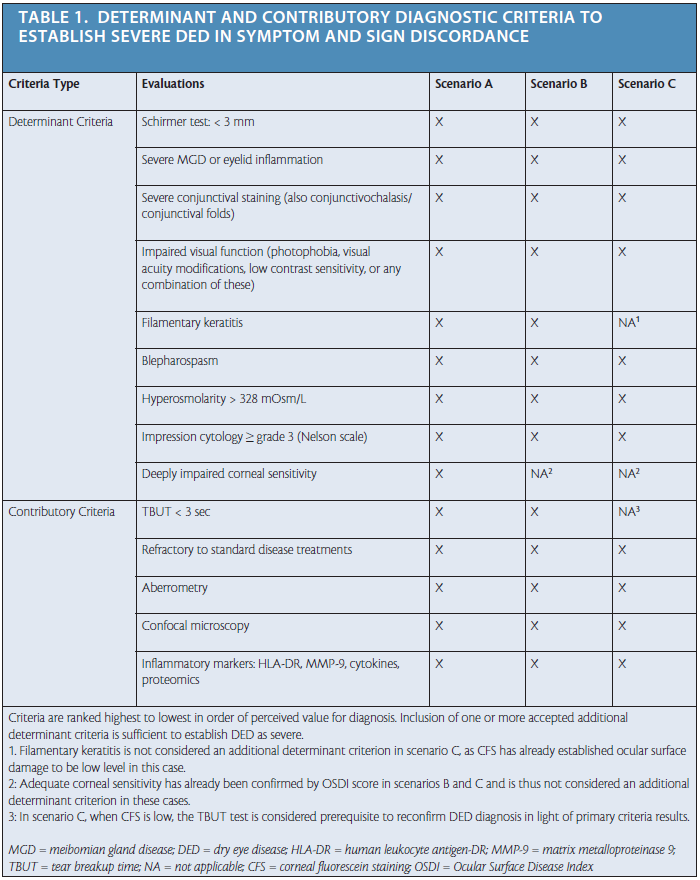
Step No. 2: Consider additional criteria. In case of discordance between DED signs and symptoms, consideration of additional diagnostic criteria is recommended in order to improve diagnostic specificity. Additional criteria were classified as either determinant or contributory and then ranked in order of perceived diagnostic value (Table 1). Determinant criteria (eg, Schirmer testing, conjunctival staining, hyperosmolarity) are well-established, validated diagnostic tests for DED severity. Contributory criteria (eg, aberrometry, inflammatory markers, confocal microscopy) may be indicative of disease severity, but generally these tests are not yet well established or routinely measured in the clinic. For further information on the advantages and disadvantages of each criterion, as discussed by the ODISSEY panel, see the full published article in the British Journal of Ophthalmology.7
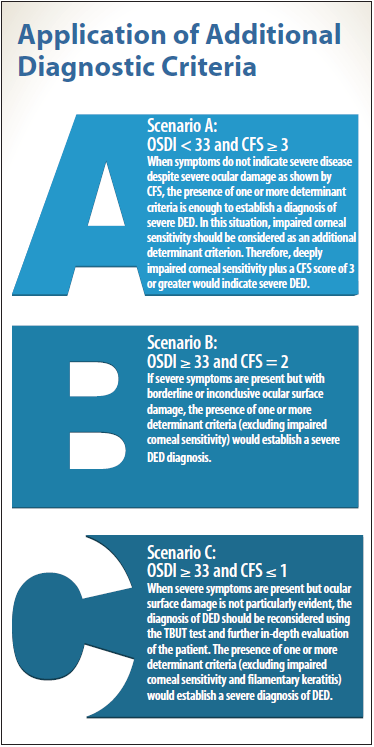
Following the algorithm, the additional diagnostic criteria are applied in Step 2 according to three possible scenarios of sign and symptom discordance observed in Step 1 (Table 1 and Application of Additional Diagnostic Criteria). In all three scenarios outlined, the presence of just one determinant criterion in addition to either OSDI of 33 or greater or CFS of 3 or greater is accepted for diagnosis of severe DED. In scenarios B and C, corneal sensitivity is not considered as a determinant criterion, as adequate corneal sensitivity will have already been demonstrated by the OSDI score in Step 1. Likewise, filamentary keratitis is not considered as an additional determinant criterion in scenario C, as low ocular surface damage will have already been established with CFS.
The ODISSEY panel has acknowledged several limitations to the use of the published algorithm, noting that development of the model was based on consensus agreement and therefore was not purely evidence-based. Additionally, the current lack of DED biomarkers with well-established criteria precludes any standardization of DED severity, and use of some of the recommended diagnostic evaluations will depend on test availability, cost, and adequate user training.
CONCLUSION
The scoring algorithm proposed by the ODISSEY group is an easy-to-use tool for the evaluation and diagnosis of severe DED. It is hoped that future validation and use of the algorithm in clinical trials will facilitate the development of new treatments for severe DED. Conceivably, once validated, the algorithm may be used for assessment of disease progression and to improve clinical decision-making in everyday ophthalmology practice. n
1. Sullivan BD, Crews LA, Messmer EM, et al. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: clinical implications. Acta Ophthalmol. 2014;92(2):161-166.
2. Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):762-770.
3. Foulks GN. Challenges and pitfalls in clinical trials of treatments for dry eye. Ocul Surf. 2003;1(1):20-30.
4. Savini G, Prabhawasat P, Kojima T, Grueterich M, Espana E, Goto E. The challenge of dry eye diagnosis. Clin Ophthalmol. 2008;2(1):31-55.
5. Sullivan BD, Whitmer D, Nichols KK, et al. An objective approach to dry eye disease severity. Invest Ophthalmol Vis Sci. 2010;51(12):6125-6130.
6. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):75-92.
7. Baudouin C, Aragona P, Van Setten G, et al. Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168-1176.
8. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118(5):615-621.
Christophe Baudouin, MD, PhD, FARVO
• Professor and Chair, Department of Ophthalmology, Quinze-Vingts National Ophthalmology Hospital, Paris
• cbaudouin@15-20.fr
• Financial disclosure: Paid consultant (Alcon, Allergan, Santen, Thea), Scientific Advisor (TearLab)
Gerd Geerling, MD, PhD, FEBO
• Professor and Chair, Department of Ophthalmology, Heinrich-Heine-Universität, Düsseldorf, Germany
• geerling@med.uni-duesseldorf.de
• Financial disclosure: Paid consultant (Santen, TearScience, Allergan, Thea, Bausch + Lomb), Owner of or shareholder in company (TearLab)
ODISSEY European Consensus Group: Christophe Baudouin, Pasquale Aragona, Gysbert Van Setten, Maurizio Rolando, Murat Irkeç, José Benítez del Castillo, Gerd Geerling, Marc Labetoulle, Stefano Bonini
