


A complaint of irritated eyes can often be perplexing. A number of technological advances are available to help differentiate among the numerous etiologies of ocular irritation. Many practices also have technicians taking preliminary histories to improve office efficiency. That said, is the use of communication to decipher the etiology of a patient’s irritated eyes a lost art?
Technological advances help us better care for our patients, but only when used in the proper context. We still must hear our patients’ complaints and utilize that information to help narrow the differential diagnoses and improve outcomes. In this article, we discuss the two conditions that cause ocular discomfort that are most commonly encountered in clinical practice: allergy and dry eye disease (DED).
MIXED BAG OF SYMPTOMS
The difficulty with complaints of ocular discomfort is that many anterior segment conditions have overlapping signs and symptoms. We have seen the subjective responses that people give based on varying presentations: Some may have severe symptoms with mild clinical signs of DED while others have significant clinical signs of DED with few symptoms.1
Part of these differences may be due to the fact that a suspected slow denervation may be occurring on the ocular surface, causing it to be less responsive to insult (Figure 1). Looked at from a different perspective, patients with the least amount of ocular surface signs consistent with DED are those who have the most heightened ocular surface sensitivity because they have likely had the condition for the least amount of time. Thus, even the slightest compromise in the quality of their tear film may trigger significant symptoms.2,3
The variability in the severity of ocular surface conditions, plus the challenge of differentiating between allergy and DED, can potentially create a confusing clinical situation. Can the patient’s presenting symptoms help differentiate between allergy and DED? We believe so.
REVIEW OF SYSTEMS AND MEDICATIONS
During office visits with patients, we often accumulate a significant amount of information that can lead us down certain paths in helping explain the etiology of their symptoms. Patients who have seasonal allergies are often aware that they have these allergies, unless they are presenting to you for the first time with these symptoms. In that instance, you have to deduce that the symptoms arose as a result of an allergen challenge.
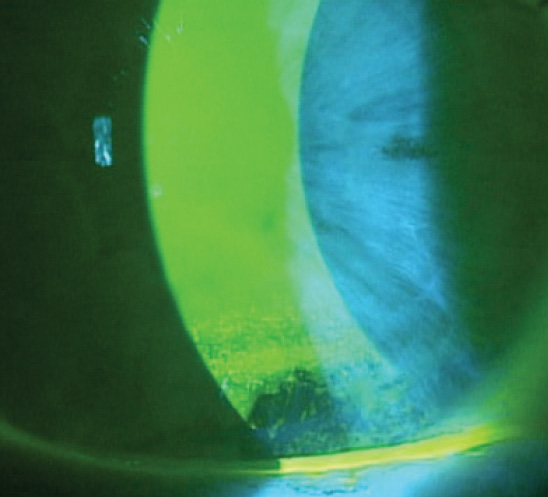
Figure 1. Significant inferior corneal staining in an asymptomatic DED patient.
Certain questions can yield crucial information: Has the patient recently acquired new pets, moved (home, office, school, etc), had a sudden onset of symptoms after performing a certain task (ie, ocular symptoms after working with certain plants)? Knowing that a patient had a sudden onset of symptoms after working with a specific substance can help lead us to consider ocular allergies as the likely etiology. On the other hand, DED is typically a slow, progressive condition.
It is also crucial to take a full patient history, as a number of contributing systemic factors can be involved in the manifesting ocular symptoms. Autoimmune conditions are those most commonly associated with dry eye.4 Although we may think of Sjögren syndrome as being the primary systemic ailment leading to DED, autoimmunity often involves multiple organ systems because of the cross-reaction of autoantibodies to various tissues in the body.5 It is not uncommon, therefore, for a patient with rheumatoid arthritis to have other systemic symptoms in addition to decreased tear production.
Certain populations, notably postmenopausal women, have an increased risk of developing DED. Other populations at greater risk for DED include older adults, computer users, and contact lens wearers.4 Pay particular attention to the medications that your patients are using, as they may be exacerbating symptoms. Common medications that can cause ocular surface drying include antihypertensives, antiarrhythmics, antidepressants, diuretics, antihistamines, and anticholingeric medications.6
Although oral antihistamines can help alleviate systemic allergic symptoms, their antimuscarinic activity has a tendency to decrease tear production and either elicit or exacerbate underlying DED.7 A less robust tear film also creates a higher concentration of antigens in the tear film, and this can potentially exacerbate an allergic conjunctivitis response. This may further complicate the differential diagnosis, in that patients may experience concurrent allergy and DED.
WHAT WILL PATIENTS TELL YOU?
Allergy. The complaint of an itchy eye is typically associated with allergic conjunctivitis. But more thorough questioning of how the eye itches will save you time and improve your diagnostic and therapeutic efforts.
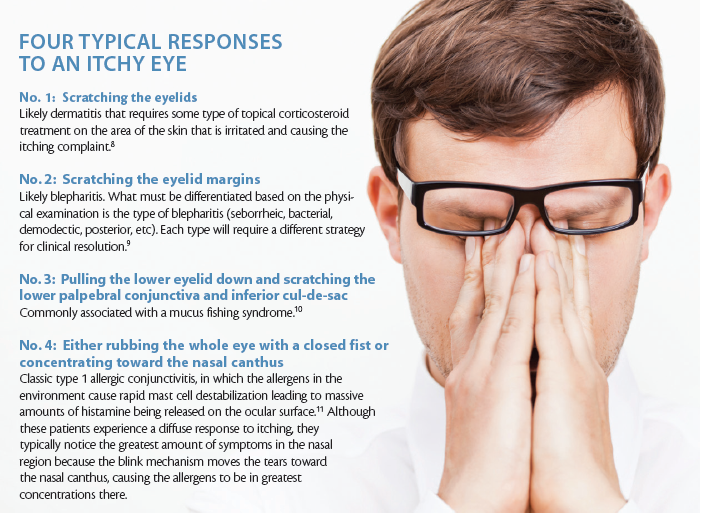
Consider having patients demonstrate how they scratch or rub their itchy eyes. We have found that people typically demonstrate four types of behavior in response to the itch (see Four Typical Responses to an Itchy Eye).8-11
DED. We often think of DED as causing a burning feeling. For some, this is the case.12 However, patients with DED can present with a variety of symptoms because the corneal subbasal nerves show significant changes compared with those in patients who do not have DED, including lower density and increased tortuosity.2 This is one of the reasons that we at times see patients whose ocular surfaces appear pristine with no visible signs of DED but who complain of significant eye dryness. This is also the reason that some corneas can have significant ocular signs with little to no symptoms reported by the patient. Which symptoms should lead us to start thinking about DED? The symptoms will vary, but the ones that patients often report are found in Common Complaints Associated With DED.
COMMON COMPLAINTS ASSOCIATED WITH DED
• My eyes feel like they are burning.
• My eyes are uncomfortable or feel like they are stinging.
• My eyes feel irritated.
• It feels like something is in my eyes.
• My vision fluctuates.
• My vision seems to get worse the longer I am reading or using a computer.
• My vision does not seem as good later in the day.
Listen to what your patients say, and pay attention to what they do as they are being tested. If your technician tells you that the patient had to blink frequently during pretesting or the patient commented on how difficult it was to keep his or her eyes open during testing, this may be an indication of DED. Additionally, if you note visual instability during the refraction, this should heighten your suspicion of DED.
At a Glance
• Although technological advances are an important component in DED diagnosis when used in the proper context, physicians must hear a patient’s complaints and utilize that information to help narrow the differential diagnosis and improve outcomes.
• Patients with the least amount of ocular surface signs consistent with DED are those who have the most heightened ocular surface sensitivity because they have likely had the condition for the least amount of time.
• The four typical responses to a scratchy eye—scratching the eyelids, scratching the eyelid margins, pulling the lower eyelid down and scratching the lower palpebral conjunctiva and inferior cul-de-sac, and either rubbing the whole eye or concentrating toward the nasal canthus— can help to reveal the etiology of the problem and illuminate an appropriate treatment course.
• As a final check of the symptoms and clinical findings, consider the following: Place an artificial tear in one eye and a topical antiallergy medication in the other and wait several minutes. If the eye with the topical antiallergy medication feels better, it is likely an allergic condition. If both drops make the eyes feel equally comfortable or the artificial tear makes that eye feel slightly more comfortable, it is likely DED.
ONE MORE TEST
Despite the investigations and questions suggested above, a patient’s symptoms and signs may at times leave us unable to differentiate an etiology. In these instances—or if you would simply like one additional piece of information to solidify your diagnosis—we recommend the following: If both eyes are experiencing symptoms, place an artificial tear in one eye and a topical antiallergy medication in the other. Then wait several minutes to see if one drop or the other improves the patient’s symptoms.
If the eye with the topical antiallergy medication feels better than the eye receiving the artificial tear, it is likely an allergic condition. If both drops make the eyes feel equally comfortable or the artificial tear makes that eye feel slightly more comfortable, it is likely DED. Although this is a basic test, it works remarkably well as a final check of symptoms and clinical findings to confirm the reason for the underlying irritation.
FINAL THOUGHTS
Patients’ symptoms often present a confounding number of factors to consider when we begin to establish a differential diagnosis. By taking a thorough history of systemic conditions, noting the medications that the patient is taking, and also digging deeper into the ocular symptoms they describe, you are likely to arrive at an accurate diagnosis and sort successfully through the plethora of symptoms that often seem to overlap in our allergy and dry eye patients. n
1. Tran N, Graham AD, Lin MC. Ethnic differences in dry eye symptoms: effects of corneal staining and length of contact lens wear. Cont Lens Anterior Eye. 2013;36(6):281-288.
2. Labbé A, Liang Q, Wang Z, et al. Corneal nerve structure and function in patients with non-Sjogren dry eye: clinical correlations. Invest Ophthalmol Vis Sci. 2013;54(8):5144-5150.
3. Mantelli F, Massaro-Giordano M, Macchi I, et al. The cellular mechanisms of dry eye: from pathogenesis to treatment. J Cell Physiol. 2013;228(12):2253-2256.
4. Granet D. Allergic rhinoconjunctivitis and differential diagnosis of the red eye. Allergy Asthma Proc. 2008;29(6):565-574.
5. Shulman S. Tissue specificity and autoimmunity. Mol Biol Biochem Biophys. 1974;0(16):1-196.
6. Fraunfelder FT, Sciubba JJ, Mathers WD. The role of medications in causing dry eye. J Ophthalmol. 2012;2012;285851.
7. Bielory L. Ocular toxicity of systemic asthma and allergy treatments. Curr Allergy Asthma Rep. 2006;6(4):299-305.
8. Alexander KL. Some inflammations of the external eye and adnexa. J Am Optom Assoc. 1980;51(2):142-147.
9. Pflugfelder SC, Karpecki PM, Perez VL. Treatment of blepharitis: recent clinical trials. Ocul Surf. 2014;12(4):273-284.
10. McCulley JP, Moore MB, Matoba AY. Mucus fishing syndrome. Ophthalmology. 1985;92(9):1262-1265.
11. Miraldi Utz V, Kaufman AR. Allergic eye disease. Pediatr Clin North Am. 2014;61(3):607-620.
12. Messmer EM. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int. 2015;112(5):71-82.
Mile Brujic, OD, FAAO
• Partner, Premier Vision Group, Bowling Green, Ohio
• brujic@prodigy.net
• Financial disclosure: Honoraria (Alcon, Allergan, Bausch + Lomb, Paragon, SpecialEyes, Valley Contax)
David L. Kading, OD, FAAO
• Partner, Specialty Eye Group, Kirkland, Washington
• dave@optometricinsights.com
• Financial disclosure: Honoraria (Alcon, Allergan, Art Optical, Bausch + Lomb, Contamac, CooperVision, Ciba Vision, Medlens Innovations, Paragon, SynergEyes, Unilens, Valley Contax, Vistakon, The Vision Care Institute)
