

Posterior polar cataract is a dense, round opacity in the center of the posterior lens capsule that is associated with congenital defects (Figure 1).1 As the capsule is extremely fragile, removing this type of cataract without a proper strategy can lead to the rupture of the posterior capsule intraoperatively.
Several surgical approaches have been suggested depending on the character of the posterior polar cataract, including anterior and posterior approaches and intracapsular cataract extraction.2 The anterior approach is preferred in many cases because trauma is minimized when the surgery can be performed without complications. However, if the lens nucleus must be divided in order to be removed, the surgical difficulty increases significantly. Reflecting this reality, high rates of posterior capsular rupture during surgery have been reported in previous studies.3,4
I recently developed a technique that I call pre-surround division. This procedure is intended to reduce surgical difficulty by dividing the nucleus into three pieces without rotating the lens.5,6 Making precise cracks before phacoemulsification helps to avoid the occurrence of accidental cracks over the polar opacity. I believe this technique is an easy and safe surgical strategy for use in posterior polar cataracts that require nucleus division (see Steps in the Pre-Surround Division Technique).
WHY PRE-SURROUND DIVISION?
In managing patients with uveitis, I have encountered many challenging surgical cases of secondary cataract caused by intraocular inflammation. In these patients, I have used not only standard techniques,7-9 but also techniques I developed myself,10,11 to address the features of these cataracts. Over time, I came to recognize that the prechopper instrument is the best device to make precise cracks during lens division.
There are several crucial points for successful posterior polar cataract surgery; however, few dividing strategies meant specifically for this indication have been elaborated in the literature. If hydrodelineation is performed imperfectly, standard dividing techniques may create cracks over the polar opacity, leading to posterior capsular rupture. Additionally, it can be difficult for inexperienced surgeons to make accurate cracks without unintentional downward pressure on the posterior capsule.
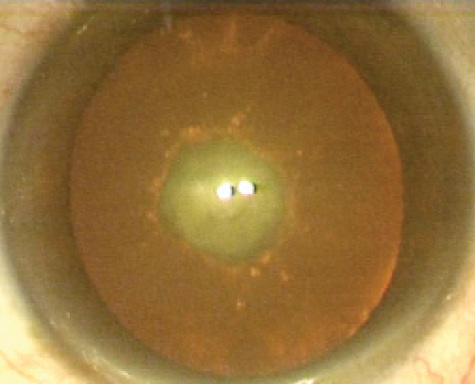
Figure 1. Posterior polar cataract: Dense polar opacity is seen in the center of the posterior capsule.
Through my experience with posterior polar cataract surgery, I recognized that one of the most important points in surgery is dividing the lens without creating cracks over the polar opacity. Making accurate cracks during phacoemulsification is difficult, even for experienced surgeons. By contrast, making precise cracks before phacoemulsification is easy, even for inexperienced surgeons.
Therefore, in the pre-surround division technique, cracks are created surrounding the polar opacity using a prechopper before phacoemulsification. This approach is easy and safe, whether hydrodelineation has been successful or not. Dividing the lens into three pieces without rotation before phacoemulsification also helps to avoid surgical complications.
At a Glance
• With a posterior polar cataract, if the lens nucleus
must be divided in order to be removed, the surgical
difficulty increases significantly.
• One of the most important points in surgery is
dividing the lens without creating cracks over the polar
opacity; in the pre-surround division technique, cracks
are created surrounding the polar opacity using a
prechopper before phacoemulsification.
• Correctly managing the prechopper blade is the key to
successful lens division.
Steps in the Pre-surround Division Technique
1. Vasavada AR, Raj SM. Inside-out delineation. J Cataract Refract Surg. 2004;30:1167-1169.
Figure 1. Hydrodelineation is performed. The golden ring is seen.
Figure 2. Division with the prechopper is performed on the left side of the lens. The polar opacity is avoided.
Figure 3. Division is performed on the right side of the lens. Cracks surrounding the polar opacity are created.
Figure 4. A hook is used as a second instrument throughout phacoemulsification to avoid accidental movement of the lens.
Figure 5. OVD is injected to separate the cortex and the polar opacity from
the posterior capsule.
Crucial Points for Successful Posterior Polar Cataract Surgery
Perform complete hydrodelineation.
Avoid lens rotation.
Divide the lens without creating cracks over the posterior polar opacity.
PEARLS FOR PRE-SURROUND DIVISION
Correctly managing the prechopper blade is the key to successful lens division. Careless movement of the blade will stress the fragile capsule. Important points to remember in movement of the prechopper blade include inserting it into the lens slowly and moving slowly away from the center with proper force.
The prechopper can be used in mild or moderately dense nuclei in most cases, but it is difficult to insert the prechopper blade into a dense nucleus without exerting pressure on the capsule. Therefore, in these eyes, other methods such as intracapsular cataract extraction should be considered.
SUMMARY
It may not be difficult for the surgeon to divide a posterior polar cataract lens with conventional techniques when hydrodelineation is performed perfectly. However, if one is concerned about performing perfect hydrodelineation and avoiding unintentional downward pressure and unintentional cracks over the posterior polar opacity, the pre-surround division technique is an easy, safe alternative strategy. n
1. Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16:157-162.
2. Vasavada AR, Raj SM, Vasavada V, Shrivastav S. Surgical approaches to posterior polar cataract: a review. Eye. 2012;26:761-770.
3. Hayashi K, Hayashi H, Nakao F, Hayashi F. Outcomes of surgery for posterior polar cataract. J Cataract Refract Surg. 2003;29:45-49.
4. Vasavada A, Singh R. Phacoemulsification in eyes with posterior polar cataract. J Cataract Refract Surg. 1999;25:238-245.
5. Kamoi K, Mochizuki M. Pre-surround division technique. J Cataract Refract Surg. 2014;40:1764-1767.
6. Kamoi K. Pre-surround division technique devised for posterior polar cataract surgery. Ocular Surgery News. February 25, 2015.
7. Gimbel HV. Divide and conquer nucleofractis phacoemulsification: development and variations. J Cataract Refract Surg. 1991;17:281-291.
8. Fine IH. The chip and flip phacoemulsification technique. J Cataract Refract Surg. 1991;17:366-371.
9. Akahoshi T. Phaco prechop: manual nucleofracture prior to phacoemulsification. In: Operative Techniques in Cataract and Refractive Surgery. Philadelphia: WB Saunders; 1998:69-91.
10. Kamoi K, Mochizuki M. Phaco forward-chop technique for managing posterior nuclear plate of hard cataract. J Cataract Refract Surg. 2010;36:9-12.
11. Kamoi K, Mochizuki M. Phaco dislocation technique in young patients with uveitis. J Cataract Refract Surg. 2008;34:1239-1241.
12. Vasavada AR, Raj SM. Inside-out delineation. J Cataract Refract Surg. 2004;30:1167-1169.
Koju Kamoi, MD, PhD
• Junior Associate Professor, Department of Ophthalmology and
Visual Science, Tokyo Medical and Dental University
• koju.oph@tmd.ac.jp
• Financial disclosure: None
