


Dry eye disease (DED) is one of the most frequent pathologies in ophthalmology, affecting 10% to 25% of the general population.1-3 Its symptomatology can negatively affect quality of life and produce significant impacts on social costs in terms of well-being and job performance. After cataract surgery, DED-like symptoms can occur in any patient and can potentially worsen in those who had experienced symptoms preoperatively.
The Report of the Dry Eye WorkShop (DEWS)4 defined DED as a multifactorial disease of the tears and ocular surface characterized by three main symptoms: ocular discomfort, visual disturbance, and tear film instability, with the potential to damage the ocular surface.
Recently, a growing number of publications have reported a high incidence of DED-like symptoms in patients who have undergone cataract surgery. In 2010, our group concluded that cataract surgery may induce signs and symptoms similar to dry eye and that an unstable tear film can still be present 60 days postoperatively.5 For these reasons, and because cataract surgery is now the most common surgical procedure performed in ophthalmic units—meaning the real incidence of dry eye is increasing every day—one should always assess the possible risk for DED in patients with previous ocular surface disease and consider treatment with tear substitutes prior to surgery in these patients.
The purpose of this article is to report the incidence of DED following cataract surgery and to review its treatment and prevention, particularly in high-risk patients.
RETROSPECTIVE ANALYSIS
From 2012 to 2014, we performed 3,200 phacoemulsification procedures at three surgery centers. Our retrospective analysis indicated that the median age of patients was 73 years (range, 48–96 years), that 69% of patients were women, and that preoperative BCVA was 0.4 (range, light perception to 0.8). In total, 70% of patients presented with some combination of the following: treated systemic hypertension, hypercholesterolemia, prostatic hypertrophy, diabetes, blepharitis, and mild dry eye; furthermore, about 10% were being treated for dry and/or wet age-related macular degeneration.
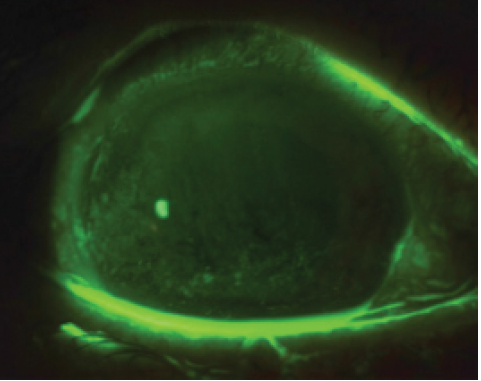
Figure 1. Positive fluorescein staining on postoperative day 1.
Surgery was performed under topical anesthesia (0.4% oxybuprocaine HCl). A 2.2-mm temporal clear corneal incision was created, and a 1-mm sideport incision was made approximately 60º away from the main incision. Phacoemulsification was performed in a median operating time of 9 minutes (range, 6–16 minutes) and with a median ultrasound time of 40 seconds (range, 5–118 seconds); standard postoperative treatment included topical steroids and antibiotics four times daily, NSAIDs twice daily, and artificial tears four times daily.
At a Glance
• A growing number of publications have reported a high incidence of DED-like symptoms in patients who have undergone cataract surgery.
• Similar to many previous studies of DED following surgery, the authors’ current analysis reported a high incidence and severity of dry eye symptoms over a 90-day period after phacoemulsification.
Data from 3,200 eyes of 2,200 patients were analyzed postoperatively. BCVA was 0.8 (range, 0.1–1). No severe complications were reported, but about 3% of patients developed cystoid macular edema that resolved with prompt treatment.
Approximately 85% of patients experienced DED-like symptoms, particularly foreign body sensation, on day 1. The percentage decreased to 25% by day 30, but 15% of patients continued to complain of dry eye symptoms at day 90. Of those with continued complaints, most had blepharitis and dry eye before surgery.

Topical treatment with antibiotics, steroids, and NSAIDs was generally terminated 15 to 30 days after surgery, and use of artificial tears was continued for the following 2 months. Patients whose symptoms of DED were unresponsive to initial treatment were prescribed topical loteprednol etabonate (Lotemax; Bausch + Lomb) and artificial tears for 4 months, with nearly all patients achieving a complete recovery after this time. The standard regimen for loteprednol etabonate was a tapering dose from four times daily to once daily.
Fluorescein staining (National Eye Institute scale) was positive in 12% of patients preoperatively and in 90% on day 1 (Figure 1), 30% on day 30, and 8% on day 90 postoperative. Lissamine green staining (Van Bijsterveld scale) was positive in 5% of patients preoperatively and in 40% on day 1, 4% on day 30, and about 1% on day 90 postoperative. Schirmer testing was not performed.
Preoperative median noninvasive tear breakup time was 8 seconds (range, 2–14 seconds), decreasing to a median of 4 seconds on day 1 (range, 1–7 seconds), then improving to 7 seconds on day 30 (range, 2–11 seconds) and 9 seconds on day 90 postoperative (range, 2–16 seconds).
CONCLUSION
DED develops often after various types of ophthalmic surgeries such as refractive surgery, cataract surgery, corneal transplantation, and 20-gauge vitrectomy. Similar to many previous studies of DED following surgery, our current analysis documented a high incidence and severity of dry eye symptoms over a 90-day period after phacoemulsification.
Systemic medications and pathologies can negatively affect lacrimal gland function and tear film distribution, particularly after cataract surgery; furthermore, the presence of diabetes frequently worsens or induces blepharitis and results in evaporative DED. Patients with these conditions must be strictly monitored before and after cataract surgery, and they often require treatment for longer than the standard postoperative regimen. n
1. van Landingham SW, West, SK, Akpek EK, et al. Impact of dry eye on reading in a population-based sample of the elderly: the Salisbury Eye Evaluation. Br J Ophthalmol. 2014;98(5):639-644.
2. McCarty CA, Bansal AK, Livingston PM, et al. The epidemiology of dry eye in Melbourne, Australia. Ophthalmology. 1998;105(6):1114-1149.
3. Schaumberg DA, Sullivan DA, Dana MR. Epidemiology of dry eye syndrome. Adv Exp Biol Med. 2002;506(Pt B):989-998.
4. [No authors listed] The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):75-92.
5. Barabino S. Dry eye-like symptoms and signs after cataract surgery. Poster presented at: Association for Research in Vision and Ophthalmology Annual Meeting; May 2-6, 2010; Fort Lauderdale, Florida.
Federico Solignani, MD
• Centro Medico DueSoli La Spezia, Italy
• Casa di Cura Barbantini, Lucca, Italy
• Ospedale di Desio, Desio, Italy
• federico.solignani@gmail.com
• Financial disclosure: None
Giancarlo Solignani, MD
• Centro Medico DueSoli La Spezia, Italy
• Casa di Cura Barbantini, Lucca, Italy
• Financial disclosure: None
