

Residual astigmatism after cataract surgery can serve as a major impediment to achieving a patient's refractive target. But, because not all astigmatism is equal, patients are best served by the availability of a wide range of options for astigmatism correction.
In my view, cylinder starting at 0.50 to 0.75 D must be addressed in order to give patients the best chance of achieving spectacle independence or reaching their refractive target, whatever that may be. There are several options for addressing astigmatism at the time of cataract surgery, ranging from manual corneal incisions to toric IOL implantation. For surgeons who use femtosecond lasers, there is the additional option of intrastromal astigmatic keratotomy (AK).
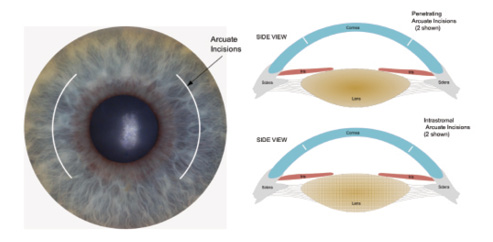
Figure 1. Illustration of AK showing penetrating (top right) and intrastromal (bottom right) incisions.
Venter et al reported that intrastromal AK is a viable option to reduce astigmatism ranging from 0.50 to 2.75 D of cylinder.1 In their study of 112 eyes with low mixed astigmatism treated with nonpenetrating femtosecond laser intrastromal AK, mean distance UCVA improved from 0.18 preoperatively to 0.02 logMAR postoperatively (P<.01), and cylinder decreased from 1.20 D preoperatively to 0.55 D postoperatively (P<.01). There was a tendency toward undercorrection, so I have slightly modified the nomogram that the authors introduced.
SELECT THE RIGHT PATIENT
Before one even thinks about surgical parameters, selecting the right patients is a key factor in the success of intrastromal AK. Because AK incisions are neutral as far as myopia or hyperopia, the best results will be attained in patients who have mixed astigmatism with a plano spherical equivalent. To address astigmatism at the time of cataract surgery, it is best to perform intrastromal AK in patients who have plano spherical equivalent and at least 0.50 to 0.75 D and above of astigmatism. Although I do not have a hard cap on the maximum amount of astigmatism to address with intrastromal AK, eyes with cylinder of 2.50 D and above may obtain more predictable effects with a penetrating AK incision and/or a toric IOL.
A toric IOL is an excellent option for patients willing to pay the extra out-of-pocket expense. I typically recommend toric IOLs for patients with about 0.75 D of astigmatism or higher; however, when I have a patient who is a toric candidate but expresses hesitance about the extra charge, I also discuss intrastromal AK as an option.
THE ART OF AK
As much as intrastromal AK is a science, there is also an art to performing these incisions (Figure 1). In their study, Venter and colleagues1 used paired symmetrical nonpenetrating intrastromal AK incisions created from 60 μm below the corneal surface to 80% depth at a 7-mm diameter. Because the authors noted some undercorrection, I use a slightly modified approach: I add 5° to the arc length to get more effect.
It is also important when making these incisions to use a high laser energy level to ensure there is a clean, powerful incision; I make the spacing of the laser pulses tight, usually around 3 µm on both the spot and layer separation. Most nomograms center around three parameters—diameter, depth, and arc length. The arc length remains the most variable of my settings, and it is adjusted according to the amount of astigmatism in the eye.
Whereas Venter et al1 suggested an 80% depth, other nomograms suggest a 90% depth. The theoretical advantage of a slightly deeper incision is that it will be more powerful; the drawback is that it may be more prone to perforation. A unique advantage of intrastromal AK incisions is that they can be more easily titrated by opening the incision, which can be performed at the slit lamp or in a minor procedure room. Opening the AK incision is most easily achieved if the anterior edge of the incision is left just under the Bowman layer.
There is one other variable in performing intrastromal AK: the surgical platform. In my practice, we use the iFS Advanced Femtosecond Laser (Abbott Medical Optics). I cannot say for certain whether one platform has advantages over others in terms of making AK incisions, but I can attest that, after using this laser for years to perform refractive procedures, I have a comfort level with the technology. Therefore, using it to perform intrastromal AK involved a minimal learning curve. n
1. Venter J, Blumenfeld R, Schallhorn S, Pelouskova M. Non-penetrating femtosecond laser intrastromal astigmatic keratotomy in patients with mixed astigmatism after previous refractive surgery. J Refract Surg. 2013;29(3):180-186.
Christopher L. Blanton, MD
• Medical Director, Inland Eye LASIK, Southern California
• blanton007@aol.com
• Financial disclosure: Advisor (Abbott Medical Optics)