


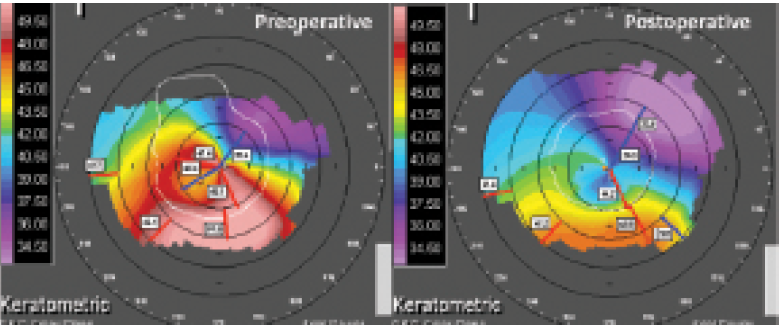
Figure 1. Clinical example of the authors’ technique of nontopographic transepithelial PRK with immediate CXL for frank keratoconus, showing greater effect than would be expected from CXL or sub–50-μm ablation alone. Corneal topography at baseline (left) and 24 months (right). BCVA improved from 0.7 to -0.08 logMAR.
ISSUES SURROUNDING PRK PLUS CXL
CONCLUSION
1. Alpins N, Stamatelatos G. Customized photoastigmatic refractive keratectomy using combined topographic and refractive data for myopia and astigmatism in eyes with forme fruste and mild keratoconus. J Cataract Refract Surg. 2007;33(4):591-602.
2. Mortensen J, Ohrström A. Excimer laser photorefractive keratectomy for treatment of keratoconus. J Refract Corneal Surg. 1994;10(3):368-372.
3. Koller T, Iseli HP, Donitzky C, Ing D, Papadopoulos N, Seiler T. Topography-guided surface ablation for forme fruste keratoconus. Ophthalmology. 2006;113(12):2198-2202.
4. Kanellopoulos AJ, Binder PS. Collagen cross-linking (CCL) with sequential topography-guided PRK: a temporizing alternative for keratoconus to penetrating keratoplasty. Cornea. 2007;26(7):891-895.
5. Alessio G, L’abbate M, Sborgia C, et al. Photorefractive keratectomy followed by cross-linking versus cross-linking alone for management of progressive keratoconus: two-year follow-up. Am J Ophthalmol. 2013;155(1):54-65.
6. Mukherjee AN, Selimis V, Aslanides I. Transepithelial photorefractive keratectomy with crosslinking for keratoconus. Open Ophthalmol J. 2013;7:63-68.
7. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg. 2009;25(9):S812-S818.
8. Kymionis GD, Grentzelos M, Kounis G, Diakonis VF, Limnopoulou AN, Panagopoulou SI. Combined transepithelial phototherapeutic keratectomy and corneal collagen cross-linking for progressive keratoconus. Ophthalmology. 2012;119(9):1777-1784.
9. Kymionis GD, Grentzelos MA, Klados NE, Xanthopoulou NA, Paraskevopoulos TA, Detorakis ET. Corneal collagen cross-linking mushroom shape demarcation line profile after limited Bowman’s membrane removal by phototherapeutic keratectomy. Open Ophthalmol J. 2015;9:17-19.
10. Stojanovic A, Zhang J, Chen X, Nitter T, Chen S, Wang Q. Topography-guided transepithelial surface ablation followed by corneal collagen cross-linking performed in a single combined procedure for the treatment of keratoconus and pellucid marginal degeneration. J Refract Surg. 2010;26(2):145-152.
Ioannis Aslanides, MD, PhD
• Medical Director, Emmetropia Mediterranean Eye Institute, Crete, Greece
• i.aslanides@emmetropia.gr
• Financial disclosure: None
Hatch Mukherjee, FRCOphth
• Consultant Ophthalmologist, Essex County Hospital, Colchester, United Kingdom
• hatch.mukherjee@gmail.com
• Financial disclosure: None
