

In my practice, I often take care of patients who have experienced difficulties relating to their IOL, because either they have become malpositioned or they have to be exchanged. Patients with subluxated or loose crystalline lenses are also often referred to me. In dealing with these cases, I use various microsurgical instruments, including iris hooks, specialized forceps, capsule hooks, and cutting instruments, and I rely on them in the most challenging surgeries, as the following case studies illustrate.
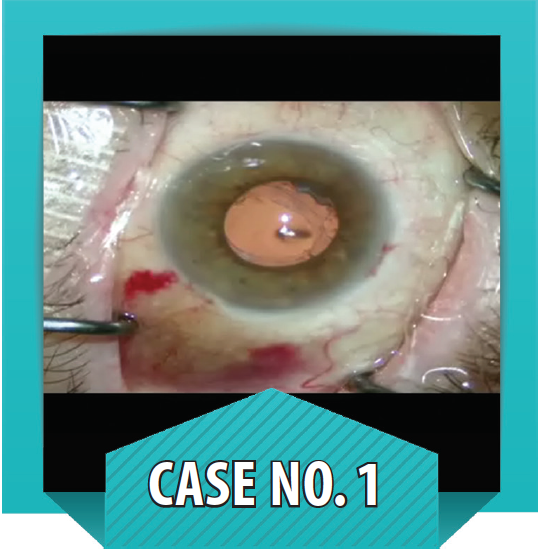
Case No. 1
Subluxated PMMA IOL and zonulopathy in a diabetic patient with keratopathy. A patient with advanced diabetes presented with a subluxated PMMA IOL with double encircling loop haptics (see figure to the left). Because this patient also had lost all vision in his fellow eye, I did not want to risk opening his one good eye widely to remove the implant through the required large incision (7–8 mm). The patient also had undergone panretinal photocoagulation and was at high risk of a suprachoroidal hemorrhage.
AT A GLANCE
• Access to microsurgical tools can help to alleviate some of the pressures associated with difficult cases.
• In the presence of a subluxated IOL, a basket safety suture can prevent the lens from falling into the posterior segment.
For these reasons, I felt that the better surgical strategy would be to salvage the IOL by suturing the haptic loops to the eye wall. This could be done through the small space at the edge of the optic at the base of the loop haptic, at the 2- and 8-o’clock positions. Because the tissue between the lens and the loop was dense and fibrotic, the trick was to pass the suture through while taking care not to let the IOL prolapse back into the vitreous.
After marking the eye for placement, I made a 350-µm groove in the peripheral cornea and created a Hoffman pocket in the sclera. I then took a fine wire needle and ran it behind the lens on each side of the eye through the pars plana, creating a basket safety suture to prevent the lens from falling into the posterior segment. I retracted the iris so I could see the haptic-optic junction through the microscope and made an opening into the Hoffman pocket with a 23-gauge trocar, allowing access to the fibrotic lens capsule material.
Once the trocar was removed, I used 25-gauge Snyder microforceps (MicroSurgical Technology) to retrieve a PTFE suture (Gore-Tex; W.L. Gore and Associates) from the opposite side of the chamber. I grabbed the end of the suture with the forceps and brought it out through the scleral pocket in order to create a lasso around the loop of the lens. This step was repeated until the two loops of the lens had been lassoed.
I then reached into the Hoffman pocket to externalize the sutures and made a slip knot in order to tension each suture equally, thereby centering and anchoring the IOL. The loose ends of the sutures were subsequently buried inside the Hoffman pocket. Finally, OVD was removed from the chamber, the basket safety suture was removed, and fibrin adhesive was added to the pockets to help them seal. Because the patient had diabetes, I also placed a bandage contact lens on the eye to protect the cornea.

Case No. 2
Placement of an artificial iris. A 50-year-old patient who had been scratched in the eye by a cat 49 years prior presented with a pronounced corneal scar with a large feeder vessel (see figure to the left). Despite having carried the blemish for so many years, the patient continued to find the disfigurement distressing and was referred to me for placement of an ArtificialIris (HumanOptics).
Because the injury happened at such an early age, the visual prognosis for this eye was not good, and I decided against offering the patient a corneal transplant at the same time as the artificial iris. My goal was to place the ArtificialIris, replace the crystalline lens with an IOL, and then, if necessary, consider addressing the corneal scar at a later date.
I began by measuring the white-to-white distance to determine the adequate size of the iris implant. The ArtificialIris is supplied with a 12.8 mm diameter but can be trimmed according to the patient’s anatomy, which, in this case, was 11.5 mm. Once I had it at the correct size, I sewed the MX60 IOL (Bausch + Lomb), a one-piece hydrophobic acrylic lens, to the back of the artificial iris using 9-0 polypropylene.
The next step was to separate the patient’s iris from the old residual lens capsule and remove some of this material using a vitrector. I went through a Hoffman pocket and used a 23-gauge trocar to make two holes, one above it and the other below it.
Before enlarging the main incision to be able to pass the iris-lens assembly through it, I reached through the pocket using the 25-gauge Snyder microforceps to bring out all four preplaced PTFE sutures. The iris-lens device was then implanted into the posterior chamber through an 8-mm incision, and the PTFE sutures were progressively tightened to stabilize and center the device. Using MicroHolder serrated forceps (MicroSurgical Technology), I removed the Soemmering ring and the degenerative lens material through the main incision in order to minimize postoperative inflammation. Finally, I performed a Siedel test to ensure that there was no leakage from the anterior chamber, restored physiologic pressure to the eye, and added fibrin adhesive to help seal the pockets and the main incision.
The surgery was successful, and, most important, the patient was happy with the result.
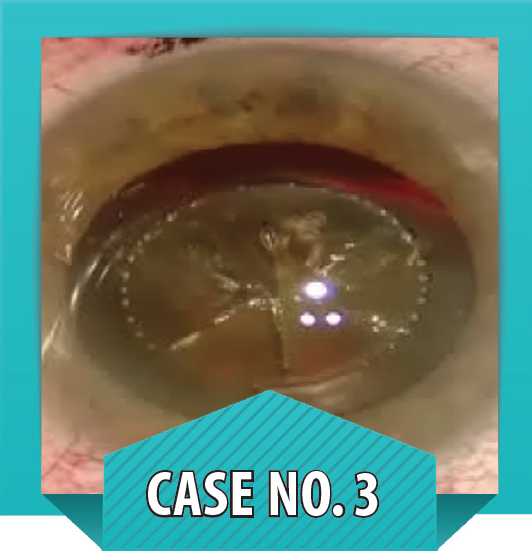
Case No. 3
Subluxated cataract caused by tennis ball injury. This patient presented with zonular disinsertion of 5 clock hours nasally after a tennis ball injury to the eye. Because the lens was loose from the zonular disinsertion, and the cataract was dense, I used the femtosecond laser to perform anterior capsulotomy and lens fragmentation (see figure to the left).
Proceeding to surgery, I used a combination of a dispersive OVD to keep the vitreous back and a cohesive OVD over the lens. I then removed the anterior capsule, which had been cut by the femtosecond laser, with Ahmed micrograspers (MicroSurgical Technology). I positioned four capsular support hooks under the capsule to hold the lens firmly in place during phacoemulsification, which was managed routinely.
The next step was cortex removal and insertion of a standard Morcher capsular tension ring. Because iris hooks can interfere with cortex removal, I tend to take them out at this point.
The capsular bag was well centered; however, because there was a large sector of zonular loss, I felt it was prudent to sew the capsular bag to the eye wall. I made a scleral groove on the nasal side, and, after making space between the iris and the capsular bag with an OVD and a microvitreoretinal blade, I inserted a Malyugin modified capsular tension ring (Morcher) into the capsular bag with a PTFE suture through the eyelet; I then reached through with forceps to bring both ends of the preloaded suture out through the scleral pocket that I had created earlier. The OVD was then removed, and, once the lens was perfectly centered, I tied the sutures and buried the ends.
A routine postoperative outcome was achieved in this difficult and risky case, thanks to the microinstrumentation and the femtosecond laser.
CONCLUSION
Complicated surgical cases, such as the three that I describe here, can require an array of microsurgical tools, from forceps to iris hooks. Access to effective, reliable microsurgical tools can help to alleviate some of the pressures associated with difficult cases.
Samuel Masket, MD
• Founding Partner, Advanced Vision Care, Los Angeles
• Clinical Professor of Ophthalmology, David Geffen School of Medicine, Jules Stein Eye Institute, UCLA, California
• avcmasket@aol.com
• Financial disclosure: Lecture fees (MicroSurgical Technology)
