



Multifocal IOLs have been implanted since 1986, and over that time they have evolved and improved greatly. Modern multifocal IOLs can be considered as a surgical treatment not only for cataract but also for refractive purposes when implanted after clear lens extraction. These lenses can be used to correct presbyopia, hyperopia, myopia, and, with toric multifocal models, astigmatism.
The primary aim of multifocal IOL implantation is to restore visual function and provide spectacle independence with a good level of patient satisfaction. With proper IOL selection and successful surgical technique, spectacle independence can be expected not only at distance but also at intermediate and near.1 In sports and other recreational activities, spectacle independence is desirable and can greatly improve a patient’s quality of life.
Most patients expect good visual outcomes after surgery, and most modern multifocal IOLs can deliver good near, intermediate, and distance vision. This is an improvement compared with previous generations of bifocal IOLs, with which intermediate vision was frequently compromised. Now with trifocal IOL technology, the addition of the intermediate focus has expanded the indication for this type of surgery to younger patients with a clear but dysfunctional crystalline lens.2
PATIENT SATISFACTION
Obtaining a good surgical result and patient satisfaction depends on careful preoperative planning and individualized IOL selection based on the patient’s preexisting conditions, visual needs, and realistic expectations. It also depends on the surgeon’s knowledge of the optical designs and visual performance of the available multifocal IOLs, proper surgical technique, and a comprehensive strategy for complications management.
The main reasons for patient dissatisfaction following multifocal IOL implantation are dry eye, residual refractive error (mainly astigmatism), and night vision complaints such as glare and halos.3,4
TYPES OF MULTIFOCAL IOLS
In order to disperse the light entering the eye to two different foci simultaneously, to provide far and near vision, a multifocal IOL either refracts or diffracts the light, or it does both. Therefore, multifocal IOLs are classified as having a refractive, diffractive, or combined mechanism.
Refractive mechanism. The refractive models achieve multifocality using annular zones with different refractive powers, and they generally provide acceptable far and intermediate vision. Their optical systems are dependent on pupil dynamics and diameter, are sensitive to postoperative decentration, may cause halos and glare, and inherently reduce contrast sensitivity.
Diffractive mechanism. Diffractive IOL models use diffractive rings distributed in a concentric fashion that either get closer to each other further from the center (apodized diffractive) or do not (nonapodized). These IOLs generally provide good far and near vision, but intermediate vision may not be satisfactory with bifocal models.5 They are not so dependent on pupil dynamics as refractive multifocals and are more tolerant to decentration, but they also can affect contrast sensitivity and can be associated with positive and negative dysphotopic optical phenomena.
Combined mechanism. Trifocal IOLs are a subtype of diffractive multifocal IOLs, designed to improve intermediate visual acuity by adding a third focus.6,7 A recent systematic meta-analysis of patient outcomes following implantation of trifocal or bifocal IOLs demonstrated that patients can achieve better intermediate visual acuity with a trifocal IOL than with a bifocal IOL without any adverse effect on distance or near acuity.8
BENEFITS AND POTENTIAL SIDE EFFECTS OF MULTIFOCAL IOLs
The primary purpose of multifocal IOLs is to provide patients with spectacle independence thanks to good UCVA at all distances. In numerous studies,1,8 implantation of refractive and diffractive multifocal IOL models has been shown to result in high levels of uncorrected distance and near visual acuity: mean uncorrected near and distance visual acuity was 20/25 or better in these studies, resulting in complete spectacle independence for about 75% of patients.
The downside of multifocal IOLs is that they are generally associated with more photic phenomena and decreased contrast sensitivity function in comparison with monofocal IOLs. Bifocal multifocals also tend to provide decreased visual acuity at intermediate, in comparison with far and near distance acuity.
Halos and glare are reported more often by individuals with a multifocal IOL compared to those with a monofocal IOL,3 and refractive multifocal IOLs appear to be associated with more photic phenomena compared with diffractive multifocal IOLs.3
CLINICAL STUDIES
We have been using trifocal technology since this type of multifocal IOL became available in Europe in 2012. Our practice has vast experience with almost every trifocal model available, including the AT LISA tri 839MP (Carl Zeiss Meditec), the FineVision POD F (PhysIOL), the AcrySof IQ PanOptix (Alcon), and, most recently, the RayOne Trifocal (Rayner, Figure 1).

Figure 1. The RayOne Trifocal IOL.
At the 2018 ESCRS meeting in Vienna, we shared our preliminary results with the RayOne Trifocal in 20 eyes of 10 patients. In terms of refractive outcome, all patients were within ±0.50 D of spherical equivalent target at 3 months postoperative. The safety and efficacy index was above 1.0 for all patients; mean binocular UCVA (logMAR) in these 20 eyes was 0.00 ±0.04 for distance, -0.10 ±0.07 for intermediate, and 0.10 ±0.08 for near (Figure 2).
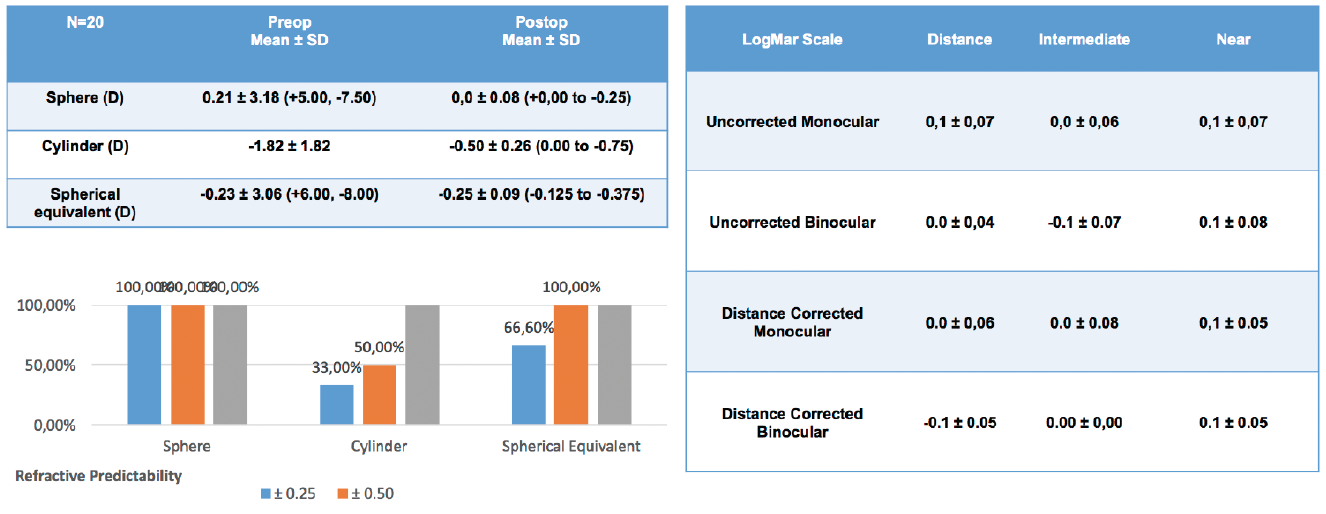
Figure 2. Preliminary results with the RayOne: All patients were within ±0.50 D of spherical equivalent target, and the safety and efficacy index was above 1.0 for all patients at 3 months postoperative.
The defocus curve also showed excellent visual outcomes at all distances at 3 months, even slightly improving the results compared with other trifocal IOLs previously studied in our department (Figure 3). In our initial series, because of the higher percentage of light transmission (89%) associated with the RayOne Trifocal when compared to other IOLs (86% with FineVision, 84% with AT LISA, and 88% with PanOptix), we also observed a significantly higher contrast sensitivity level under mesopic conditions (Figure 3).
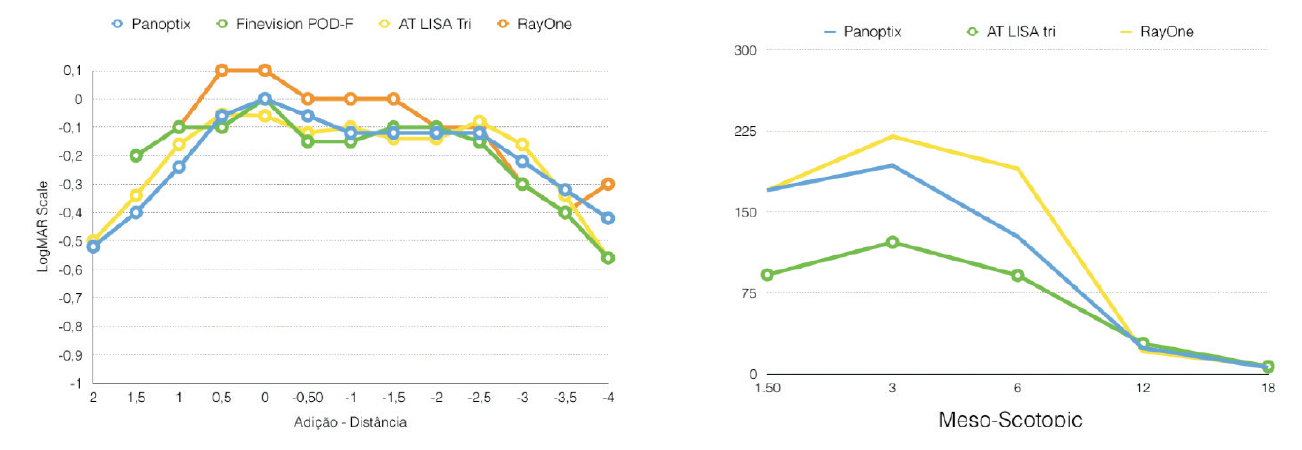
Figure 3. Preliminary results with the RayOne: Full spectacle independence and a significantly higher contrast sensitivity level under mesopic conditions was found at 3 months postoperative.
patient satisfaction
A recent meta-analysis of peer-reviewed publications revealed evidence of high levels of patient satisfaction in general with multifocal IOLs.9 Spectacle independence 80% or more of the time was reported by 91.6% of patients for distance vision, 100% for intermediate vision, and 70% for near vision among the different study populations.
Taking into consideration all the patients included in the studies, a binocular uncorrected visual acuity of 0.30 logMAR or better was achieved by 100% for distance, 96% for intermediate, and 97.3% for near visual acuity.
conclusion
Multifocal IOLs are good options to surgically correct presbyopia. Patients achieve spectacle independence in the majority of cases, with high levels of satisfaction. The visual needs of each patient should be carefully analyzed to choose the multifocal model that best fits each one’s lifestyle.2,3,5
As with all refractive procedures, appropriate patient selection and counseling are required, along with proper and accurate preoperative measurements. With recent advances in intraoperative techniques and multifocal IOL technology, these lenses can provide excellent outcomes with minimal risk of complications.
1. de Vries NE, Nuijts RM. Multifocal intraocular lenses in cataract surgery: literature review of benefits and side effects. J Cataract Refract Surg. 2013;39(2):268-278.
2. Jonker SM, Bauer NJ, Makhotkina NY, Berendschot TT, van den Biggelaar FJ, Nuijts RM. Comparison of a trifocal intraocular lens with a +3.0 D bifocal IOL: results of a prospective randomized clinical trial. J Cataract Refract Surg. 2015;41(8):1631-1640.
3. de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859-865.
4. Liu JW, Haw WW. Optimizing outcomes of multifocal intraocular lenses. Curr Opin Ophthalmol. 2014. 25(1):44-48.
5. Alfonso JF, Fernández-Vega L, Puchades C, Montés-Micó R. Intermediate visual function with different multifocal intraocular lens models. J Cataract Refract Surg. 2010;36(5):733-739.
6. Gatinel D, Houbrechts Y. Comparison of bifocal and trifocal diffractive and refractive intraocular lenses using an optical bench. J Cataract Refract Surg. 2013;39(7):1093-1099.
7. Madrid-Costa D, Ruiz-Alcocer J, Ferrer-Blasco T, García-Lázaro S, Montés-Micó R. Optical quality differences between three multifocal intraocular lenses: bifocal low add, bifocal moderate add, and trifocal. J Refract Surg. 2013;29(11):749-754.
8. Shen Z, Lin Y, Zhu Y, Liu X, Yan J, Yao K. Clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2017;7:45337.
9. Rosen E, Alió JL, Dick HB, Dell S, Slade S. Efficacy and safety of multifocal intraocular lenses following cataract and refractive lens exchange: Metaanalysis of peer-reviewed publications. J Cataract Refract Surg. 2016;42(2):310-328.
