

My current manual phaco technique, as shown in the accompanying Eyetube video (bit.ly/neuhann0220), begins with creation of sideport incisions at the 12 and 7 clock hours with a Zaldivar/Neuhann diamond knife (Huco). With the same knife, I construct a three-step incision at the temporal limbus, 2 mm wide and 1.5 mm in length (Figure 1). The anterior chamber is then filled with an OVD, in this case Amvisc (Bausch + Lomb). The capsulorhexis is created using Utrata forceps. I aim to create a 4.5-mm anterior capsular opening (Figure 2).
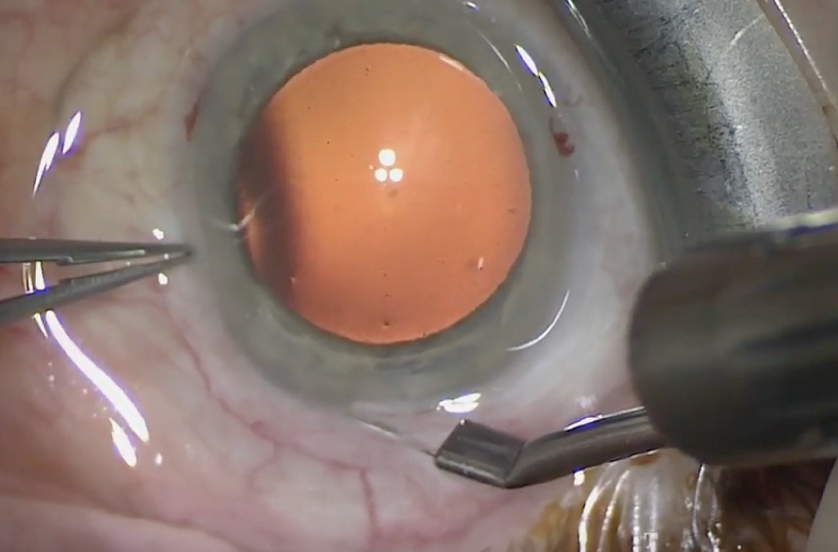
Figure 1. A three-step incision is constructed at the temporal limbus with a diamond knife.
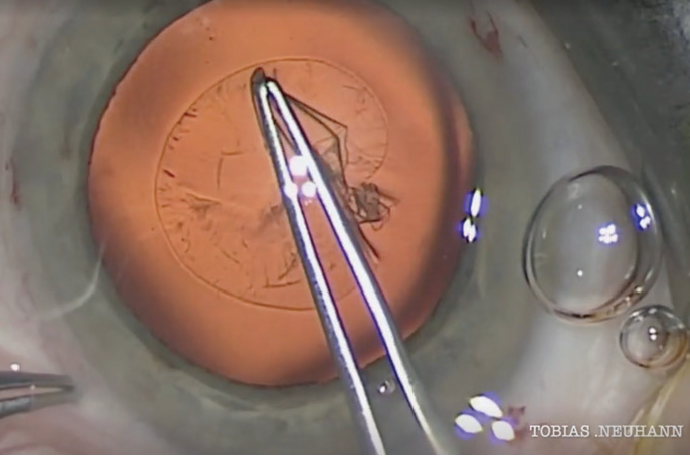
Figure 2. A 4.5-mm capsulorhexis is created with Utrata forceps.
With successful hydrodissection, all the following steps become much easier. I use a phaco chop technique, performed with the Neuhann chopper (Geuder) in my left hand. My strategy is to create four quadrants of the nucleus, which can then be easily aspirated and emulsified. The Adaptive Fluidics on the Stellaris Elite Vision Enhancement System (Bausch + Lomb) guarantees an amazingly stable anterior chamber. I like that it allows me to aspirate the quadrants into the center of the capsule and then safely emulsify them one by one.
I prefer to perform irrigation and aspiration of the cortex bimanually with the disposable VV650010 I/A handpiece tips (Oertli Instrumentes) as seen in the video. With the separate instruments I can perform what I call potato mashing, crushing small pieces of cortex as you can see in Figure 3.
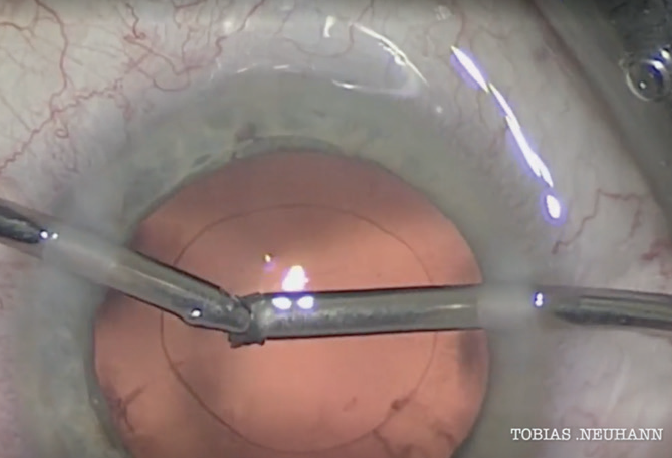
Figure 3. During bimanual irrigation and aspiration of the cortex, Dr. Neuhann performs potato mashing, crushing small pieces of cortex.
Using separate handpieces also allows me to polish the inner face of the anterior capsule around 360°. Although the value of this polishing process is controversial, in the past few years we have seen much less postoperative inflammation after capsule polishing. As a result of the reduced inflammation, we also seldom see postoperative cystoid macular edema in our patients.
Before IOL implantation, a Type 14A capsular tension ring (Morcher) is inserted under balanced saline solution, followed by the Acunex Vario hydrophobic extended depth of focus IOL (Teleon Surgical), which unfolds very smoothly (Figure 4).
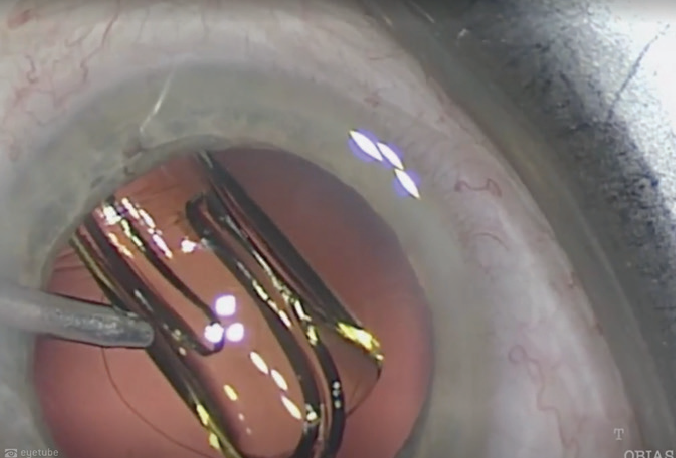
Figure 4. The IOL unfolds smoothly in the eye.
Closing the sideports with wound hydration then ends this successful surgery. Postoperatively, patients are typically prescribed bromfenac (Yellox, Bausch + Lomb).
CONCLUSION
The combination of innovative technologies such as the Neuhann chopper and Adaptive Fluidics with capsular tension ring insertion and new IOL designs helps me to achieve this manual cataract surgery technique quite simply in routine cases.
