

A routine cataract surgery technique is important for any surgeon to establish, but it can be especially crucial for high-volume surgeons who must ensure maximal efficiency and flow in the OR in order to manage a large daily case load. In a typical day, I perform about 20 cataract surgery procedures in our clinic, and one of my routine cases is detailed in an accompanying video on Eyetube (bit.ly/pajic0220) and in this article.
I use a femtosecond laser in cataract surgery on a routine basis to create the capsulotomy and incisions and to perform nucleus fragmentation. I prefer the Femto LDV Z8 (Ziemer) because it is easily integrated into our workflow without any time delay for the staff or for patients (Figure 1).

Figure 1. Using the femtosecond laser to create the capsulotomy and incisions and to perform nucleus fragmentation improves workflow in the OR.
The Z8 is a low-energy, high-frequency femtosecond laser. Its portable format means that it can be wheeled to where it is needed in our clinic. The laser comes with a no-touch liquid interface for cataract surgery that maintains the shape of the cornea. The suction system uses several sensors to ensure that the vacuum on the eye remains in effect during the cutting process.
The laser creates only a small amount of bubbles, so when surgery begins I always have a clear view. The clear corneal incisions open easily. I prefer to make them close to the limbus, which is possible with the Z8. My standard settings are 0.8 mm for the paracentesis and 2.2 mm for the main incision. The latter is a multiplanar, watertight incision. After this last laser step, the device is rolled away, and I continue with the surgery.
A cystotome is used to double-check the integrity of the capsulotomy (Figure 2). In more than 1,300 cases, I always have experienced a free-floating capsulotomy. In the case shown in the accompanying video, I used a spiderweb pattern of nucleus fragmentation with six segments and one ring. I fill the anterior chamber with Biolon OVD (Altacor Pharma), and I use balanced saline solution for hydrodissection.
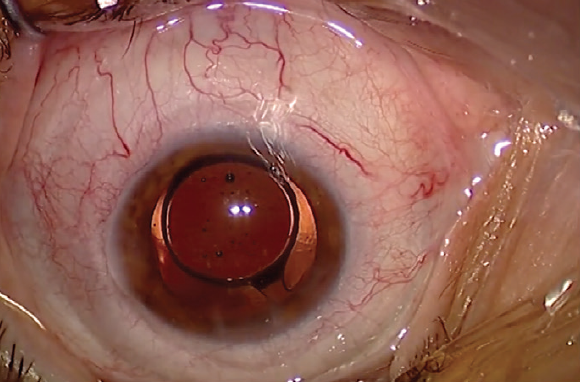
Figure 2. A cystotome is used to double-check the integrity of the capsulotomy.
NUCLEUS DIVISION
The phaco device I use is the CataRhex 3 (Oertli Instrumente). The tip is 2.2 mm in diameter, matching the width of the main incision (Figure 3). This is another advantage of a laser: I can program the width of the clear corneal incision to coordinate precisely with the size of the instruments I use.
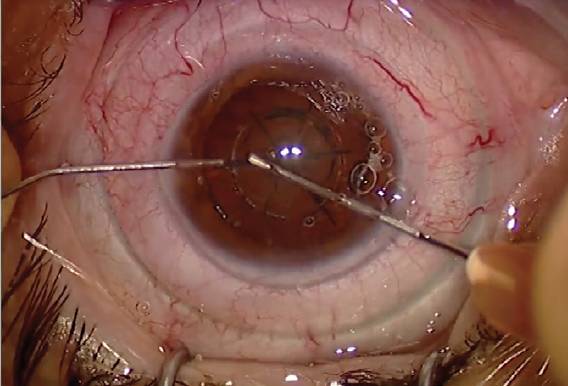
Figure 3. The incision size (2.2 mm) matches the size of the CataRhex 3 phaco tip.
For chopping, I use the Neuhann chopper (Geuder). It has a round tip that helps to prevent intraoperative trauma to the capsule. I use the stop-and-chop method. The CataRhex allows me to use high vacuum, up to 600 mm Hg, so I can easily mobilize the laser-fragmented nucleus, enabling a low effective phaco time.
Another important factor is not to move the phaco tip during the surgery. Rather, I deliver the segments to the phaco tip so that I do not stretch the main incision and it remains watertight.
I use disposable bimanual instruments (Bürki inno med) for irrigation and aspiration. When aspirating cortex, I do not feel a difference between laser cataract surgery and conventional cases. This might be because of the low energy the laser applies. There is no stickiness.
IOL INSERTION
The IOL I routinely use is the aspheric NS-60YG (Nidek). Because the main incision was precut to the right size by the laser, I do not need to expand the incision to accommodate the IOL injector, saving operative time. Before insertion, I fill the capsule with Biolon.
The haptics of the IOL should always be horizontal in order to prevent dysphotopsia (Figure 4). After the IOL is in place, I again use bimanual irrigation and aspiration to remove the remaining OVD, including from behind the IOL.
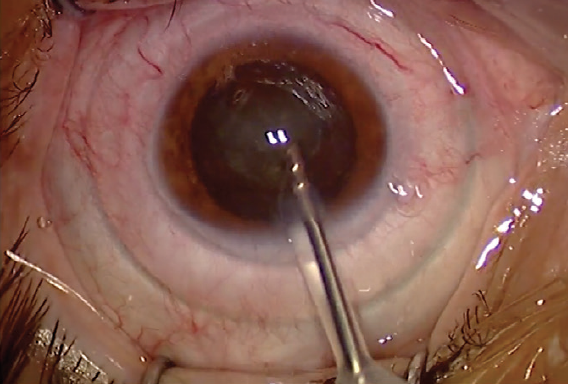
Figure 4. The haptics of the IOL are in a horizontal position.
Finally, I hydrate the paracentesis at the end of surgery and apply intracameral antibiotics, specifically Aprokam (cefuroxime, Thea Pharmaceuticals).
CONCLUSION
It takes me the same amount of time to perform conventional and laser cataract surgery procedures. It does not make a difference as far as patient scheduling is concerned. Rather, good OR flow is all about planning and organization.
