





IOL subluxation is a rare but serious complication. In most cases, dislocation occurs within 3 months of IOL implantation.1 Accumulating evidence links early IOL dislocation with poor fixation in the capsular bag; late dislocation is generally caused by progressive zonular insufficiency and contraction of the capsular bag years after uneventful cataract surgery.1-5
Despite technological and surgical advances, IOL subluxation remains challenging to manage.6-9 Many techniques have been described for fixating and repositioning a partially dislocated IOL. Some involve the use of sutures,10-15 and some do not.16-20 Each technique offers advantages and disadvantages, so the choice of strategy is made on a case-by-case basis.
DIAGNOSIS
A comprehensive history is the first step in the clinical assessment of a patient with a subluxated IOL. A detailed slit-lamp examination of the anterior and posterior segments is required. Direct ophthalmoscopy, anterior segment OCT, and B-scan ultrasound may be useful for locating a subluxated IOL. It is important to evaluate the position of the IOL while the patient is seated and again while the patient is supine. The severity of the dislocation can be assessed by measuring the change in the lens position.
TREATMENT OPTIONS
Observation. This is an option in the following situations:
- The severity of subluxation is low;
- The impact of IOL subluxation on visual acuity is insignificant;
- There is no evidence of an inflammatory response;
- The patient is not experiencing monocular diplopia or halos;
- No retinal complications are observed;
- The patient does not have glaucoma;
- Uveitis-glaucoma-hyphema syndrome is not observed; and
- There is a low risk of damage to neighboring ocular structures.
Otherwise, surgery may be indicated.21-26
IOL exchange. This is one of the most popular surgical strategies for managing a subluxated IOL. Many effective techniques to remove a dislocated IOL have been described. Most of them entail cutting the lens into two or three pieces with intraocular scissors before removing them.
Transscleral suture fixation. This is an effective surgical option for eyes with insufficient capsular support. The IOL is fixated between the vitreous cavity and the iris by blindly passing sutures from outside to inside (ab externo approach) or from inside to outside (ab interno approach) the eye.
A zigzag intrascleral suture or Z-suture is a knotless, rapid technique devised to fixate different IOL models in the ciliary sulcus. The use of a Z-suture eliminates the need for a lamellar groove or scleral flap. This technique can effectively reduce suture-related complications such as suture erosion, scleral atrophy, and infection. To our knowledge, a double-blinded randomized trial has not been conducted to compare the relative risks of each suture and lens type for transscleral fixation, so these decisions are based on the surgeon’s experience and preferences.11,15,27-34
Transscleral haptic fixation. If capsular support is inadequate, the Yamane technique for sutureless instrascleral fixation is an option. Two needles are used to externalize the haptics of a three-piece IOL. A flanged haptic tip is created and cauterized to be fixated intrasclerally (Figure 1). This technique reduces the risk of postoperative hypotony by minimizing the creation of sclerotomies. (For more on this subject, see “Yamane Tips and Tricks.”)
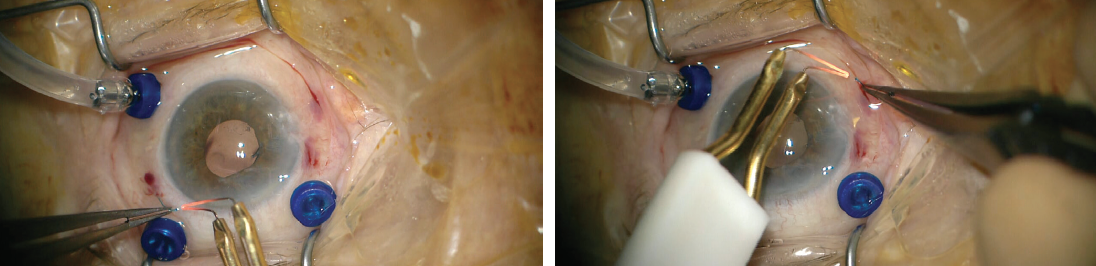
Figure 1. A flanged haptic tip is cauterized to be fixated intrasclerally.
A recently described technique involves the use of a scleral-fixated, foldable, sutureless IOL (Carlevale, PhysIOL). This lens’ T-shaped harpoons are not subject to rupture, deformation, or dislocation after fixation to the sclera (Figure 2). Studies have shown implantation of the Carlevale lens to be safe and fast, and the lack of scleral pockets reduces the risk of suture-related complications.35-37
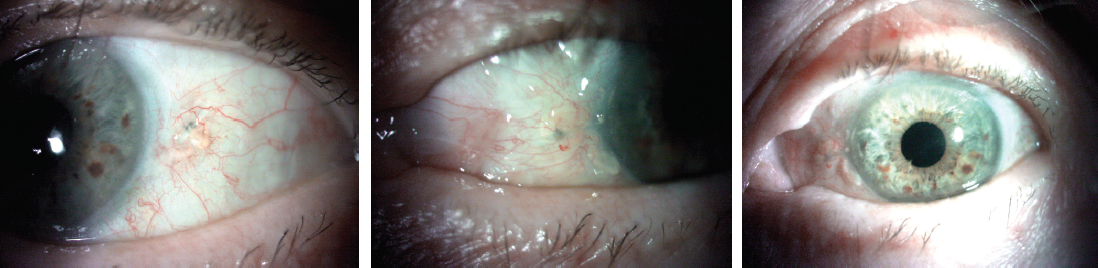
Figure 2. The Carlevale IOL in situ.
COMPLICATIONS AND PROGNOSIS
Evidence suggests that IOL subluxation can cause complications such as infection, hypopyon, retinal detachment, inflammation, bleeding, recurrent IOL dislocation, and elevated IOP.38-40 Transscleral suture fixation to address exposed sutures can increase the risk of infection, tissue erosion, and IOL subluxation.22,41,42 When transscleral haptic fixation is performed, the implantation of the IOL haptics through uveal tissue is associated with an increased risk of hemorrhage.19
Surgery successfully addresses IOL subluxation in a majority of cases. Poor outcomes are more likely in patients with diabetic retinopathy, preexisting ocular pathology, iris neovascularization, preoperative corneal disease, glaucoma, a history of retinal detachment, iritis, and corneal edema.43 Careful surgical planning based on the patient’s expectations, symptoms, and history of trauma can reduce the risk of complications in these cases.
1. Ascaso FJ, Huerva V, Grzybowski A. Epidemiology, etiology, and prevention of late IOL-capsular bag complex dislocation: review of the literature. J Ophthalmol. 2015;2015:805706.
2. Böke WR, Krüger HC. Causes and management of posterior chamber lens displacement. J Am Intraocul Implant Soc. 1985;11(2):179-184.
3. Schneiderman TE, Johnson MW, Smiddy WE, Flynn HW Jr, Bennett SR, Cantrill HL. Surgical management of posteriorly dislocated silicone plate haptic intraocular lenses. Am J Ophthalmol. 1997;123(5):629-635.
4. Hayashi K, Hirata A, Hayashi H. Possible predisposing factors for in-the-bag and out-of-the-bag intraocular lens dislocation and outcomes of intraocular lens exchange surgery. Ophthalmology. 2007;114(5):969-975.
5. Krėpštė L, Kuzmienė L, Miliauskas A, Janulevičienė I. Possible predisposing factors for late intraocular lens dislocation after routine cataract surgery. Medicina (Kaunas). 2013;49(5):229-234.
6. Davis G. The evolution of cataract surgery. Mo Med. 2016;113(1):58-62.
7. Micieli JA, Arshinoff SA. Cataract surgery. CMAJ. 2011;183(14):1621.
8. Shah MA, Shah SM, Mehta R, Shah P. Spontaneous dislocation of lens bag with acrylic lens after uneventful cataract surgery – unusual complication of cataract surgery. GMS Ophthalmol Cases. 2015;5:Doc11.
9. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013;39(9):1383-1389.
10. Hoffman RS, Fine IH, Packer M. Scleral fixation without conjunctival dissection. J Cataract Refract Surg. 2006;32(11):1907-1912.
11. Khan MA, Gupta OP, Smith RG, et al. Scleral fixation of intraocular lenses using Gore-Tex suture: clinical outcomes and safety profile. Br J Ophthalmol. 2016;100(5):638-643.
12. Lewis JS. Ab externo sulcus fixation. Ophthalmic Surg. 1991;22(11):692-695.
13. Malbran ES, Malbran E Jr, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986;9(2-3):151-160.
14. Mittelviefhaus H, Wiek J. A refined technique of transscleral suture fixation of posterior chamber lenses developed for cases of complicated cataract surgery with vitreous loss. Ophthalmic Surg. 1993;24(10):698-701.
15. Szurman P, Petermeier K, Aisenbrey S, Spitzer MS, Jaissle GB. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol. 2010;94(2):167-169.
16. Abbey AM, Hussain RM, Shah AR, Faia LJ, Wolfe JD, Williams GA. Sutureless scleral fixation of intraocular lenses: outcomes of two approaches. The 2014 Yasuo Tano Memorial Lecture. Graefes Arch Clin Exp Ophthalmol. 2015;253(1):1-5.
17. Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008;34(9):1433-1438.
18. Prenner JL, Feiner L, Wheatley HM, Connors D. A novel approach for posterior chamber intraocular lens placement or rescue via a sutureless scleral fixation technique. Retina. 2012;32(4):853-855.
19. Scharioth GB, Prasad S, Georgalas I, Tataru C, Pavlidis M. Intermediate results of sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2010;36(2):254-259.
20. Yamane S, Inoue M, Arakawa A, Kadonosono K. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology. 2014;121(1):61-66.
21. Gimbel HV, Condon GP, Kohnen T, Olson RJ, Halkiadakis I. Late in-the-bag intraocular lens dislocation: incidence, prevention, and management. J Cataract Refract Surg. 2005;31(11):2193-2204.
22. Lorente R, de Rojas V, Vazquez de Parga P, et al. Management of late spontaneous in-the-bag intraocular lens dislocation: retrospective analysis of 45 cases. J Cataract Refract Surg. 2010;36(8):1270-1282.
23. Gross JG, Kokame GT, Weinberg DV; Dislocated In-The-Bag Intraocular Lens Study Group. In-the-bag intraocular lens dislocation. Am J Ophthalmol. 2004;137(4):630-635.
24. Masket S, Osher RH. Late complications with intraocular lens dislocation after capsulorhexis in pseudoexfoliation syndrome. J Cataract Refract Surg. 2002;28(8):1481-1484.
25. Lim MC, Doe EA, Vroman DT, Rosa RH Jr, Parrish RK II. Late onset lens particle glaucoma as a consequence of spontaneous dislocation of an intraocular lens in pseudoexfoliation syndrome. Am J Ophthalmol. 2001;132(2):261-263.
26. Jones NP, Jalil A, Steeples LR. Management of subluxed and dislocated intraocular lenses in patients with uveitis: a practical approach. Ocul Immunol Inflamm. 2020 9:1-6.
27. Assia EI, Nemet A, Sachs D. Bilateral spontaneous subluxation of scleral-fixated intraocular lenses. J Cataract Refract Surg. 2002;28(12):2214-2216.
28. Borkenstein AF, Reuland A, Limberger IJ, Rabsilber TM, Auffarth GU. Transscleral fixation of a toric intraocular lens to correct aphakic keratoplasty with high astigmatism. J Cataract Refract Surg. 2009;35(5):934-938.
29. Chang DF. Disruptive innovation and refractive IOLs: how the game will change with adjustable IOLs. Asia Pac J Ophthalmol (Phila). 2019;8(6):432-435.
30. Emanuel ME, Randleman JB, Masket S. Scleral fixation of a one-piece toric intraocular lens. J Refract Surg. 2013;29(2):140-142.
31. Morgan-Warren PJ, Andreatta W, Patel AK. Opacification of hydrophilic intraocular lenses after Descemet stripping automated endothelial keratoplasty. Clin Ophthalmol. 2015;9:277-283.
32. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31(7):1320-1326.
33. Wasiluk E, Krasnicki P, Dmuchowska DA, Proniewska-Skrętek E, Mariak Z. The implantation of the scleral-fixated posterior chamber intraocular lens with 9/0 polypropylene sutures – long-term visual outcomes and complications. Adv Med Sci. 2019;64(1):100-103.
34. Asadi R, Kheirkhah A. Long-term results of scleral fixation of posterior chamber intraocular lenses in children. Ophthalmology. 2008;115(1):67-72.
35. Rossi T, Iannetta D, Romano V, et al. A novel intraocular lens designed for sutureless scleral fixation: surgical series. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):257-262.
36. Vaiano AS, Hoffer KJ, Greco A, et al. Long-term outcomes and complications of the new Carlevale sutureless scleral fixation posterior chamber IOL. J Refract Surg. 2021 1;37(2):126-132.
37. Veronese C, Maiolo C, Armstrong GW, et al. New surgical approach for sutureless scleral fixation. Eur J Ophthalmol. 2020;30(3):612-615.
38. Jakobsson G, Zetterberg M, Sundelin K, Stenevi U. Surgical repositioning of intraocular lenses after late dislocation: complications, effect on intraocular pressure, and visual outcomes. J Cataract Refract Surg. 2013;39(12):1879-1885.
39. Kim SS, Smiddy WE, Feuer W, Shi W. Management of dislocated intraocular lenses. Ophthalmology. 2008;115(10):1699-1704.
40. Mello MO Jr, Scott IU, Smiddy WE, Flynn HW, Feuer W. Surgical management and outcomes of dislocated intraocular lenses. Ophthalmology. 2000;107(1):62-67.
41. Holt DG, Young J, Stagg B, Ambati BK. Anterior chamber intraocular lens, sutured posterior chamber intraocular lens, or glued intraocular lens: where do we stand? Curr Opin Ophthalmol. 2012;23(1):62-67.
42. Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support. Surv Ophthalmol. 2005;50(5):429-462.
43. Stark WJ, Worthen DM, Holladay JT, et al. The FDA report on intraocular lenses. Ophthalmology. 1983;90(4):311-317.
