



According to the Centers for Disease Control and Prevention, an epidemic is “an increase, often sudden, in the number of cases of a disease above what is normally expected in that population in that area.”1 To my mind, late subluxation of the IOL–capsular bag complex qualifies as an epidemic except that its prevalence has risen over decades with the universal adoption of the continuous curvilinear capsulorhexis (CCC) instead of suddenly. Most anterior segment surgeons who treat referred patients see several of these cases each week.
My choice of IOL and implantation technique in the presence of a weak capsular bag depends on the degree of zonular pathology and the patient’s age. The younger patients are, the more likely they are to live long enough to experience subluxation of the IOL.
CONSIDERATIONS
Sizing the CCC. Zonulopathy is often diagnosed when the capsule is first touched for CCC initiation. Difficulty penetrating the center of the anterior capsule with a cystotome and the appearance of striae that radiate peripherally signal that caution is required. In the presence of zonulopathy, the capsule demonstrates pseudoelasticity; it does not follow the expected vector of applied forces, which can lead to too large or too small an opening. More frequent regrasping of the flap is required to correct the vector, and the CCC is sized with a caliper, laser-marked forceps, or a reticule in the microscope. The goal is to create a CCC sized to allow optic capture (ie, approximately 5 mm; Figure 1).
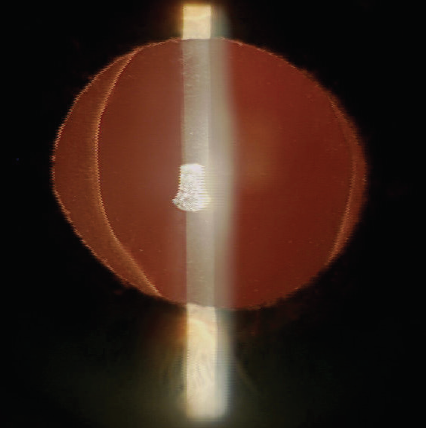
Figure 1. A CCC sized to allow optic capture.
If an IOL is ultimately implanted in the bag, the optic can be used as a template for enlarging a capsulorhexis that is too small. This is done so that it barely covers the optic edge just after IOL implantation and before OVD removal (safe even in the presence of an implanted capsular tension ring). Leaving a small CCC opening invites phimosis in almost any eye and possibly subluxation.
Choice of IOL material. Acrylic material is generally considered to be more compatible with the capsule than silicone. Subluxation of the IOL–capsular bag complex, however, has been reported with every IOL material when the lens is placed in the bag.
Traumatic zonulolysis. In the setting of traumatic zonulolysis, because there is no underlying progressive zonulopathy, I implant a standard one-piece hydrophobic acrylic IOL in the bag. If there are more than 3 clock hours of zonulolysis, if the lens does not center well, or if pseudophacodonesis is suspected, I fixate the IOL to the sclera using an Ahmed Capsular Tension Segment (Morcher) and an 8-0 PTFE suture (GoreTex, W.L. Gore & Associates). This requires a sub-Tenon injection of lidocaine over the anticipated scleral incision for the patient’s comfort. I avoid plate-haptic and accommodating IOLs in eyes with zonulolysis after significant trauma.
Pseudoexfoliation. I also never implant a plate-haptic or accommodating lens in the presence of pseudoexfoliation (PXF). Patients with PXF syndrome whose IOL is implanted in the bag require close monitoring with pupillary dilation during the early postoperative period to facilitate the diagnosis and treatment of phimosis with Nd:YAG laser anterior relaxing incisions. Phimosis can become evident within 2 weeks of surgery. Anterior relaxing incisions can halt progressive phacodonesis, but they must sometimes be repeated, possibly more than once, to achieve a stable capsular opening (Figure 2). Anterior relaxing incisions do not eliminate pseudophacodonesis, and therefore the impact on IOL subluxation is uncertain.
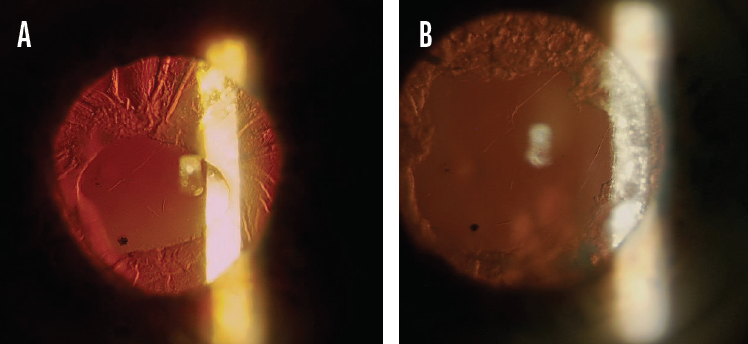
Figure 2. The first of two Nd:YAG laser anterior relaxing incisions (A). The anterior relaxing incisions were repeated a second time to achieve a stable capsular opening (B).
When PXF is diagnosed preoperatively, I am not only prepared to implant a capsular tension ring but also to abandon standard implantation of a one-piece acrylic IOL. If significant zonulopathy is present and particularly if the patient is young, my preference is to implant a three-piece hydrophobic acrylic IOL in the sulcus and to capture the optic through the anterior CCC.
The technique for optic capture is more nuanced in the presence of zonulopathy than in an eye with healthy zonules. If the zonules are heathy, the IOL is delivered into the sulcus, and pressure is applied to the optic 90º away from the optic-haptic junction on one side and then on the other. This pops the optic behind the CCC and changes the previously round edge into the classic football or cat’s eye appearance. When the zonular network is loose, a two-handed technique may be required to dunk the optic under the CCC edge and move the capture toward each optic-haptic junction on either side. This maneuver avoids placing stress on the zonules with the usual downward motion.
When I have executed this successfully, I have observed no pseudophacodonesis on postoperative day 1 or thereafter. In effect, the bag supports the IOL, and the optic supports the bag and physically prevents phimosis (scan the QR code now to watch a related procedure). Theoretically, if the zonules truly give out, the IOL–capsular bag complex could subluxate, but this occurrence has been exceedingly rare in my decades of practice.
Because this configuration almost always requires an Nd:YAG laser posterior capsulotomy, it is worth considering posterior optic capture in combination with polishing of the anterior capsule or, possibly, hyaloid-sparing double capture in patients with high myopia, diabetes, or significant zonular instability who are also at increased risk of complications in association with an open posterior capsule. To my knowledge, outcomes with these techniques in these populations have yet to be reported.
1. Centers for Disease Control and Prevention. Principles of epidemiology in public health practice, 3rd ed. An introduction to applied epidemiology and biostatistics. Accessed March 30, 2021. https://www.cdc.gov/csels/dsepd/ss1978/lesson1/section11.html#:~:text=Epidemic%20refers%20to%20an%20increase,more%20limited%20geographic%20area
