



A subluxated or highly mobile IOL almost always requires surgical management. When the optic of the IOL only partially covers the pupil, decreased or fluctuating vision often causes patients to feel dissatisfied with their outcomes. A subluxated IOL can be either sutured in place or exchanged. If repositioning the IOL, it is important to use an easy scleral fixation technique and a suture that will last for years. This article describes our preferred technique.
THE HOFFMAN TECHNIQUE
In our experience, a subluxated IOL is best repositioned with scleral fixation performed under the protection of a scleral flap. We prefer the transscleral technique first described by Hoffman and colleagues in 2006.1 In short, a scleral pocket is initiated through a peripheral clear corneal incision, followed by full-thickness passage of a double-armed suture through the scleral pocket and conjunctiva. The ends of the suture are then retrieved through the external corneal incision and tied.
This transscleral technique has several advantages. First, it creates a larger surface area for suture passes than the area created with triangular scleral flaps and grooves. The suture needles can therefore exit anywhere inside the large scleral pocket, provided they are at an appropriate distance from the limbus. Second, the Hoffman technique requires neither conjunctival dissection nor scleral cautery. We find that patients typically experience less discomfort with this fixation technique compared to others. Third, it is easy to execute this technique, and sutures are not required for wound closure. Fourth, the Hoffman technique can be performed with any IOL (although closed-loop lenses are ideal) sutured to the sclera so that the suture doesn't slip.
QUALITY SUTURES
Polypropylene sutures (9-0 and 10-0 Prolene, Ethicon) are most often used for scleral fixation. Some studies have shown, however, that 10-0 polypropylene sutures carry a higher risk (27.9%) of degradation over time than 9-0 polypropylene sutures,2,3 especially in young patients.4 Most surgeons therefore use 9-0 sutures.5-7
PTFE sutures (Gore-Tex, W.L. Gore & Associates) are another option. Their use is routine in cardiac valvular surgery and vascular procedures but is considered to be off-label in ophthalmology. During the past few years, however, some ophthalmologists have reported the utility of PTFE sutures for scleral fixation.
PTFE sutures have many advantages, including a high tensile strength and a lower risk of erosion and degradation8 compared to polypropylene sutures. Surgical steps may therefore be repeated without damaging the suture. Additionally, these sutures are highly visible and soft, they have minimal memory, and they are easy to handle.
In our experience, not only are PTFE sutures manageable, but their use also simplifies transscleral fixation. We have performed 10 cases with PTFE sutures and have not seen a single case of postoperative inflammation or temporary hypotony, which are the most common complications with transscleral fixation techniques.9
CASE SERIES
Surgical technique. In our series of 10 cases, eight of the IOLs that had subluxated were acrylic foldable one-piece monofocal IOLs, and two were acrylic foldable three-piece monofocal IOLs.
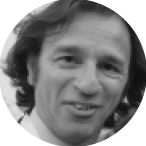
Scan the QR code now to watch a demonstration of our surgical technique. The positions of the corneal incisions were marked in a meridian that could help with positioning the IOL loops. Of note, the 3 and 9 clock positions should be avoided because placement in these meridians can promote damage to the long posterior ciliary arteries. The 3-mm corneal incisions were made 180º from each other and 300 to 400 µm deep in clear cornea. The 30º blade was inserted anterior to the conjunctival insertion at the limbus and through the corneal incision in order to create a scleral pocket. The 3 x 3-mm scleral pockets (Figure 1) were created posterior to each corneal incision with a crescent knife. Two 1-mm paracentesis incisions (Figure 2), made from each corneal incision with a 30º knife, were used to pass the PTFE needles. The paracentesis incisions may also be placed adjacent to the clear corneal incisions.
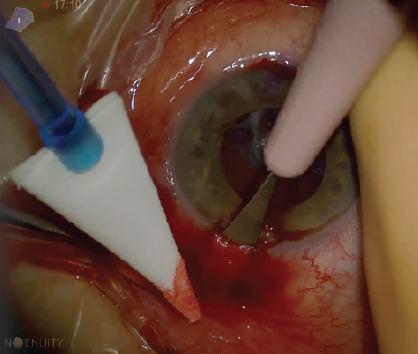
Figure 1. A scleral pocket.
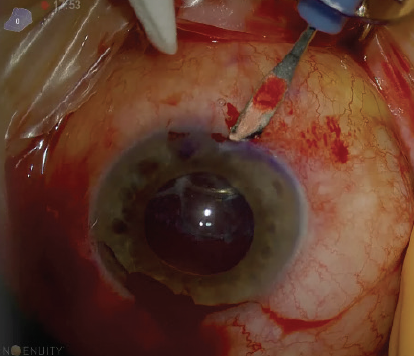
Figure 2. A paracentesis incision.
The anterior chamber was stabilized, and the endothelium was preserved by injecting an OVD through the paracentesis. A 25-gauge needle was passed transconjunctivally through the scleral pocket 1 mm posterior to the limbus and inserted behind the iris and the IOL haptic (Figure 3). The needle punctured the capsular bag and passed completely through the posterior and anterior capsules. A double-armed CV-8 PTFE suture was inserted through the opposite paracentesis and was docked into the 25-gauge needle (Figure 4). The sutures were removed externally from the scleral pocket and the conjunctiva. The PTFE needles were straightened in order to avoid damaging the corneal endothelium. Again, the 25-gauge needle was passed through the scleral pocket 1 mm posterior to the limbus and 1 mm adjacent to the first pass within the pocket. This time, the needle was passed in front of the IOL haptic without perforating the capsular bag.
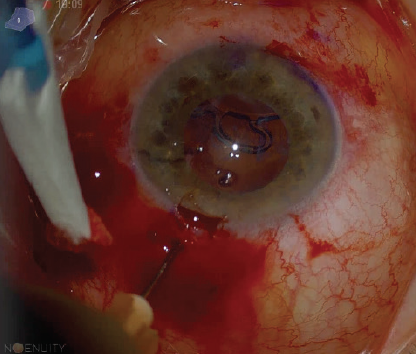
Figure 3. A sclerotomy with a 25-gauge needle.
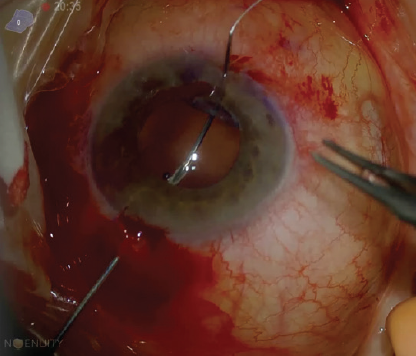
Figure 4. PTFE sutures are placed inside the 25-gauge needle.
The second needle of the double-armed PTFE suture was passed through the opposite paracentesis and docked into the 25-gauge needle. They were removed together through the sclera and the conjunctiva (Figure 5). The needles were removed, and the sutures were retrieved with a capsular hook through the limbal entrance of the scleral pockets (Figure 6). With the sutures in place 1 mm posterior to the limbus through the ciliary sulcus, the ends were tied, the lens was recentered (Figure 7), and the knots were buried in the scleral pockets (Figure 8).
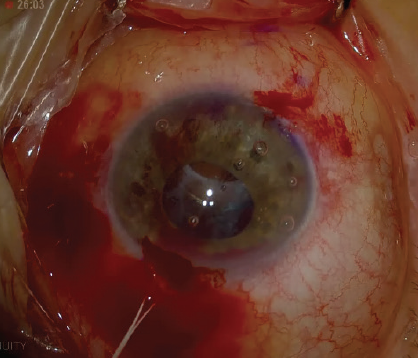
Figure 5. The suture is removed outside the sclera.
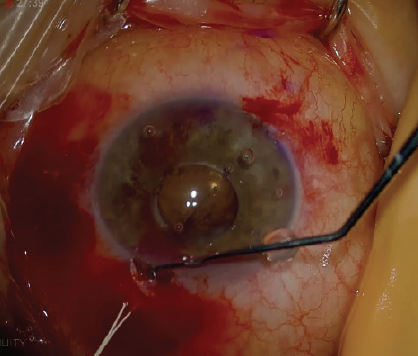
Figure 6. A capsular hook is used to retrieve the suture.
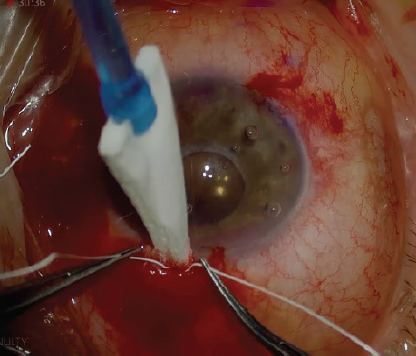
Figure 7. The suture knot.
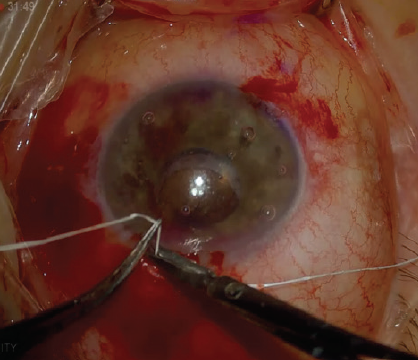
Figure 8. The suture cut.
The same technique was repeated on the opposite scleral pocket. At this point, all the sutures were in the ciliary sulcus through the full thickness of the sclera. No scleral or conjunctival sutures were required. Balanced salt solution was injected into the anterior chamber to flush out the OVD.
Results. All of the IOLs fixated with PTFE sutures were well centered—owing to the suture’s high tensile strength and low risk of erosion and degradation—and did not tilt during the 8-month follow-up period. Moreover, the larger size of the suture (7-0 vs 9-0 or 10-0 polypropolene) was well tolerated in the eye. The sutures slid under the sclera, and the knot disappeared into the pocket in a similar fashion as polypropylene sutures. Further, patients did not experience discomfort because the knots of the PTFE sutures were well buried in the scleral pockets (Figure 9).
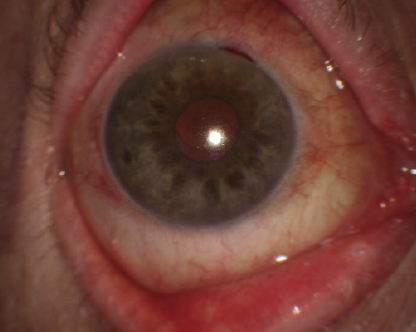
Figure 9. The postoperative appearance of an eye 1 week after transscleral fixation of a subluxated IOL with PTFE sutures.
Bleeding was observed in two patients, but the blood was reabsorbed within a few days without hyphema. In an early case of ours, the back of the 3/8 circle needle touched the endothelium, but the resultant endothelial damage resolved within a couple of weeks of the procedure. Thereafter, we started straightening the needles before each procedure to avoid this risk.
No early or late postoperative complications such as inflammation or endophthalmitis were encountered, and no hypotony or ocular hypertension was noted. Postoperative corneal edema occurred in three cases. With medical management, this settled after 1 week. No cystoid macular edema was noted. There was no breakage or erosion of the suture or IOL dislocation or tilt.
CONCLUSION
We prefer to start with the most conservative approach to managing a subluxated IOL, and in our hands, that is to suture the IOL to the sclera. Although the use of PTFE sutures in ophthalmology is off-label, their strength and maneuverability make them ideal for scleral fixation. Based on our experience performing the Hoffman fixation technique with PTFE sutures, they have become our first choice for stabilizing a decentered posterior chamber IOL.
1. Hoffman R, Fine IH, Packer M. Techniques: scleral fixation without conjunctival dissection. J Cataract Refract Surg. 2006;32:1907-1912.
2. Vote BJ, Trano P, Bunce C, Charteris DG, da Cruz L. Long term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141:308-312.
3. Parekh P, Green WR, Stark WJ, Akpek EK. Subluxation of suture-fixated posterior chamber intraocular lenses. Ophthalmology. 2007;114:232-237.
4. McAllister AS, Hirst LW. Visual outcomes and complications of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg. 2011;37:1263-1269.
5. Forlini M, Soliman W, Bratu A, Rossini P, Cavallini GM, Forlini C. Long-term follow-up of retropupillary iris-claw intraocular lens implantation: a retrospective analysis. BMC Ophthalmol. 2015;15:143.
6. Veronese C, Maiolo C, Armstrong GW, et al. New surgical approach for sutureless scleral fixation. Eur J Ophthalmol. 2020;30(3):612-615.
7. Yang JM, Yoon KC, YS Ji. Trans-scleral fixation of single-piece foldable acrylic lens with eyelets at optic-haptic junction. Can J Ophthalmol. 2015;50(5):367-372.
8. Scharioth GB. IOL fixation techniques. Retinal Physician. 2009;8:26-28.
9. Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008;34(9):1433-1438.