


The collective adoption of new technology and ways of thinking has been a common thread through many of my recent conversations. In 1962, Everett Rogers, a sociology professor, developed the diffusion of innovation curve (Figure 1) to describe the rate of adoption of innovation in a group of people, and it is still used today. The theory holds that more than half of people (68%) sit waiting and watching in the middle of the adoption curve while the innovators (2.5%) and the early adopters (13.5%) pave the way. The remaining 16% of people—the laggards—are averse to change and wait until the bitter end to get on board.1
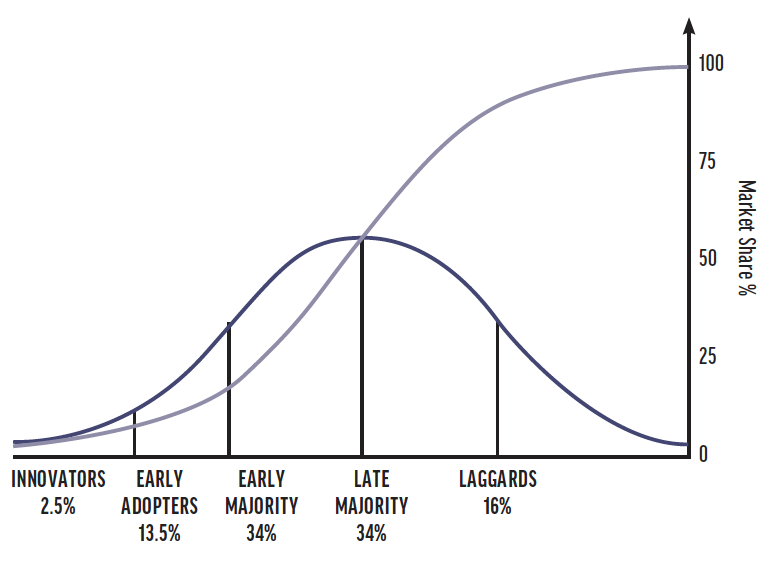
Figure 1. The diffusion of innovation curve remains an accurate prediction of market adoption of new technology or ideas.
The COVID-19 pandemic forced the world to adapt quickly to an ongoing and evolving situation. Ophthalmology practices had to be agile and open to new approaches to survive. The pandemic also seems to have softened long-held views about in-office cataract surgery and immediately sequential bilateral cataract surgery.
At the height of the pandemic, many cataract surgeons found themselves shut out of hospitals, unable to operate. For example, when the first wave of the pandemic hit the United Kingdom and Ireland, both governments moved to have the public health system hospitals focus on treating COVID-19 patients and asked private hospitals to provide all other care. This caused elective procedures such as cataract surgery to be put on hold in public hospitals and left many surgeons searching for alternatives. Some moved to private clinics, and others converted office space into a cataract surgery suite.
In this edition of Strategic Practice Management, I’ve asked James Ball, MA (Cantab), MB BChir, FRCOphth; Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth); and Daniel S. Durrie, MD, to elucidate the thought processes behind their decisions to add an in-office surgery suite and the requirements and challenges associated with it.
- Kristine Morrill, BS




FORCED CHANGE
James Ball, MA (Cantab), MB BChir, FRCOphth: Before the pandemic, I performed surgery at a large private hospital in Leeds, United Kingdom. When the pandemic hit, we had no business and no way of generating revenue.
Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth): For my practice in Ireland, cataract surgery in the private hospital represented just a portion of our revenue, so being shut out of the hospital was not a deal breaker. I know many surgeons, however, who relied solely on the hospital OR to generate revenue and suddenly found themselves with no income. It scared me.
Private hospitals generate much more revenue from various other surgical procedures than from cataract surgery. Ophthalmology is an afterthought, so I had already explored the idea of an in-office surgery suite before the pandemic. Being locked out of the hospitals pushed me to act on the idea.
Daniel S. Durrie, MD: We forget that cataract surgery was an in-patient procedure before it became a hospital outpatient procedure. In the United States and other countries, cataract surgeons started performing surgery in ambulatory surgery centers (ASCs) in the mid 1980s. When excimer lasers were first introduced, they were placed in hospitals or ASCs. Today, most laser refractive surgery is performed as an office-based procedure with no trade-off in safety. In Germany, private cataract surgeons have been performing in-office cataract and refractive surgery for the past 20 years, and they are considered the standard of care.
We are at a stage where the technology used for cataract surgery allows the procedure to be safely performed in our offices. More than 40,000 procedures have been successfully performed in an office-based setting. This shouldn’t be seen as controversial but rather as a natural evolution from ASCs.
THE PRACTICALITIES
Dr. Durrie: An in-office surgery suite is neither a procedure room nor a clean room. It is a full OR located in your practice. In addition to the initial investment required to establish an office-based surgery suite, economies of scale exist with it compared to building a standalone surgery center. You use the same front desk area, the same staff, and the same parking lot, for example. iOR Partners works with surgeons on implementation, staff training, and ongoing management.
Dr. Cummings: We initially considered working with Dr. Durrie’s company to build an OR in our eye clinic, but the pandemic complicated the logistics. Ultimately, we opted to purchase a SurgiCube (SurgiCube International), a system that creates a sterile environment for performing surgery.
Mr. Ball: We also opted for a SurgiCube. Fortunately, there was an empty office unit next door where we could install the OR. I like the fact that it’s portable. If we decide to move or outgrow our current premises, the SurgiCube can come with us.
The system uses unidirectional airflow to create a sterile field. The patient’s head, the surgeon, and the necessary equipment sit within this protected zone (Figure 2).

Figure 2. The SurgiCube in Mr. Ball’s in-office surgery suite.
Dr. Cummings: I used a particle counter to test the air quality within the SurgiCube. There must be fewer than 3,520 particles per cubic meter to avoid the risk of airborne pathogens. I tested the air quality in the hospital OR where I perform most of my cataract surgeries. Holding the device near the patient’s head, the count was about 900 particles per cubic meter (a very good score by any standard). Within the SurgiCube, the particle counter detected 0 particles per cubic meter measured from the same location.
Mr. Ball: Beyond the SurgiCube, you must invest in all the other surgical equipment, adapt your patient flow, and ensure you meet all regulatory requirements. In my experience, an increasing number of suppliers can provide the full range of cataract surgery equipment, from diagnostics through surgery.
The regulatory requirements vary by country. In the United Kingdom, the certification process is regulated by the Care Quality Commission.
Dr. Cummings: We plan to seek accreditation from the Joint Commission International, which should enable us to extend our care beyond private-paying patients to those with health insurance.
THE PATIENT EXPERIENCE
Dr. Cummings: An in-office surgery suite provides a better patient experience in the clinic, not because the hospital provides a subpar service but because it’s more efficient. Patients know the team and are in a familiar location.
Our experience with the SurgiCube is still early, but the first patients to experience it gave fabulous reviews. There’s no intravenous anesthesia, just topical, and oral diazepam. It’s the same experience now as a LASIK procedure.
Dr. Durrie: More than 20,000 procedures have been performed in iOR suites in the United States. When we surveyed the surgeons we work with, 95% said that office-based surgery improved patient satisfaction in their practice.
Mr. Ball: When patients arrive at our clinic, they come straight to the preoperative room, which is like a clinic room. They have surgery and then are moved to a relaxation area. It’s a perfect flow. Patients are then escorted to their car. I think having surgery in the office lowers their stress. A bonus is that my team’s stress levels are also lower working in an office-based OR. There’s no stress in the theater. We get through the cases quickly, and there is less pressure. I think patients pick up on that.
UNDERSTAND THE INVESTMENT UPFRONT
Dr. Cummings: We have two autoclaves for LASIK procedures, but we found that they weren’t ideal for phaco equipment. We bought a new autoclave for the SurgiCube that cost about €25,000. There is also the microscope, the phaco machine, the handpieces, the instruments, and instrument trays. It adds up quickly.
I encourage anyone considering an office-based OR to write a business plan for it. There are online templates that walk you through how revenue should look and whether or not it is a profitable investment.
Mr. Ball: Run the numbers and read the fine print in the contracts with suppliers. Look at the big capital expenses and obtain data from the suppliers on how often their equipment breaks down. They have the information but won’t present it if you don’t request it, and it can have a significant impact on the bottom line. Learn how long it typically takes to fix their equipment and what their commitment is to you to get things turned around.
THE PREMIUM BENEFIT
Dr. Durrie: Apart from the initial investment and setup, an office-based surgery suite is probably the easiest thing to do to increase your volume of premium procedures. One key reason is that you can provide a LASIK-like experience in the office setting. In the United States, many surgeons who establish an in-office OR have been able to double the percentage of premium procedures performed in their practice.
Mr. Ball: Adding an in-office surgery suite has positively affected the number of premium cataract surgeries performed in my practice. It’s important to ensure patient safety and outcomes are the primary motivation behind any decision made for your practice. If they are your guiding light, it’s amazing how straightforward difficult decisions can become.
1. Rogers EM. Diffusion of Innovations. New York: Free Press of Glencoe; 1962.
