




Refractive Outcomes After Descemet Membrane Endothelial Keratoplasty + Cataract/ Intraocular Lens Triple Procedure: A Fellow Eye Comparison
Augustin VA, Weller JM, Kruse FE, Tourtas T1
Industry support: None
ABSTRACT SUMMARY
A retrospective fellow eye analysis evaluated whether the refractive spherical equivalent shift (RSES) after Descemet membrane endothelial keratoplasty (DMEK) combined with phaco cataract surgery and IOL implantation (ie, triple procedure) in the second eye followed the RSES in the first eye. Investigators analyzed the 3-month outcomes of 127 patients with Fuchs endothelial corneal dystrophy (FECD; Krachmer grade 5) and comparable mean preoperative data, including spherical equivalent, BCVA, central corneal thickness, and posterior corneal curvature. The RSES was calculated as the difference between the manifest refraction spherical equivalent and the residual refractive error predicted by optical biometry with the Haigis formula (ie, target refraction). All patients received a monofocal, spherical, one-piece hydrophilic IOL with a hydrophobic surface.
Study in Brief
A retrospective study evaluated the refractive shifts experienced by patients with Fuchs endothelial corneal dystrophy who underwent a bilateral triple procedure (Descemet membrane endothelial keratoplasty combined with cataract extraction and IOL implantation). The refractive shifts observed in the first and second eyes were comparable.
WHY IT MATTERS
The refractive shift after the triple procedure is difficult to predict. The study indicated that the refractive outcome of the first eye may be used to predict the refractive target of the second eye.
Three months after surgery, the visual and anatomic outcomes were comparable between both eyes. The mean hyperopic RSES was 0.98 ±0.89 D, with a mean difference between the first and second eyes of 0.49 ±0.43 D in a paired analysis. The difference between mean RSES in the first and second eyes, however, did not reach statistical significance.
DISCUSSION
In the study by Augustin et al,1 the RSES after DMEK ranged from -1.51 to +3.72 D, highlighting the relative refractive unpredictability of the corneal procedure. DMEK is superior to Descemet stripping endothelial keratoplasty and penetrating keratoplasty in terms of refractive outcomes, but changes of 1.00 D or more in the target refraction occur in as many as 35% of DMEK eyes.2 The main issue with refractive accuracy in FECD eyes is an overestimation of corneal power, largely due to posterior corneal changes that disrupt the corneal anterior-posterior relationship.2,3
Disease stage was similar in both eyes in the study by Augustin et al.1 Using the first eye as a reference for the second eye appeared to be a valid strategy, and it was extrapolated from crystalline lens surgery on non-FECD eyes. Notably, although this approach showed good predictability, graph interpretation suggested that significant interocular RSES differences still occurred in 20% of patients.
It is generally accepted that refractive stability is reached 3 months after DMEK, but many eyes experience refractive and topographic changes thereafter.2 An enhancement after DMEK should be postponed until refractive and topographic stability is confirmed. The decision to provide an enhancement should be made on a patient-by-patient basis.4 The risk of opacification is greater with hydrophilic versus hydrophobic IOLs; if the opacification is significant, an IOL exchange may be required, which puts the DMEK graft at risk.5
Refractive Accuracy in Eyes Undergoing Combined Cataract Extraction and Descemet Membrane Endothelial Keratoplasty
Campbell JA, Ladas JG, Wang K, Woreta F, Srikumaran D6
Industry support: J.G.L., Principal (Advanced Euclidean Solutions); D.S., Consultant (Alcon)
ABSTRACT SUMMARY
The retrospective cohort study evaluated the accuracy of five IOL formulas (Hoffer Q, SRK/T, Holladay 1, Barrett Universal II [BUII], and Haigis) in 86 FECD eyes that underwent the triple procedure and for which there was at least 3 months of postoperative follow-up. The investigators analyzed the accuracy of the formulas using a thick lens equation based on anterior and posterior corneal radii and corneal thickness acquired preoperatively with Scheimpflug corneal topography.
Study in Brief
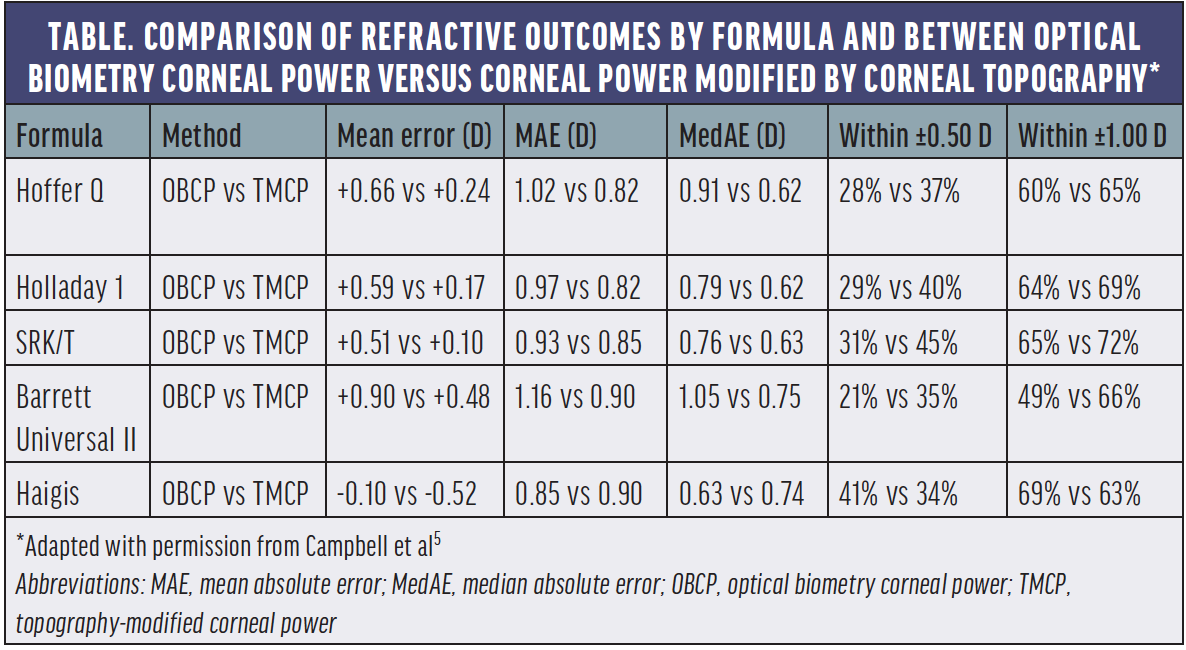
A retrospective cohort study of patients with Fuchs endothelial corneal dystrophy who underwent cataract extraction and IOL implantation combined with Descemet membrane endothelial keratoplasty (ie, triple procedure) found a mean hyperopic error for the Hoffer Q, SRK/T, Holladay 1, and Barrett Universal II formulas and a mean myopic error for the Haigis formula. Corneal power modification using topographic data resulted in significantly lower mean absolute errors with all but the Haigis formula.
Hyperopic errors had weak but significant positive correlations with preoperative posterior corneal curvature and posterior asphericity.
WHY IT MATTERS
When a thick lens equation modification of corneal power was used, the accuracy of most of the evaluated IOL formulas in eyes that underwent the triple procedure improved significantly. The Haigis formula may yield the highest refractive accuracy in this patient population.
The Hoffer Q, SRK/T, Holladay 1, and BUII formulas produced a mean hyperopic error, and the Haigis formula produced a mean -0.10 D myopic error. The Haigis and the BUII formulas exhibited the highest and the lowest refractive predictability, respectively (Table). Corneal power modification yielded a significantly lower corneal power than optical biometry measurements and significantly improved accuracy with all but the Haigis formula.
DISCUSSION
Corneal topography/tomography (and probably corneal densitometry) is essential to understand the impact of posterior corneal changes in patients with FECD. The study by Campbell et al demonstrated relative refractive unpredictability after DMEK.6 The mean postoperative manifest refraction spherical equivalent was -0.29 D, but the range was -4.25 to +2.25 D. Moreover, 40% of eyes ended up hyperopic, and only 50% to 70% of eyes were within ±1.00 D of the target refraction using optical biometry corneal power measurements.
Incorporating corneal topographic/tomographic parameters, including asphericity, corneal posterior curvature, and central-peripheral thickness relationship, into IOL power determination may improve refractive results after DMEK. IOL formulas that account for central corneal thickness may be affected by the limitations inherent to isolated measurements of this parameter in FECD eyes because changes in corneal thickness after DMEK contribute to the RSES.3 The Haigis and other formulas using corneal power modification improved refractive accuracy, but newer formulas (eg, seven-variable vergence, AI, and ray-tracing) may improve it further.7 Studies addressing DMEK refractive outcomes have placed emphasis only on spherical equivalent. Up to one-third of eyes, however, may experience a change in cylinder that is greater than 1.00 D,2 although DMEK produces small mean changes in astigmatism.8
Refractive unpredictability after DMEK poses challenges for the use of toric and presbyopia-correcting IOLs in eyes that undergo the triple procedure.9,10 Comparisons of staged surgery (ie, cataract and IOL surgery followed at a later date by DMEK) versus the triple procedure yield conflicting results.11 Attractive alternatives include the following:
- Phakic DMEK followed by cataract surgery and the implantation of a presbyopia-correcting IOL12; and
- The use of a Light Adjustable Lens (RxSight), which can theoretically correct up to 2.00 D of residual sphere and up to 3.00 D of cylinder.13
1. Augustin VA, Weller JM, Kruse FE, Tourtas T. Refractive outcomes after Descemet membrane endothelial keratoplasty + cataract/intraocular lens triple procedure: a fellow eye comparison. Cornea. 2021;40(7):883-887.
2. van Dijk K, Rodriguez-Calvo-de-Mora M, van Esch H, et al. Two-year refractive outcomes after Descemet membrane endothelial keratoplasty. Cornea. 2016;35(12):1548-1555.
3. Diener R, Eter N, Alnawaiseh M. Using the posterior to anterior corneal curvature radii ratio to minimize the risk of a postoperative hyperopic shift after Descemet membrane endothelial keratoplasty. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1065-1071.
4. Moura-Coelho N, Manero F, Papa R, Amich N, Cunha JP, Güell JL. Photorefractive keratectomy after DMEK for corneal decompensation by phakic IOL. Published online January 6, 2022. Eur J Ophthalmol. doi:10.1177/11206721211073429
5. Moura-Coelho N, Güell JL, Papa R, et al. Visually significant IOL opacification following DMEK. Poster presented at: 12th EuCornea Congress, September 25, 2021; virtual meeting.
6. Campbell JA, Ladas JG, Wang K, Woreta F, Srikumaran D. Refractive accuracy in eyes undergoing combined cataract extraction and Descemet membrane endothelial keratoplasty. Br J Ophthalmol. 2022;106(5):623-627.
7. Knutsson KA, Savini G, Hoffer KJ, et al. IOL power calculation in eyes undergoing combined Descemet membrane endothelial keratoplasty and cataract surgery. J Refract Surg. 2022;38(7):435-442.
8. Deng SX, Lee WB, Hammersmith KM, et al. Descemet membrane endothelial keratoplasty: safety and outcomes: a report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(2):295-310.
9. Yokogawa H, Sanchez PJ, Mayko ZM, Straiko MD, Terry MA. Astigmatism correction with toric intraocular lenses in Descemet membrane endothelial keratoplasty triple procedures. Cornea. 2017;36(3):269-274.
10. Trindade BLC, Garcia JC, Nogueira LR. Toric IOL in combined DMEK and cataract surgery. Clin Ophthalmol. 2021;15:1511-1516.
11. Semler-Collery A, Bloch F, Hayek G, Goetz C, Perone JM. Comparison of triple-DMEK to pseudophakic-DMEK: a cohort study of 95 eyes. PLoS One. 2022;17(5):e0267940.
12. Price MO, Pinkus D, Price FW Jr. Implantation of presbyopia-correcting intraocular lenses staged after Descemet membrane endothelial keratoplasty in patients with Fuchs dystrophy. Cornea. 2020;39(6):732-735.
13. Eisenbeisz HC, Bleeker AR, Terveen DC, Berdahl JP. Descemet membrane endothelial keratoplasty and light adjustable lens triple procedure. Am J Ophthalmol Case Rep. 2021;22:101061.
