








Cathleen M. McCabe, MD: Presbyopia is an expanding market, and the number of patients who come to our practices seeking relief of their symptoms is steadily increasing. All of us on this virtual panel have experience with a variety of presbyopia correction methods. The aim of this discussion is to share our preferred treatments and thoughts on patient selection.
PHARMACOLOGIC DROPS
Dr. McCabe: Let’s jump right in and talk about the newest presbyopia treatment on the block, which is pharmacologic agents. Right now, the only available presbyopia drop is Vuity (pilocarpine HCl ophthalmic solution 1.25%, Allergan), but others are on the way. I am fully in the depths of presbyopia now, and I feel like I better understand the struggles that our patients have. Who else on the panel is presbyopic?
Stephen G. Slade, MD, FACS: I am.
Audrey R. Talley Rostov, MD: I’m also enduring presbyopia.
Dr. McCabe: Who has prescribed or maybe even used Vuity themselves?
Dr. Slade: I have prescribed it. I use monovision—which I think is a wonderful tool for presbyopia—and I don’t even own readers. I have not used Vuity myself, but my wife has.
Dr. Talley Rostov: I also use monovision. I wear glasses to operate, but overall I’m okay with my monovision. I have tried Vuity on my husband, who can’t tolerate monovision. He said that the drops stung when he put them in and, although they made a difference in his vision, it was minimally noticeable to him. I wouldn’t call it a huge success but maybe a mild success.
Dr. McCabe: I also use a combination of mini-monovision and multifocal contact lenses, and I have tried Vuity on my spouse.
Mitchell C. Shultz, MD: I prescribe Vuity on a weekly basis. There is a pool of patients—especially young patients with presbyopia and no experience with glasses—who do not want to wear reading glasses. The bottom line is this: If you choose the right patients, they are happy with the product.
Personally, I have used Vuity, but not daily. I had LASIK 26 years ago and have experienced a modest amount of regression. I have some uncorrected astigmatism and a little bit of myopia. I can function in the office without glasses. In low-light environments, however, I have difficulty reading menus and books. Instilling the drops controls my pupil size, which eliminates aberrations related to my astigmatism. When I am driving at night, the effect of having smaller pupils allows me to see a bit more clearly at distance, and my near vision improves as well. I would say I’m able to read print of every size for 4 to 5 hours after instilling the drops.
Dagny C. Zhu, MD: Patients come into my practice every day asking to be glasses-free. I probably see five to 10 good candidates for Vuity per week. These patients have early presbyopia and are not ready for surgery. I don’t feel comfortable doing a refractive lens exchange (RLE) in an eye with ametropia and a fully or even partially functioning lens. Many of them don’t tolerate monovision because they’ve had perfect vision their entire lives. I think Vuity is a good option for patients in this group.

PHARMACOLOGIC DROPS
Have you prescribed Vuity (pilocarpine HCl ophthalmic solution 1.25%, Allergan) or used another presbyopia-correcting drop?
Vuity is not available on the Turkish market yet, so I have no experience with the product or category.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
I explain to patients that no IOL technology can provide excellent UCVA at all distances. Optical principles and the law of physics prevent it. Patients must accept this reality. Accommodation, moreover, is a dynamic process. With current nonaccommodating presbyopia-correcting IOLs, we have been trying to find static solutions to a dynamic problem.
To choose the best IOL for a given patient, I begin by trying to understand their lifestyle. I inquire about night driving, their job and hobbies, and other aspects of life that can be affected by dysphotopsias and reduced contrast sensitivity.
If a patient desires excellent near vision and is not worried about night vision problems, I recommend a trifocal IOL. If a patient requires good contrast sensitivity or prioritizes nighttime vision, I recommend an extended depth of focus (EDOF) IOL and the use of a mini-monovision strategy targeting -0.50 D for the nondominant eye.
My use of EDOF IOLs has increased greatly during the past 2 years. As part of the consultation, I explain to patients that an IOL exchange is the only recourse if they continue to be bothered by halos and starbursts after a period of neural adaptation following the implantation of trifocal IOLs. In contrast, I say, the main disadvantage of EDOF IOLs is a potential inability to read small print, which can be addressed by wearing low-powered (0.50 D) reading glasses. The main thing is for patients to understand the pros and cons of each IOL category and to determine what they can accept.
I no longer offer enhanced monofocal IOLs because I found that they did not provide patients with good near vision for the long term. Some of my patients experienced increased near vision for the first few months after surgery, which was probably the result of pseudoaccommodation. Thereafter, however, their near vision decreased as the capsule contracted.
What are your thoughts on light adjustable lens technology?
I do not have experience with the Light Adjustable Lens (RxSight), but even adjustable IOLs are a static solution to a dynamic problem.
What are your thoughts on the use of small-aperture IOLs?
I do not have experience with small-aperture IOLs, but I think they are useful only for eyes with high or irregular astigmatism, not those with presbyopia.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
If you clearly explain to patients that all options have flaws and that no perfect solution to presbyopia exists, you can enjoy success with presbyopia-correcting lens technologies. It is also important to ensure that patients have realistic expectations and to explain that the quality of near vision and night vision are generally inversely correlated.
Do not offer IOL surgery as a solution to presbyopia to someone who retains some accommodative amplitude. In my experience, the best candidates for this form of treatment are at least 50 years old if they are emmetropic or myopic and at least 45 years old if they are hyperopic.
I recommend starting with hyperopic patients because they are likely to be happy after surgery. Be careful with myopic patients because they often have trouble understanding presbyopia and may be unhappy with their postoperative near vision.
CORRECTION ON THE CORNEA
What laser vision correction (LVC) strategy do you use for presbyopia correction? When is this the best option?
I do not use an LVC strategy for presbyopia correction.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
No. I think a virgin cornea offers a big advantage for cataract surgery. Corneal aberrations can negatively affect the performance of IOLs, particularly trifocal designs. Moreover, I do not like the idea of altering the cornea of someone who will probably need cataract surgery in 15 to 20 years.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
Understanding the patient’s lifestyle and expectations is essential, and effective communication is a must. Unrealistic expectations are a red flag for postoperative dissatisfaction.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
I begin by communicating the pros and cons of the treatment options clearly and factually. I find that this approach instills confidence and that patients return for treatment if they decide to proceed with surgery.
The response from patients has been variable. A few haven’t seen any improvement, but many like the effects of the presbyopia drop. I like to trial the drop in the office. Patients wait 15 minutes, and then I check their near vision. I’ve seen patients go from J10 to J1. That has been pleasantly surprising.
I find that Vuity works best in patients who are on the younger side—in their early 40s—and seeing about J3. The drop can get them to a sharper J1, sometimes even J1+. Occasionally, an older patient will have a remarkable response.
Dr. Shultz: I think pretty much anyone with early presbyopia is a good candidate. The key is to consider the total plus prescription and uncorrected refractive error if the patient is hyperopic. I pay particular attention to the uncorrected plus spherical equivalent (SE). I know that a young patient with low hyperopia in the range of 1.00 to 2.25 D SE can benefit from Vuity. I find that treatment can benefit slightly older patients like me who have low myopia (-0.50 to -1.00 D SE) at distance with a total uncorrected near demand of up to 2.00 D SE. Not only can the drops benefit phakic individuals, but pseudophakic patients who have received a presbyopia-correcting IOL andå even some who have not benefit.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
No. They are not yet available in my country.
Where do you expect drops to fit into your treatment paradigm for presbyopia correction once they are available in your country?
Currently, no form of presbyopia correction can preserve the distance vision of patients with emmetropic presbyopia. I believe this is the niche for presbyopia drops.
Who are the most appropriate patients for presbyopia drops?
Many patients will be willing to try the drops, but their side effects and efficacy will determine who continues using them.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
Trifocal and trifocal toric IOLs are my go-to lenses for patients who want a full range of vision and a maximum amount of spectacle independence. Good distance vision seems to be the minimum expected result of any cataract procedure. My patients are willing to pay a premium if they can also achieve good near vision. Among my patients, a minority have significant complaints about dysphotopisa after receiving a trifocal IOL.
What are your thoughts on the use of small-aperture IOLs?
I have participated in several clinical studies of the IC-8 IOL (now the IC-8 Apthera, AcuFocus) during the past 7 years. We found that, with a spherical equivalent of -0.75 D, patients’ distance, intermediate, and near UCVA was 20/25.1
I consider the IC-8 Apthera IOL to be a versatile and unique lens. Its pinhole optics extend depth of focus for presbyopia correction and can filter out unwanted aberrations in an eye with a complex cornea and distorted optics. The IC-8 Apthera can therefore be of particular benefit to patients with keratoconus or a history of corneal refractive surgery.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
Discuss presbyopia-correcting IOLs with all eligible patients. Describe the technology, set reasonable expectations, and let them decide if they are interested. Do your best to achieve the desired refractive outcome so the lens can function as it was designed to.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I perform presbyopic LASIK (Supracor, Bausch + Lomb) on the nondominant eye of patients with presbyopia and either hyperopia or myopia. I find that a refractive target of -0.50 D with the varifocal treatment generally provides patients with 20/25 distance, intermediate, and near UCVA. Standard LASIK with a distance target is performed on the dominant eye. With this modified monovision strategy, I can treat patients who are 40 to 60 years old and have a manifest refraction spherical equivalent of 3.00 to -6.00 D.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
It took some time for corneal scarring to occur and be recognized after the implantation of the first generation of corneal inlays. Allograft or allogenic inlays will have to overcome the history of the earlier devices and demonstrate long-term safety and efficacy.
What other future treatments have promise?
Laser scleral microporation is under investigation as a laser treatment for patients with emmetropic presbyopia. Four quadrants of the sclera are treated with an Er:YAG laser to uncrosslink the sclera and rejuvenate the accommodative mechanism (see video demonstration below). Treatment does not appear to affect the visual axis or alter the eye’s refractive status.2
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
For patients who are 40 to 60 years old and have presbyopia and clear lenses, I perform presbyopic LASIK, as described earlier. Patients who are older than 60 years of age undergo refractive lens exchange (RLE), and those with cataracts undergo cataract surgery and receive the IOL type of their choice.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
My center offers all subspecialty and optical services. By meeting all of a patient’s eye care needs, we establish a relationship with them and their families. Our center thus becomes the preferred provider for people of all ages.
1. Ang RE. Visual performance of a small-aperture intraocular lens: first comparison of results after contralateral and bilateral implantation. J Refract Surg. 2020;36(1):12-19.
2. Ang RE. Scleral uncrosslinking: a minimally invasive presbyopia solution. Paper presented at: ASCRS/AOA Annual Meeting; April 22, 2022; Washington, DC.
Dr. McCabe: I’ve had a similar experience. I think we’re figuring out where those sweet spots are, and sometimes they are not the patient you’d expect. I loved hearing everybody’s stories and learning how we can fit these drops into our practices’ offerings.
Brian M. Shafer, MD: I have had a hard time figuring out how to talk to patients about presbyopia drops. We know that patients who do best with the drops give them a 2-week trial before deciding if they like the effects or not. My challenge is this: How do I guide them through that journey?
In the first 2 weeks, patients may notice stinging upon instillation. Some say they get a little bit of dimness. One of our practice administrators who tried it described a similar sensation to what you get when you get off a cruise ship and still feel like you’re on the water!
Dr. McCabe: The stinging has not been a barrier for my patients. A few have experienced a headache associated with the use of the drops, and to your point, Dr. Shafer, some have experienced a difficult-to-describe sensation. Some patients explain it as feeling dizzy or like they’re in a movie. There is a neural adaptive part that happens in the early experience. Most patients do not have success with the drops on day 1, but if they are counseled on what to expect and are willing to try it for long enough that they notice the positive effects, then they can find success with the treatment.
Some patients want to use presbyopia drops daily, and others want to use them only at certain times when spectacle independence is most important to them. For me, the slam dunk patients for presbyopia drops are younger and don’t have a great need for a large increase in their near vision. We are still learning how best to prescribe these drops.
Dr. Zhu, I have two questions for you. First, would you prescribe presbyopia drops to patients with complex corneas? Second, do you think there’s a diagnostic role for presbyopia drops to predict how a patient might do with different technologies such as the small-aperture IOL?
Dr. Zhu: I am comfortable using presbyopia drops in patients with aberrated corneas. Pinhole optics filter out peripherally scattered rays. Reducing the size of the pupil creates a much sharper image. Patients who experience chronic halos and glare after LASIK or who have corneal scars or keratoconus are ideal for a pupil-modulating drop and, potentially, the IC-8 Apthera small-aperture IOL (AcuFocus).
Currently, I use presbyopia drops off label mainly for patients who have experienced dysphotopsias, halos, and glare after either LASIK or a multifocal lens. In the past, I used generic pilocarpine 1% for patients who needed something to help them drive at night. Compared to generic pilocarpine, Vuity is much more tolerable for my patients. Fewer of them complain about headache with Vuity compared to generic pilocarpine.
Dr. McCabe: I haven’t seen a lot of patients with headaches as a side effect with Vuity, either. I’ve also had some success in patients with either dysphotopsias or complex corneas.
Dr. Slade: The measure for success with any technology is twofold. First, what do patients think? Second, what do clinicians think? Some patients take issue with the duration of effect. Different formulations are coming, however, that may have a longer duration of effect. For clinicians, many of us want a product that acts as a bridge to keep patients in the practice from the LASIK age to the cataract age—from their 30s into their 60s or 70s. I’m not sure that presbyopia drops are going to provide that. I don’t think that they will tie patients to the practice. Patients will eventually go elsewhere to get the prescription.
Dr. McCabe: Do you think a longer-acting presbyopia drop would help bridge the gap between the LASIK patient who’s now presbyopic until they’re candidates for an RLE procedure?
Dr. Slade: A long-acting drop might work, but I’m not sure it’ll pass the real-world test as a temporary treatment.
Dr. Talley Rostov: I think of presbyopia drops as a temporary, cosmetic product that works well for certain scenarios such as reading a dinner menu without glasses. The product also works well for LASIK patients who are looking for a little better vision at near. When used in this fashion, presbyopia drops can, I think, bridge the gap between LASIK and RLE or cataract surgery. I think it is a really nice way of addressing presbyopia.
Dr. Zhu: I see it as a postsurgical adjunct, too. It can help to enhance near vision in patients who have a multifocal or extended depth of focus IOL and are not getting as much near vision as they want. For LASIK patients who can’t tolerate full monovision, I would consider using a mini-monovision strategy and prescribing Vuity. I feel like there could be more applications for postsurgical eyes than virgin eyes.
Dr. McCabe: I like that thought process. One of my patients who is happiest with Vuity has a Crystalens (Bausch + Lomb). The presbyopia drops improve her near vision and her distance vision to some degree, too. She has a little residual astigmatism. I agree the pharmacologic treatment could be a great adjunct, especially in the future as other formulations become available.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
Unfortunately, these eye drops are not yet approved in Egypt, where I practice.
Where do you expect drops to fit into your treatment paradigm for presbyopia correction once they are available in your country?
These pharmacologic agents are a reasonable alternative for patients who have presbyopia but no ametropia. Many of these individuals have no cataracts and are anxious for an alternative to reading glasses that allows them to perform near tasks with clear vision.
Who are the most appropriate patients for presbyopia drops?
Relatively young patients—around 45 years of age—who have presbyopia, clear crystalline lenses, and perfect distance vision without glasses but who have no ametropia.
How will the market change when other drops become available?
I think the availability of these agents may delay some patients’ desire for surgical correction of presbyopia for a few years. For example, some patients may choose to instill presbyopia drops until their dysfunctional lens index decreases to a level that affects their quality of vision. At that point, they are likely to seek an alternative solution in the form of lens-based refractive surgery. Other patients may use presbyopia drops until they tire of the side effects or the drops no longer allow them to perform near tasks without glasses. Cost may be another factor; the cost of a 2- to 3-year supply of these drops is almost equivalent to that of refractive surgery for presbyopia.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
I don’t consider enhanced monofocal or monofocal-plus IOLs to be presbyopia-correcting IOLs, and I do not present them as such to my patients. These IOLs do, however, provide a slight increase (approximately 0.50 D) in depth of focus, which can improve patients’ quality of life but not eliminate their need for spectacles for near vision. I am willing to implant enhanced monofocal lenses in eyes with diabetic maculopathy, glaucoma, or dry eye disease (DED) because I have not observed a drawback to doing so. I do not implant these IOLs in eyes with irregular corneas or a history of hyperopic LVC.
I am comfortable offering EDOF IOLs. I have found them to be more forgiving of inaccurate biometry measurements than trifocal IOLs. My patients are also less likely to experience halos with EDOF lenses than multifocal and trifocal IOLs that have diffractive optics. I am willing to implant a trifocal IOL if the patient fits the selection criteria, including the requirements for a pristine cornea, no DED, a healthy macula, and a small angle kappa. My preference for patients with presbyopia, however, is an EDOF IOL with refractive optics.
What are your thoughts on light adjustable lens technology?
I have no experience with the Light Adjustable Lens, but I think it is a milestone in presbyopia correction.
What are your thoughts on the use of small-aperture IOLs?
I have experience with the XtraFocus Pinhole Implant (Morcher). I consider the technology for patients with irregular corneas from past radial keratotomy (RK) or another cause. The implantation procedure can be tricky because the device must be perfectly centered on the visual axis. I recently implanted an XtraFocus for presbyopia correction in the nondominant eye of a patient and achieved a successful result.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
The design and optics of available presbyopia-correcting IOL models are superior to earlier generations of these lenses. Modern IOLs perform better at different ranges of vision and are associated with a lower amount of dysphotopsias. As I mentioned previously, I do not consider enhanced monofocal IOLs to be presbyopia-correcting IOLs. That said, the technology can be a great place to start for surgeons who are interested in offering presbyopia-correcting IOLs. Enhanced monofocal IOLs can increase depth of focus slightly without compromising quality of vision.
After a surgeon becomes comfortable with enhanced monofocal IOLs, I recommend gaining experience with EDOF IOLs that have refractive optics because they are more forgiving of subtle corneal surface irregularities, mild DED, and inaccurate biometry compared to trifocal IOLs. Some EDOF IOLs have no zones on their anterior and posterior surfaces and are thus less sensitive to decentration. The loss of contrast sensitivity is also generally not as great with EDOF IOLs compared to multifocal IOLs.
Once surgeons gain comfort and experience with enhanced monofocal and EDOF IOLs, they can consider adding trifocal IOLs to their offerings.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I prefer to create a hyperprolate cornea using a mini-monovision strategy in the patient’s nondominant eye. I have found the best candidates for this treatment are between 40 and 50 years old and have low to moderate hyperopia and clear crystalline lenses.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
I think allograft inlays may overcome most of the limitations associated with earlier corneal inlays.
What other future treatments have promise?
I expect the future to favor lens-based presbyopia correction. Future iterations of the Light Adjustable Lens may become the standard of care.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
Most important is for the patient to demonstrate enthusiasm for presbyopia correction. I never try to convince someone of the value of surgically managing their presbyopia if they show no excitement about the possibility. Some patients are content with their reading glasses.
For patients who express interest in presbyopia correction, I briefly discuss their lifestyle needs, including reading, computer work, sports, and night driving, and inquire about their expectations. At this point, patients also undergo a thorough examination that includes OCT scans of the anterior and posterior segments, topography, tomography, DED and angle kappa assessments, and pupillary measurements. I also recently began using ray tracing to evaluate the dysfunctional lens index; if the number is below 7, I recommend lens-based refractive surgery.
Today, we talk about continuity of care and making decisions that are right for patients throughout their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
Careful identification and management of DED are important before and after presbyopia treatment. My practice offers treatment with intense pulsed light, the LipiFlow Thermal Pulsation System (Johnson & Johnson Vision), and mechanical exfoliation. My staff and I are on the alert for patients’ reports of DED after surgery.
Patients who experience dysphotopsias postoperatively receive reassurance that the phenomenon is normal and should become less noticeable in time. Macular OCT may be required in some instances to rule out cystoid macular edema.
Postoperative management may involve more frequent visits over a longer period than after conventional cataract or LVC surgery. Satisfied patients, however, tend to refer their friends and relatives for presbyopia correction.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
No. It’s not available in the Middle East, where I practice.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
More than 50% of my cataract surgery patients receive trifocal IOLs, and both they and I are highly satisfied with their outcomes. The key for success is properly assessing patients’ preoperative quality of vision and setting realistic expectations. Trifocality presents a compromise; it’s important for patients to understand what they can expect to lose and gain. An objective preoperative assessment of quality of vision that includes a measurement of scatter is crucial to the decision to proceed with trifocal IOLs.
My colleagues and I found that the objective scatter index after trifocal lens implantation is around 1.5.1 Cataract patients usually have an objective scatter index that is greater than 1, so they are typically satisfied with a trifocal IOL. Patients undergoing RLE have clear crystalline lenses and high refractive errors. It’s important to calculate the risk-benefit ratio of trifocal IOL implantation. They must understand that some quality of vision is sacrificed to reduce their spectacle dependence. Other factors in surgical success include accurate IOL calculations; an emmetropic target; the correction of corneal astigmatism (toric trifocal IOL); and a preoperative assessment of angles alpha and kappa, corneal aberrations, posterior vitreous detachment, and macular function. Significant DED is a contraindication for trifocal IOLs.
What are your thoughts on light adjustable lens technology?
It is not yet available where I practice.
What are your thoughts on the use of small-aperture IOLs?
If I had access to this technology, I would use it only for patients with highly aberrated corneas such as those who received a corneal graft.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
When getting started with trifocal IOLs, I recommend selecting presbyopic patients who are hyperopic and have moderate (stage 2) cataracts because they already have a compromised quality of vision. These individuals tend to reap the greatest benefits from surgery—improved quality of vision, reduced ametropia, and greater spectacle independence. Once you have experience with trifocal IOLs and are achieving good results, extend your selection criteria to include more patients. Don’t neglect to perform an objective evaluation of every prospective patient’s preoperative quality of vision (Figure).
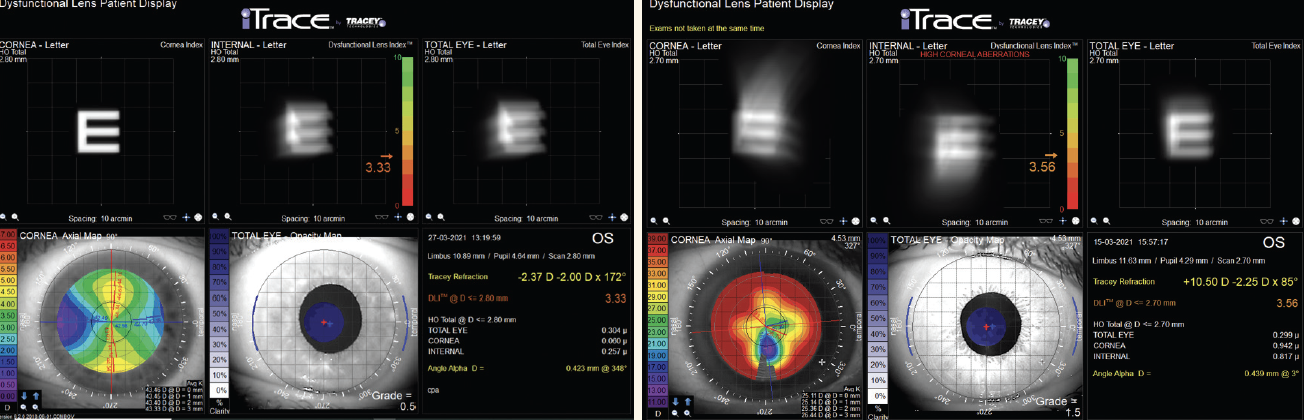
Figure. The dysfunctional lens display on the iTrace (Tracey Technologies).
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I usually offer femtosecond LASIK. My targets are -0.3 ocular spherical aberration OU and a refraction of -0.50 D in the nondominant eye. This strategy has worked well for my patients between 45 and 55 years of age. I consider phakic IOLs to be a better solution than LVC for patients on the cusp of presbyopia who have high refractive errors.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
I think that lens-based solutions are superior to corneal approaches for presbyopia correction. I consider trifocal IOLs to be the most effective option currently and expect that to remain true until a true accommodating IOL is developed. I am nevertheless paying close attention to the early results with allograft inlays and look forward to the release of complete clinical trial data.
What other future treatments have promise?
Presbyopia-correcting phakic IOLs are of great interest to me. Early reports with the EVO+ ICL (STAAR Surgical) from colleagues who have access to the technology have been promising. I look forward to its availability where I practice.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
Choosing the best form of presbyopia treatment for a given patient depends on several factors: presbyopia severity; the patient’s age; refractive error; uncorrected and corrected distance visual acuity; overall quality of vision, which should be analyzed thoroughly to differentiate between corneal and internal (mainly lenticular) aberrations; ocular anatomy, including angles kappa and alpha; pupillary diameter; patient expectations and needs; and lens clarity.
Most patients with presbyopia and lenticular opacities can benefit from trifocal IOLs unless there is a contraindication. Individuals with clear lenses and hyperopia are also usually good candidates for a trifocal IOL. Patients with low myopia tend to be the most difficult to satisfy because they usually have satisfactory uncorrected near and intermediate vision and use spectacles only for distance. It may be wisest not to offer surgical intervention to them unless they are highly motivated. Patients with high myopia, however, who use far and near adds may be good candidates for a trifocal IOL. Posterior vitreous detachment and macular function should be assessed preoperatively.
I generally do not offer refractive surgery to patients with emmetropic presbyopia and clear lenses because they usually lose quality of vision after this procedure.
I reserve LVC for patients with low to moderate myopia who are using far and near adds—especially individuals with compound myopic astigmatism—because they do not have satisfactory uncorrected near visual acuity. In this situation, I target -0.30 µm spherical aberration using a mini-monovision strategy.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
The way to retain patients is to offer them the best possible solutions over the course of their lifetime—solutions that address their current needs without compromising their future choices. During the refractive surgery consultation, it is important to bear in mind a patient’s future needs for presbyopia correction and, most likely, cataract surgery. Treatments that can induce significant corneal aberrations such as LVC for high refractive errors may eliminate a patient’s future candidacy for a multifocal or accommodating IOL. Posterior chamber phakic IOLs can be an excellent option that preserves the cornea.
After 30 years of refractive surgery practice, I am delighted when a patient in whom I implanted an ICL decades ago returns for a solution to nuclear sclerosis and presbyopia. Removing the ICL and implanting a trifocal IOL can deliver an excellent outcome.
1. Eldanasoury A, Tolees S, Bains HS. Clinical outcomes after phacoemulsification with implantation of trifocal and toric trifocal intraocular lenses. J Refract Surg. 2021;37(6):372-379.
Dr. Shultz: I think duration of action is going to be a major differentiator between what is available now and other formulations coming to market. Patients don’t want to carry bottles around with them, and they don’t want to go from seeing well to suddenly not seeing well and having to instill another drop.
Dr. McCabe: I think there will be circumstances for which patients want a shorter duration of action. Maybe they have something to do at night but otherwise prefer to avoid a dimming effect.
Dr. Shultz: That’s a great observation. Some of the friends and family members to whom I’ve prescribed the drops and whom I see regularly have experienced and not felt comfortable with the dimming effect. Others, including me, notice the dimming effect when we first instill the drops, but then the effect seems to go away. I think my brain kind of adapts. Another factor when I’m driving at night is that my car has a big windshield that makes it easier for me to know where I am despite dim vision. License plates and street signs, however, aren’t sharp. Despite the dimming effect, everything else is so much clearer, and I am reminded of the early days after my LASIK procedure.
LENS OPTIONS
Dr. McCabe: Let’s discuss lens options. Many patients with presbyopia are good candidates for IOL surgery. Our colleagues in Europe have many more IOLs to choose from than we do here in the United States, but we can always look to see what we may have in the future. Lens options are growing, and we have an array of choices in the United States. What are your current go-to IOLs for healthy patients with presbyopia who really want an expanded range of vision?
Dr. Shultz: I consider multiple factors when I’m treating a patient with presbyopia. I want to know about their near work. Do they hold objects to read close or at arm’s length? Are they looking at their phones, tablets, and computers primarily, or do they sit and read print materials?
Dr. McCabe: Do your patients complete a questionnaire before speaking with you and your staff, or are these questions just part of the consultation?
Dr. Shultz: My practice uses Veracity Surgical (Carl Zeiss Meditec), which has a built-in questionnaire. The answers that patients provide serve as a starting point for discussion.
Questionnaires are helpful for identifying what patients care about. Are they concerned about experiencing glare and halos after surgery? Is clear distance vision a priority, or is a full range of vision important? There are, however, downsides to questionnaires. One is that they can’t demonstrate where patients hold reading material. I want them to show me. Another is that a questionnaire doesn’t provide all the information about a patient’s ocular anatomy and visual pathway that I want.
I use the iTrace (Tracey Technologies) to measure angle alpha-D, which is basically the difference between the patient’s line of sight and the center of the eye. It helps me determine where an IOL will be located after surgery. Before I began using the iTrace, I would place the IOL where I thought the patient’s line of sight was after asking them to look at the microscope light. I found that IOLs were not always in the correct spot after surgery. Some became decentered, so the patient was not looking through the center of the lens. Incorporating angle alpha-D into my surgical decision-making process helps me to avoid unhappy postoperative patients.
Dr. McCabe: Let’s say a patient has an active lifestyle and healthy eyes, likes to hold things close, and desires a full range of vision. Their line of sight and the center of their eye line up perfectly on their preoperative assessment. What’s your go-to technology?
Dr. Shultz: I would implant a Tecnis Symfony OptiBlue IOL (Johnson & Johnson Vision) in the patient’s dominant eye. It is an improvement on the previous model of the lens that has eliminated the complaints I received from some patients about glare, halos, and spiderwebs. Changes to the haptics have improved the rotational stability of the IOL.
One thing I like about the Symfony relative to trifocal IOLs, which I also offer, is that patients experience minimal loss of contrast sensitivity. They have good night vision with the Symfony. These are issues I discuss with patients preoperatively, and I tend to steer patients who frequently drive at night away from trifocal IOLs. I find that the Symfony works well for patients who like to hold objects close (14 inches). Most of my patients are happy with the range of vision that they achieve with the Symfony. If they do not achieve the range they are seeking, then I choose a different IOL for their nondominant eye. I usually choose a medium-add Tecnis Multifocal IOL (Johnson & Johnson Vision), but I also consider a Tecnis Synergy (Johnson & Johnson Vision). My one concern with the latter is its tight landing zone. The Synergy is unforgiving of residual refractive error. When I am implanting it in the nondominant eye, however, I can use the experience with the patient’s dominant eye to fine-tune the surgical plan. I can account for effective lens position more accurately. I also prefer to implant the same IOL platform in a patient.
Dr. McCabe: Do you ever offset the Symfony a little bit to give a patient a little more near vision?
Dr. Shultz: If the patient is generally happy, I don’t want too much of an offset (-0.25 to -0.50 D) in the nondominant eye.
Dr. Zhu: I have two go-to presbyopia-correcting IOLs, the Clareon PanOptix and the Clareon Vivity (both from Alcon). I mix and match in most of my patients. I prefer to implant the PanOptix in the nondominant eye and the Vivity in the dominant eye. The rest of my patients receive either the PanOptix or the Vivity bilaterally depending on their visual needs at distance and nighttime.

PHARMACOLOGIC AGENTS
Where do you expect drops to fit into your treatment paradigm for presbyopia correction once they are available in your country?
It is too early to say where presbyopia drops will fit into my treatment paradigm. In the future, drops may be an option I consider for patients who are not good candidates for surgical correction or when I recommend delaying surgery.
How will the market change when other drops become available?
It is reasonable to think that the price of the drops will decrease and treatment will become more cost-effective.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
I do not like to use adjectives such as excellent because of their subjective meaning. For instance, 20/25 VA might be rated excellent by a patient who underwent surgery to remove and replace a dense cataract but poor by someone who underwent RLE. I prefer to talk about the percentage of patients who achieve spectacle independence at all distances or who are satisfied with their UCVA. From this perspective, current evidence shows that trifocal IOLs deliver the highest rate of spectacle independence at all distances.1-4 For this reason, they are my primary offering for presbyopia correction. In several studies, when emmetropia was targeted in both eyes, spectacle independence was achieved by around 60% and 90% of patients who received EDOF and trifocal IOLs, respectively.5-9 Contrary to what is commonly believed, higher rates of spectacle independence have not been reported when a mini-monovision strategy with EDOF IOLs was implemented.10-12
What are your thoughts on light adjustable lens technology?
I do not have experience with the Light Adjustable Lens, but I find it an interesting alternative to explore for individuals in whom the accuracy of IOL calculations could be a concern. In my experience, however, this is a small number of patients.
What are your thoughts on the use of small-aperture IOLs?
I have implanted a few of these lenses in healthy patients. The small-aperture IC-8 Apthera was placed in the nondominant eye, and a monofocal IOL was placed in the dominant eye. I found this strategy to offer greater distance vision and to be associated with a lower incidence of dysphotopsias than EDOF lenses—particularly those with diffractive designs—using a mini-monovision strategy. Patients, however, may have less functional near vision and more difficulty seeing in dim lighting with a small-aperture IOL than with other EDOF IOLs.12,13
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
Based on published studies, patient satisfaction with presbyopia-correcting IOLs is high. Around 90% of patients are satisfied or very satisfied with these lenses.14-17 Additionally, dissatisfaction is generally low, at less than 10%.17-19 In other words, when proper selection criteria are used, the risk of postoperative dissatisfaction seems to be similar with presbyopia-correcting and monofocal IOLs. A dissatisfaction rate that is higher than 6% might suggest problems with the selection criteria or with the surgery itself.17-19
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I favor Presbyond Laser Blended Vision with the MEL 90 excimer laser (Carl Zeiss Meditec) for individuals with presbyopia who are younger than 45 years of age and have functioning crystalline lenses. For patients who are between 45 and 50 years of age, I take nuclear sclerosis and axial length into consideration when deciding between LVC and RLE. When patients are 50 to 60 years old, LVC is a short-term solution at best for presbyopia, so I recommend RLE instead if the axial length is less than 23 mm. If the axial length is greater than 23 mm, I am more cautious about offering RLE because of an increased risk of retinal detachment.20 I may advise these patients to use multifocal contact lenses or progressive spectacles until they progress to cataract surgery.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
The main advantage of inlays is that corneal tissue is preserved for future surgery. The safety and accuracy reported with the first allogenic devices was lower than with LVC, their main competitor. Research on the safety and accuracy of allograft and allogenic inlays is therefore required before they become widely used to correct presbyopia.
What other future treatments have promise?
With proper patient selection and careful surgical technique, we have many good options for correcting presbyopia. New alternatives for simultaneous vision will become available in the near term, but I do not expect them to represent major advances compared to available technologies. Surgeons therefore should not wait for the perfect solution for presbyopia correction such as an accommodating IOL that behaves exactly like the crystalline lens. Now is the time to learn to use available alternatives optimally.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
My colleagues and I have conducted several studies on how to identify candidates for a multifocal IOL.21-26 The patient’s age and grade of nuclear sclerosis are the two main determinants of which presbyopia treatment to recommend. At ESCRS 2022, we will show that understanding grading systems such as the objective scatter index and the dysfunctional lens index can help surgeons to identify which patients are at increased risk of experiencing an unacceptable reduction in contrast sensitivity or bothersome postoperative dysphotopsias with a presbyopia-correcting IOL.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
Optimizing the patient experience requires involving patients in treatment decisions and planning care that takes their future needs into account. For example, long-term studies of several multifocal IOLs indicate the median time until recipients require an Nd:YAG laser capsulotomy. Surgeons can use this information to advise patients when they may experience a decrease in vision and inform them that technology is available to address the issue. If surgical intervention is not currently advisable, thoroughly educating patients on the reasons and offering options such as multifocal contact lenses and progressive spectacles in the interim can demonstrate the physicians’ commitment to providing a lifetime of eye care.
1. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48(2):136-143.
2. Webers VSC, Bauer NJC, Saelens IEY, et al. Comparison of the intermediate distance of a trifocal IOL with an extended depth-of-focus IOL: results of a prospective randomized trial. J Cataract Refract Surg. 2020;46(2):193-203.
3. Jonker SMR, Bauer NJC, Makhotkina NY, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Comparison of a trifocal intraocular lens with a +3.0 D bifocal IOL: results of a prospective randomized clinical trial. J Cataract Refract Surg. 2015;41(8):1631-1640.
4. Law EM, Aggarwal RK, Buckhurst H, et al. Visual function and subjective perception of vision after bilateral implantation of monofocal and multifocal IOLs: a randomized controlled trial. J Cataract Refract Surg. 2020;46(7):1020-1029.
5. Reinhard T, Maier P, Böhringer D, et al. Comparison of two extended depth of focus intraocular lenses with a monofocal lens: a multi-centre randomised trial. Graefes Arch Clin Exp Ophthalmol. 2021;259(2):431-442.
6. Ferreira TB, Ribeiro FJ, Silva D, Matos AC, Gaspar S, Almeida S. Comparison of refractive and visual outcomes of 3 presbyopia-correcting intraocular lenses. J Cataract Refract Surg. 2022;48(3):280-287.
7. Darian-Smith E, Versace P. Visual performance and positional stability of a capsulorhexis-fixated extended depth-of-focus intraocular lens. J Cataract Refract Surg. 2020;46(2):179-187.
8. Liu X, Song X, Wang W, et al. Comparison of the clinical outcomes between echelette extended range of vision and diffractive bifocal intraocular lenses. J Ophthalmol. 2019;2019:5815040.
9. Farvardin M, Johari M, Attarzade A, Rahat F, Farvardin R, Farvardin Z. Comparison between bilateral implantation of a trifocal intraocular lens (Alcon Acrysof IQ PanOptix) and extended depth of focus lens (Tecnis Symfony ZXR00 lens). Int Ophthalmol. 2021;41(2):567-573.
10. Hovanesian JA, Jones M, Allen Q. The Vivity extended range of vision IOL vs the PanOptix trifocal, ReStor 2.5 Active Focus and ReStor 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle independence. Clin Ophthalmol Auckl N Z. 2022;16:145-152.
11. Newsom TH, Potvin R. Evaluation of quality of vision and visual outcomes with bilateral implantation of a non-diffractive extended vision intraocular lens with a target of slight myopia in the non-dominant eye. Clin Ophthalmol Auckl N Z. 2022;16:183-190.
12. Schojai M, Schultz T, Jerke C, Böcker J, Dick HB. Visual performance comparison of 2 extended depth-of-focus intraocular lenses. J Cataract Refract Surg. 2020;46(3):388-393.
13. Ang RE, Picache GCS, Rivera MCR, Lopez LRL, Cruz EM. A comparative evaluation of visual, refractive, and patient-reported outcomes of three extended depth of focus (EDOF) intraocular lenses. Clin Ophthalmol Auckl N Z. 2020;14:2339-2351.
14. Nicula CA, Popescu R, Rednik AM, Nicula D, Bulboaca AE, Stanescu I. Refractive lens exchange in hyperopic presbyopes with the Acrysof IQ Panoptix intraocular lens: one-year results and analysis of the literature. Ther Clin Risk Manag. 2020;16:1125-1137.
15. Sinha R, Sahay P, Saxena R, Kalra N, Gupta V, Titiyal J. Visual outcomes of binocular implantation of a new extended depth of focus intraocular lens. Indian J Ophthalmol. 2020;68(10):2111.
16. Ruiz-Mesa R, Abengózar-Vela A, Aramburu A, Ruiz-Santos M. Comparison of visual outcomes after bilateral implantation of extended range of vision and trifocal intraocular lenses. Eur J Ophthalmol. 2017;27(4):460-465.
17. Schallhorn SC, Teenan D, Venter JA, Hannan SJ, Schallhorn JM. Initial clinical outcomes of a new extended depth of focus intraocular lens. J Refract Surg. 2019;35(7):426-433.
18. Ribeiro FJ, Ferreira TB, Silva D, Matos AC, Gaspar S. Visual outcomes and patient satisfaction after implantation of a presbyopia-correcting intraocular lens that combines EDOF and multifocal profiles. J Cataract Refract Surg. 2021;47(11)1448-1453.
19. Fernández J, Rodríguez-Vallejo M, Martínez J, Tauste A, Piñero DP. Standard clinical outcomes with a new low addition trifocal intraocular lens. J Refract Surg. 2019;35(4):214-221.
20. Qureshi MH, Steel DHW. Retinal detachment following cataract phacoemulsification—a review of the literature. Eye. 2020;34(4):616-631.
21. Fernández J, Burguera N, Rocha-de-Lossada C, Martin FZ, Rodríguez-Vallejo M. A new approach for detecting patients complaining of dysphotopsia after multifocal intraocular lens implantation due to non-optical reasons. Paper presented at: 26th ESCRS Winter Meeting; February 18-20, 2022; Virtual.
22. Fernández J, Rodríguez-Vallejo M, Martínez J, Tauste A, Piñero DP. Biometric factors associated with the visual performance of a high addition multifocal intraocular lens. Curr Eye Res. 2018;43(8):998-1005.
23. Fernández J, Rodríguez-Vallejo M, Martínez J, Tauste A, Piñero DP. From presbyopia to cataracts: a critical review on dysfunctional lens syndrome. J Ophthalmol. 2018;2018:1-10.
24. Fernández J, Rodríguez-Vallejo M, Martínez J, Burguera N, Piñero DP. Pupil dependence assessment with multifocal intraocular lenses through visual acuity and contrast sensitivity defocus curves. Eur J Ophthalmol. 2020:112067212094020.
25. Fernández J, Rodríguez-Vallejo M, Martínez J, Burguera N, Piñero DP. Pupil diameter in patients with multifocal intraocular lenses. J Refract Surg. 2020;36(11):750-756.
26. Fernández J, Rodríguez-Vallejo M, Burguera N, Rocha-de-Lossada C, Piñero DP. Spherical aberration for expanding the depth of focus: a review for the anterior segment surgeon. J Cataract Refr Surg. 2021;47(12):1587-1595.
Dr. McCabe: Do you find that the issue of glare and halos at night or the possibility of dysphotopias is a driving factor for the use of the Vivity versus a trifocal IOL like the PanOptix? Is it sometimes early pathology within the eye, or is it both?
Dr. Zhu: It’s both. Vivity has filled a tremendous gap. It is a great lens for patients who desire presbyopia correction but are not good candidates for a trifocal IOL because objectively they have mild pathology or they don’t tolerate the halos and glare because they do a lot of nighttime driving, like truck drivers.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
Vuity is not yet available in Australia, but we expect to have access to the product within the year. I already have patients asking me about it.
Where do you expect drops to fit into your treatment paradigm for presbyopia correction once they are available in your country?
Most patients who come to see me ask for a solution to their presbyopia. I pride myself on being able to restore the range of vision they desire. There is a group of patients, however, for whom RLE and keratorefractive procedures would not be safe or ideal. These individuals typically have early presbyopia. I therefore do not expect presbyopia drops to affect my surgical candidates but rather to provide an option for patients whom I currently ask to wait until their presbyopia progresses.
Who are the most appropriate patients for presbyopia drops?
I expect the ideal candidate to have early presbyopia and retain some accommodative ability. Treatment with presbyopia drops may allow them to delay or reduce their need for reading glasses. Historically, pilocarpine use has raised concerns about retinal tears and inflammation,1,2 so the ideal candidate does not have risk factors for either of these conditions.
How will the market change when other drops become available?
As an ophthalmologist who specializes in the surgical management of presbyopia, I have thought a lot about this question. I expect my optometric colleagues to be the major prescribers of these drops when the products become available because they are generally the first providers contacted by patients with early presbyopia. This may mean that some patients will wait longer to see me about surgical solutions, but they will visit my office eventually. Perhaps the most interesting change will be if patients present with a better understanding of depth of focus, loss of accommodation, and the side effects of pinhole optics such as nighttime vision problems. That would make discussing the pros and cons of various presbyopia-correcting IOL designs easier.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
I am fortunate to have access to many different presbyopia-correcting IOLs, all of which have pros and cons. I have three go-to IOLs. The first is the AcrySof IQ Vivity (Alcon) extended range of vision IOL, which I find provides patients with very good distance and intermediate vision and at least functional reading vision. About 70% of my patients who receive the Vivity lens can read well, but I cannot predict preoperatively which patients will be a part of this subgroup. The first eye is therefore targeted for emmetropia. A week later, the patient returns to the clinic to discuss whether to target the same refraction or slight myopia in the second eye. I find this strategy works well, even if it decreases clinic efficiency. The lens has a low side effect profile, so postoperative glare or halos are of minimal concern.
My second go-to option is a trifocal IOL. I prefer the AT LISA tri (Carl Zeiss Meditec) or the AcrySof IQ PanOptix (Alcon), and I also have had great outcomes with the FineVision trifocal (BVI Medical). I find that these IOLs provide excellent vision quality. I sometimes favor the PanOptix for its hydrophobic lens material and C-loop haptic design. One of my concerns about trifocal IOL technology, however, is that DED can negatively affect vision quality and can be difficult to resolve.3 My other concern is potential difficulty with night vision; about 30% of my patients who received a trifocal IOL reported avoiding driving at night after surgery, which is a major life change.
My third go-to presbyopia-correcting IOL is the IC-8 Apthera. I favor the small-aperture IOL as a therapeutic option for eyes with irregular corneas, and I share more about my experience with the IC-8 Apthera IOL below.
What are your thoughts on light adjustable lens technology?
I have not implanted the Light Adjustable Lens. The ability to fine-tune correction postoperatively, however, interests me because I feel we are close to the limits of what we can achieve with preoperative data. I think a true game-changing technology will allow adjustments such as adding or removing sphere, cylinder, and multifocality to be made postoperatively to any IOL. We will see this with laser-adjustable IOLs in the near future.
What are your thoughts on the use of small-aperture IOLs?
I have been implanting the IC-8 Apthera routinely in eyes with irregular corneas for the past 3 years (click here for a case example). The lens can provide these patients with a quality of vision that was previously possible to achieve only with rigid contact lenses. I find that individuals with a history of RK do particularly well with the IC-8 Apthera. In my experience, the lens functions well in eyes with up to about 2.00 D of astigmatism, but a lot of these patients have a greater amount of astigmatism. I therefore hope that a toric model becomes available soon.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLS?
No. 1: Obtain high-quality biometry measurements. Residual refractive error is the enemy of presbyopia correction, and rubbish in equals rubbish out.
No. 2: Manage the signs and symptoms of DED and start the process preoperatively. An unhealthy ocular surface degrades vision to a much greater extent with a presbyopia-correcting IOL compared to a monofocal IOL.
No. 3: Discuss side effects such as halos and glare with patients before surgery. Part of this pointer is also setting reasonable expectations.
No. 4: Implant a toric IOL if indicated. Even a small amount of residual astigmatism can reduce patient satisfaction.
No. 5: Start with ideal candidates. I recommend beginning with patients who have low hyperopia and presbyopia because they generally appreciate an improvement in vision even if they experience dysphotopsias. Avoid patients with low myopia at the outset because they can be hard to please.
No. 6: If a patient is dissatisfied after surgery, don’t send them to their optometrist. The best things you can do in this situation are to discuss neural adaptation with them, optimize the health of the ocular surface, assess the posterior capsule for opacity, and consider offering a laser enhancement or IOL rotation or exchange if necessary.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I do not currently create multifocal corneas. I perform LASIK, SMILE, and PRK but use a monovision strategy only rarely. In my opinion, if a patient is old enough to consider targeting myopia in only one eye, then changes in the crystalline lens are likely to occur soon that alter their refraction and lead to disappointment. I prefer to offer presbyopia-correcting IOLs and RLE. Perhaps the approval of hyperopic SMILE will change my view.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
I like the idea of being able to adjust a patient’s refractive error without removing tissue. Results with allogenic intrastromal corneal ring segments have been promising for managing keratoconus,4 which suggests that the technology may be suited to treating other refractive errors. Inlay procedures, however, are not as quick or simple as lens surgery or LVC, so it may take time for the technology’s use to become routine.
What other future treatments have promise?
The ability of CXL to treat refractive error accurately would be wonderful. A greater understanding of how to measure corneal biomechanics is required for this application of CXL to be accepted and widely adopted. Additionally, a true accommodating IOL would hold great potential. Many approaches are being tested; they differ in terms of how the IOL senses the requirement to adjust and how it changes refractive power.
Perhaps the most futuristic technology but one with some biologic plausibility is eye drops to stop and even reverse cataract formation (click here for more on this topic). Whether accommodation can be restored is another question. If, however, the crystalline lens can remain flexible for longer, then presbyopia could be delayed.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
The best tools I have are the time I spend with patients and my relationships with referring optometrists. During the assessment, I seek to understand what patients like doing, what their priorities are, and what trade-offs they are willing to accept. This has resulted in a high rate of satisfaction after surgery. The main question that guides my recommendation of an extended range of vision or trifocal IOL is whether the patient frequently drives at night. If they do, I typically recommend an extended range of vision IOL.
I also spend time educating my referring optometrists about IOL options so they can begin educating patients before they meet me. Optometrists have usually known the patients for years and understand their patients’ lifestyle and needs. I often receive referral letters specifying which IOL type the patient prefers. Sometimes I disagree, but knowing the reason for the recommendation is helpful nevertheless.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
From the start, I explain to patients that eye care is a team effort. I will perform their surgery and do everything I can to give them the outcome they want. They all know that they will return to their optometrist for ongoing health checks. That said, I make clear to patients that they may return to see me and contact me directly whenever they want.
If I see a patient with presbyopia who is not yet ready for surgery, I explain that I have their information and will be ready with a plan when needed. I then return them to the care of their referring optometrist.
The most important thing to me is that the patient is happy. Happy patients return and are confident I can solve their problems. Sometimes, satisfying patients requires absorbing the cost of laser enhancements, multiple extra clinic visits, and communication in the forms of text messages, emails, and phone calls. This goes a long way toward building a trusting relationship.
1. Al-Khersan H, Flynn Jr HW, Townsend JH. Retinal detachments associated with topical pilocarpine use for presbyopia: pilocarpine-associated retinal detachments. Am J Ophthalmol. 2022;242:52-55.
2. Benozzi J, Benozzi G, Orman B. Presbyopia: a new potential pharmacological treatment. Medical Hypothesis. Discovery and Innovation in Ophthalmology. 2012;1(1):3.
3. Llovet-Rausell A, Llovet-Osuna F, Bilbao-Calabuig R, Del Pozo MM, Ortega-Usobiaga J, Baviera-Sabater J. Visual outcomes, spectacle independence and satisfaction after diffractive trifocal intraocular lens implantation. Archivos de la Sociedad Española de Oftalmología (English Edition). 2018;93(10):481-490.
4. Jacob S, Patel SR, Agarwal A, Ramalingam A, Saijimol AI, Raj JM. Corneal allogenic intrastromal ring segments (CAIRS) combined with corneal cross-linking for keratoconus. J Refract Surg. 2018;34(5):296-303.
In the past, I would have done monovision with monofocal lenses in these patients. Now, I implant the Vivity and either target plano or use a mini-monovision strategy to give them a little more near vision.
Combining the Vivity with the PanOptix can give patients the best of both worlds. In my practice, patient satisfaction with this strategy is greater than 90%. Most patients achieve spectacle independence, including at near. This mix-and-match strategy provides just enough near vision, and most patients don’t notice any dysphotopias at night, which is better than what I’ve seen with bilateral PanOptix IOLs.
Dr. Shafer: I’m very interested in everything you said, Dr. Zhu. It could influence what I do in my practice. I have shifted away from diffractive IOL technologies over the past few months. I practice in an affluent area outside of Philadelphia, and many of my patients who received diffractive lenses complain of dysphotopias. Most of them adapt, however.
I’ve been getting a lot of mileage out of the Vivity lately, and it’s become my go-to presbyopia-correcting lens even though it does not always provide patients with complete spectacle independence. I like knowing that, even if patients develop subtle maculopathy, the Vivity can continue to provide most of its benefits unlike a diffractive lens.
In patients with low myopia, I will occasionally target -1.00 D bilaterally with the Vivity. This usually gives patients about 20/40 VA at distance and J1 at near. These patients are extremely happy, which helped convince me to shift my focus to near vision more than distance.
Dr. McCabe: That’s an interesting strategy. I would consider, however, targeting closer to plano in the patient’s dominant eye. Dr. Talley Rostov, what are your preferred IOL choices, and how do you decide what to offer patients?
Dr. Talley Rostov: I use a number of IOLs, and I like to match the technology to each patient. For example, I pay close attention to the higher-order aberrations (HOAs). Patients with significant HOAs are not good candidates for a multifocal IOL. I would consider putting a Vivity in those patients and using a mini-monovision strategy targeting -0.25 D in the dominant eye and -0.50 D in the nondominant eye. If the HOAs are minimal, I implant either a PanOptix or a Tecnis Synergy IOL. I find that patients are more likely to notice glare and halos with the Synergy but that it gives a little more pop at near than the PanOptix does.
Having a discussion with the patient to discover what they want and need is crucial to selecting the right IOL. For example, I have treated a few lawyers who wanted more pop at near, but they understood that they would have glare and halos at night. For these patients, spectacle independence was more important.
I also use the Light Adjustable Lens (RxSight) for patients who previously underwent LASIK or radial keratotomy (RK). Again, I target a little bit of mini-monovision. Patients are very happy with a Light Adjustable Lens because it extends their depth of focus.
Like Dr. Zhu, I also mix and match the PanOptix in one eye with the Vivity in the other. I use all the different technologies, and I try to match the technology to the patient’s needs.
Dr. McCabe: I love that we have so many lens choices. We can assess the patient’s residual refractive needs after surgery in their first eye and fill in the blank, so to speak, with another technology in the fellow eye.
Dr. Slade: That’s really become our job, hasn’t it—to figure out which lens is best for each patient? I am excited about the results I’ve seen with the PanOptix, and right now it is my favored IOL. Previously, I used a lot of Vivity IOLs, but my explant rate was too high. My second go-to IOL is the Light Adjustable Lens.
The one wish I have is for a better IOL for patients with compromised and complex corneas. The Tecnis Symfony (Johnson & Johnson Vision) has been pretty good for that. The company is coming out with a new model of the lens.
Dr. McCabe: The Light Adjustable Lens has been a game-changer, especially when we can’t obtain accurate biometry measurements preoperatively or when patients have a history of complicated corneal surgery such as RK. I’ve been impressed with the range of near vision patients get while they refract to very little myopia, and the Light Adjustable Lens helps extend their depth of focus. A lot of work, however, goes into the postoperative process to fine-tune the result and walk the patient through the process.
Dr. Shultz: I’ve been very happy with the Light Adjustable Lens, and I’ve gotten more comfortable with the technology since RxSight added ActivShield. With the previous model of the lens, some late changes occurred. Since the addition of ActivShield, I can tell patients they don’t have to wear UV glasses indoors, just outdoors.
I regularly use the Light Adjustable Lens in several situations. I find it to be an excellent option for patients who have a successful history with monovision. The Light Adjustable Lens permits testing of different refractive targets. I also find the lens to be excellent for patients who have a history of refractive surgery because the technology allows me to optimize postoperative refractive accuracy. Additionally, I have had great success with the Light Adjustable Lens in patients who have a history of arcuate keratotomy and RK as well as those who underwent LASIK. The lens is also a useful option for patients who desire presbyopia correction but want to avoid optical aberrations at night. The center of the lens is steepened to provide slight multifocality and increase patients’ range of vision, and we can play with a little mini-monovision to achieve a broader range of vision.
Dr. McCabe: Dr. Talley Rostov, where will the IC-8 Apthera IOL will fit into your practice?
Dr. Talley Rostov: I’m super excited about the IC-8 Apthera for patients with previous RK. I have a large, thriving cornea practice, and many of my patients with aberrated corneas could benefit from the technology.
Dr. Zhu: I agree with you, Dr. Talley Rostov. Now that the IC-8 Apthera is available in the United States, I am going to start with aberrated corneas—post-RK patients and those with keratoconus and corneal scars. There are a lot of good data from our colleagues overseas showing a significant improvement in BCVA after implantation of the IC-8 Apthera lens because it decreases HOAs. It also improves the image quality in eyes with aberrated corneas and extends depth of focus. This is an exciting way for us to offer these patients presbyopia correction that we otherwise could not achieve except with full monovision. I have heard that patients can experience some dimness if the IC-8 Apthera is implanted in both eyes, so that is one thing that I’m going to counsel my patients on. Alternatively, perhaps I will implant the IOL only in the nondominant eye and use a mini-monovision strategy with a regular monofocal IOL in the dominant eye.


PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
We do not use pharmacologic treatments.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
To correct a patient’s vision at all distances, we implant a trifocal IOL (FineVision). If dysphotopsias or loss of contrast sensitivity is of great concern, we offer the Lucidis (Swiss Advanced Vision), which is an EDOF lens with an atypical (pseudo-nondiffractive) profile that provides distance and intermediate vision and some near vision. Both IOLs are available in toric models, and we find that their unpolished surfaces provide good stability.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
A thorough history that documents the patient’s needs and visual habits is necessary to identify and propose the most suitable solution. Achieving the best possible results requires precisely analyzing all the ocular data and optimizing the health of the ocular surface. Correcting presbyopia without also correcting astigmatism should be unthinkable.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
We perform hyperopic presbyopic or myopic presbyopic LVC with Q-factor modulation and additive mini-monovision for patients who are less than 55 years old. Q-factor is a mathematical descriptor designed to qualify the asphericity of the corneal surface. It seems to us, however, that RLE is the best way to correct presbyopia for patients who are above the age of 55.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
Each of our patients completes a questionnaire on their visual habits. Graphs are created from the responses that indicate how much time the patient spends using each range of vision. An IOL type is recommended based on the survey results, the patient’s history, and their economic situation.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
If a patient experiences a decrease in near vision or develops a cataract after presbyopic LVC, RLE with a multifocal or EDOF IOL can be performed depending on their residual refractive error or corneal aberrations.
Dr. Shultz: Several of my patients have been waiting for this lens. One who couldn’t wait recently traveled to Europe for the surgery. She has irregular corneas due to RK. She received an IC-8 Apthera in one eye and a Light Adjustable Lens in the contralateral eye. I’ve been monitoring the patient and am impressed with the results. It’s amazing how effectively the IC-8 Apthera has reduced her optical aberrations, and it has extended her depth of focus.
I often see patients who have irregular corneas, so I expect the technology to have a place in my practice.
Dr. McCabe: Did the patient you describe notice the dimming of vision in the eye with the IC-8 Apthera that Dr. Zhu referenced?
Dr. Shultz: It is too early to tell. I am in the process of performing the light adjustments of the Light Adjustable Lens, so she currently sees better with the eye that received the IC-8 Apthera. She understood preoperatively that her options were limited and that nothing would give her perfect vision. Her goals were to be able to drive and not to wear contact lenses. The patient is happy with the dramatic reduction in her astigmatism.
Dr. McCabe: One of the interesting things to me is that the IC-8 Apthera has a lot of refractive forgiveness—up to 1.00 D of refractive error and 1.25 D of astigmatism on either side of plano—while somewhat increasing depth of focus with a little myopic offset. I think there is no better solution for patients who have a moving refractive target throughout the day, such as post-RK patients, for example.
Dr. Zhu: The flexible landing zone is even larger. According to results from our colleagues overseas, the IC-8 Apthera IOL can tolerate up to 1.50 D of cylinder. That is pretty remarkable. There is no toric version, but you could probably even use it in patients with high cylinder because of that flexibility.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
I have no experience with pharmacologic agents for presbyopia correction.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
My current go-to IOLs are trifocal and EDOF IOLs. For many years, the FineVision trifocal IOL was my default choice for patients who want a full range of vision. I recently began implanting the RayOne Trifocal IOL (Rayner) and have found that the lens provides my patients with better intermediate vision compared to the FineVision trifocal. In my experience, the FineVision trifocal IOL delivers exceptional near vision at 30 cm but variable intermediate visual results. Additionally, the RayOne Trifocal comes fully preloaded whereas the FineVision does not. Both IOLs are available in a toric model, and I have a low threshold for correcting preexisting astigmatism (≥ 0.75 D of cylinder).
The EDOF category of IOLs, and the Vivity in particular, has been a revelation to me. I was the chief investigator in the United Kingdom for the original trials of the Vivity and have found it highly rewarding to watch the evolution of the technology and its incorporation into clinical practice. The IOL has a favorable side effect profile in terms of glare and halos and behaves essentially like a monofocal lens in this respect. In my experience, patients achieve excellent distance and intermediate vision with the Vivity. Patients generally obtain a full range of vision with an offset of about -1.00 D in the nondominant eye. I find the IOL especially useful for individuals who have a history of refractive surgery, those who wish to avoid experiencing glare and halos after surgery, and those who are not good candidates for a trifocal IOL (eg, patients with ocular surface disease).
I may offer an enhanced monofocal IOL such as the Tecnis Eyhance (Johnson & Johnson Vision) or RayOne EMV (Rayner) to patients who have experience with contact lens monovision and are keen to maintain the visual strategy with which they are familiar. I have found, however, that EDOF lenses work well even for these individuals and can give them a more natural range of vision if distance and intermediate are targeted in the dominant eye and intermediate and near vision in the nondominant eye targeting -1.00 D.
What are your thoughts on light adjustable lens technology?
I have no experience with the Light Adjustable Lens. Modern biometry machines and IOL calculations—and thus surgical outcomes—are more accurate than ever. The chances that a patient will need a refractive enhancement after cataract or RLE surgery are low at my practice, and a touch-up with LVC if needed can be performed safely. To my mind, these considerations outweigh the potential benefits of the light-adjustable technology. My attitude may change in the future if laser technology becomes available that can add, adjust, or remove multifocality from an IOL.
What are your thoughts on the use of small-aperture IOLs?
I have implanted the IC-8 Apthera in a small number of eyes that had a history of RK. I believe that there is a place for the technology, but EDOF IOLs also work well in this population. All of the patients in whom I implanted IC-8 Apthera lenses experienced an improvement in visual acuity but also a reduction in night vision. I have therefore largely shifted to using EDOF IOLs for these patients unless they have marked corneal irregularity.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
The key to success is understanding the technology. A low-risk strategy is to start with enhanced monofocal IOLs such as the Tecnis Eyhance and RayOne EMV because the downside of the technology is minimal. A toric model of the Eyhance is available, which is a big plus. I understand that a toric version of the RayOne EMV should be released in the future.
Once surgeons become comfortable with enhanced monofocal IOLs, they can consider gaining experience with EDOF IOLs. They are available in toric models and can provide patients with good distance and intermediate vision.
When surgeons are comfortable with enhanced monofocal and EDOF IOLs, they can consider implementing trifocal IOL technology while bearing in mind its potential drawbacks.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I offer monovision or blended vision LASIK to patients with presbyopia who have no signs of lenticular opacity. I typically target distance vision in the dominant eye and -1.50 to -2.00 D in the nondominant eye depending on the patient’s age and vision preferences. I chose this strategy for my own eyes and have fared well with it.
I offer presbyopic LASIK to patients who are older than 50 years of age but also discuss with them the option of RLE with either trifocal or EDOF IOLs using a mini-monovision strategy. The choice between LASIK and RLE also depends on the patient’s expectations and ocular status.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
I implanted the Kamra corneal inlay (CorneaGen) many years ago. The technology worked well initially, but many of the inlays had to be removed owing to compatibility issues. Given the other technologies currently available, I feel that there is limited space for inlays. I don’t discount the technology, but I find it hard to envision great market success for any inlay because of the technology’s history and the inherent problems of biocompatibility of foreign material with the cornea.
What other future treatments have promise?
I think it will be hard for cornea-based treatments to compete with the range of vision and favorable side effect profile of current (and future) IOL technology, particularly in the EDOF category. I am not a fan of creating a multifocal cornea with laser technology because the procedure is hard to reverse if a problem arises and quality of vision could be negatively affected if the patient undergoes lens surgery in the future.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
I proceed from least to most invasive, but the decision depends on each patient’s examination findings and expectations. As I mentioned earlier, my patients who are 45 to 50 years old typically undergo presbyopic LASIK unless they are better candidates for RLE. I typically advise these patients to wait until the age of 50. For individuals who are older than 50 years of age, LASIK is still an option, but the scale starts tipping more in favor of RLE in terms of quality of vision and longevity of results, especially as they approach the age of 60. As far as the choice of IOL, it depends on the patient’s expectations, their ocular examination, and whether there is a history of refractive surgery.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
The best way to retain patients is to be honest with them. To young patients with presbyopia, I say, “We can proceed with LASIK now. It will probably buy you 5 to 15 years depending on what happens to your lens in the future. At that time, RLE becomes an option.”
LVC involves less overall risk than intraocular surgery. If patients tolerate a blended vision or monovision strategy, it makes sense to perform LVC initially and reserve more invasive surgery for the future. In my experience, problems can arise from offering laser blended vision to older patients who have presbyopia without discussing the option of RLE because the effects of LVC are unlikely to satisfy them for long. If they become disgruntled, they may seek a different provider for their lens surgery when the time comes. Honesty and transparency in the preoperative discussion of their options make it more likely that these individuals will return to our practice for their eye care needs.
Dr. McCabe: Dr. Shafer, do you have any pointers for surgeons who haven’t begun offering presbyopia-correcting IOLs?
Dr. Shafer: With so many lens options available, it can be overwhelming to consider the pros and cons of each lens design. As I mentioned before, I prefer nondiffractive lenses like the Vivity because they avoid glare and halos. In my experience, this simplifies the patient counseling process. A good place to start for those who don’t have much experience with presbyopia-correcting IOLs is the Light Adjustable Lens. It’s a great option for most patients.
It can be harder to jump into offering diffractive IOL technologies because fine-tuning may be required postoperatively. If your practice does not have access to an excimer laser for enhancements or can’t refer patients to another practice that does, I recommend starting simpler. Start with the Vivity lens and a mini-monovision rather than a full monovision strategy. It’s quite easy and rewarding to get involved with presbyopia-correcting lenses.
Dr. McCabe: Those are good pearls. I would encourage people to take the plunge with presbyopia-correcting IOLs because I have to say my presbyopia-correcting IOL patients are some of my happiest. They have their youthful vision back, as I’ve heard them say, and they didn’t think that would be possible later in life. It’s such a great gift to patients.
Dr. Shultz: I have a couple of pearls to share. Ocular surface management is a major factor in success with presbyopia-correcting IOLs. Unfortunately, some practitioners do not critically evaluate the ocular surface before surgery. Fluorescein staining and an assessment of tear function are crucial. Don’t be afraid to tell patients that surgery must be delayed until problems with the ocular surface are resolved. Not addressing problems can lead to postoperative dissatisfaction for the patient, require more chair time, and discourage the physician and staff. In this situation, blame may be assigned to the technology when the fault actually lies with the unhealthy ocular surface.
My second tip is to start with extended depth of focus IOLs because they have a larger sweet spot and are associated with fewer unwanted visual phenomena compared to multifocal or trifocal IOLs. When you begin working with multifocal and trifocal IOLs, track your refractive results and be ready to offer a refractive enhancement.
CORRECTION ON THE CORNEA
Dr. McCabe: Who offers presbyopia laser vision correction (LVC) to patients?
Dr. Slade: We were involved in two early-stage trials for presbyopic ablations on the cornea. Both methods were problematic, and we withdrew from the trials. The methods later were abandoned. Centration and accuracy in a laser procedure are excellent, but reversal is not at all there yet.
Dr. Shultz: I currently perform PRK and LASIK but not SMILE. My first consideration is whether the patient is phakic or pseudophakic. I have performed LASIK on pseudophakic patients who had standard IOLs and desired clearer near vision, but I am slightly more likely to offer PRK to this population. I generally prefer monovision LASIK for patients who are less than 55 years old. Regardless of the form of LVC, I talk to patients about extending their range of vision and reducing their need for glasses.
Dr. McCabe: Dr. Shultz, you were involved with a lot of the early corneal inlays. What are your thoughts on allogenic corneal inlays?
Dr. Shultz: I was, as was Dr. Slade. The refractive results with synthetic corneal inlays were promising, but unfortunately the cornea rejected them. I am interested in allogenic inlays because the earlier technology demonstrated that the concept of a corneal inlay works. Moreover, the placement of an allogenic inlay is reversible, and rejection should be less of a problem.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
No. These agents are not available in Germany, where I practice.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
I offer bifocal, trifocal, and EDOF IOLs but not accommodating IOLs.
What are your thoughts on light adjustable lens technology?
I worked with the Light Adjustable Lens about 10 years ago, but I have not used the current model.
What are your thoughts on the use of small-aperture IOLs?
I implant the IC-8 Apthera. I think it is a great technology, especially for eyes with corneal irregularities. For example, I use it often for patients with previous RK and those with keratoconus or irregular astigmatism. Despite the availability of highly sophisticated biometry, however, IOL power calculation can be challenging. If the patient is not happy postoperatively and asks for further improvement, I counsel them to wait about 3 months for their refraction to stabilize. If they are still unhappy, we discuss implanting a spherical or toric add-on or supplementary IOL in the sulcus.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
Perfect the preoperative examination and pay particular attention to lens apex centration and angle alpha (to read more about the lens apex, click here).
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
I perform both presbyopic LASIK (PresbyMax, Schwind eye-tech-solutions) and monovision.
Corneal inlays have fallen out of favor, but in your opinion, do allograft/allogenic inlays have potential?
In my opinion the allogenic inlay being developed by Allotex is a promising technology.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
The preoperative discussion with patients guides treatment. Those who are somewhat hesitant about presbyopia treatment receive the Liberty2 IOL (1stQ). With this dual-lens system, a basic monofocal IOL is placed in the capsular bag and an add-on trifocal IOL is implanted in the sulcus. Different add powers are available.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
Implanting an add-on multifocal IOL is an option for patients who desire presbyopia correction after receiving a monofocal IOL.
Dr. McCabe: Dr. Shultz, you’ve also been involved in the development of scleral expansion devices for quite a while, correct?
Dr. Shultz: I became involved in the development of scleral expansion devices about 20 years ago. Some patients were extremely happy with their results. Unfortunately, the crystalline lens becomes too thick over time to function, so eventually patients need glasses. I think scleral expansion probably has a role for treating mild to moderate presbyopia.
Something we haven’t talked about but is on the horizon is the ability to adjust lenses that are already in the eye. We don’t have the capacity now, but I think refractive lens indexing will become part of our armamentarium.
PREFERRED TREATMENTS AND PATIENT SELECTION
Dr. McCabe: What does the presbyopia lifecycle look like for your patients? I try to think of their progression to presbyopia and what series of treatments I can fit together to help them over their lifetime. It’s a unique puzzle that includes the patient’s ocular anatomy and health, their expectations, and their age the first time they present as well as all the tools that we have.
With all the strategies we have for presbyopia correction, from LASIK to drops to RLE to cataract surgery to an enhancement of cataract surgery, how do you treat your patients?
Dr. Slade: Presbyopia is one of if not the most common refractive error that we treat in our practices because everybody who lives long enough experiences it. Unfortunately, we have had few options that work as well as LASIK does for patients with other refractive errors. It’s a challenge.
We have so many more treatments now than we did even 5 years ago. It’s wonderful that, perhaps for the first time, we can span the lifetime experience of patients. The first key is to have a bridge procedure that avoids lens exchanges and explants. The second key is to select the first one or two procedures that are as compatible as possible with what patients are likely to need in the future.

PHARMACOLOGIC AGENTS
Have you prescribed Vuity or used another presbyopia-correcting drop?
No. These products are not available in Italy, where I practice.
LENS OPTIONS
What are your current go-to IOLs for patients with presbyopia who are looking for excellent vision at all distances?
After implanting several diffractive trifocal IOLs, my go-to IOLs became the EDOF and enhanced monofocal/monofocal-plus categories.
What are your thoughts on light adjustable lens technology?
It is not available in Italy and is much too expensive.
What are your thoughts on the use of small-aperture IOL technology?
I implant the IC-8 Apthera in select patients to decrease corneal aberrations caused by prior surgery such as RK, pathology such as keratoconus, or trauma.
What pointers do you have for surgeons who are hesitant to segue into presbyopia-correcting IOLs?
Start with patients who have cataracts rather than RLE patients. I would also suggest to first use EDOF IOLs because they offer high-quality optics with fewer compromises than trifocal IOLs.
CORRECTION ON THE CORNEA
What LVC strategy do you use for presbyopia correction? When is this the best option?
Most of my patients seeking presbyopia treatment undergo Presbyond Laser Blended Vision performed with the MEL 90 excimer laser. I consider this procedure to be the best option for surgical presbyopia correction in patients without cataracts because the optical quality of the natural crystalline lens is higher than that of the best monofocal IOL. Moreover, most patients retain some accommodation, which augments the effect of the corneal procedure, and patients maintain blended vision and stereopsis (Figure).
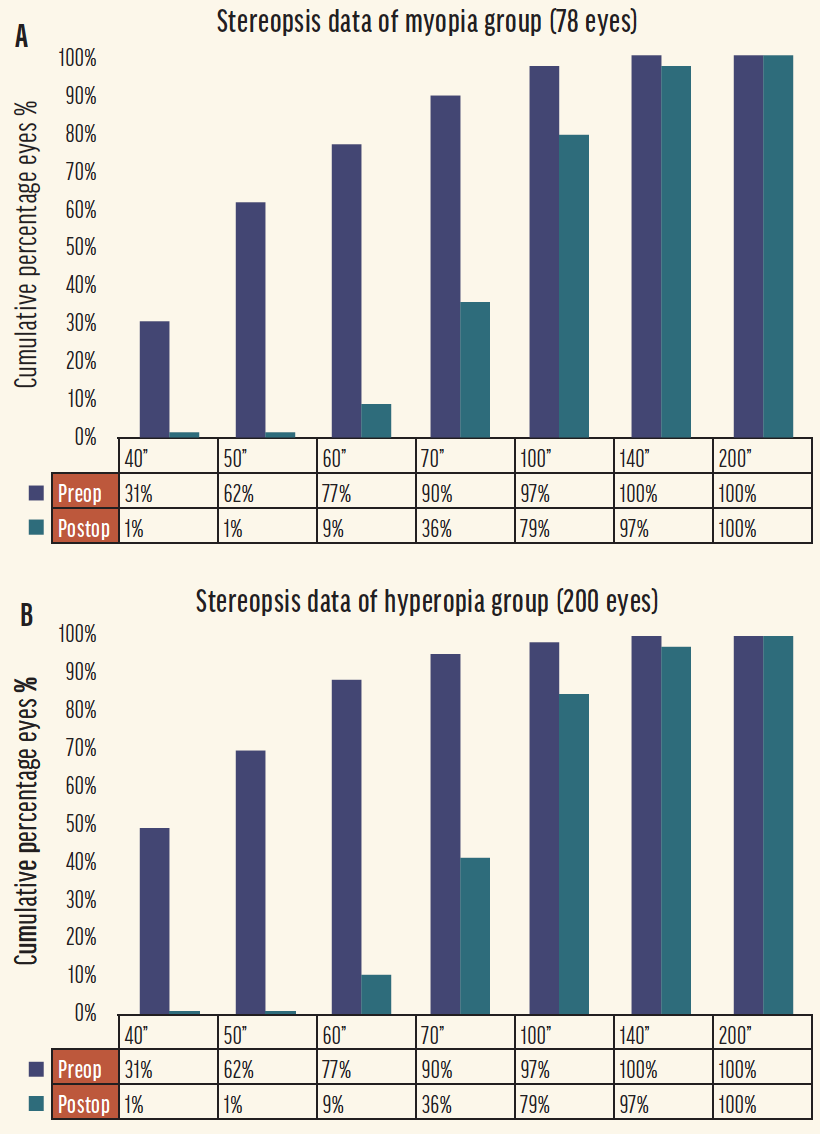
Figure. Cumulative histogram showing the stereoacuity before (corrected near visual acuity) and after (uncorrected near visual acuity) Presbyond for myopia (A) and hyperopia (B).
Abbreviations: Preop, preoperative; Postop, postoperative
Adapted from: Russo A, Reinstein DZ, Filini O, et al. Visual and refractive outcomes following laser blended vision with non-linear aspheric micro-anisometropia (PRESBYOND) in myopic and hyperopic patients. J Refract Surg. 2022;38(5):288-297.
Corneal inlays have fallen out of favor, but in your opinion do allograft/allogenic inlays have potential?
I have no experience with or interest in these devices.
What other future treatments have promise?
New EDOF lenses and maybe accommodating IOLs currently in the pipeline.
PREFERRED TREATMENTS
How do you know what presbyopia treatment to use when and in which patients?
Patients who do not have cataracts undergo the Presbyond procedure. Those who have cataracts undergo cataract surgery and the implantation of an EDOF IOL. To my mind, the procedures produce similar effects.
Today, we talk about continuity of care and making decisions that are right for patients over the course of their lifetime. How can you retain patients with presbyopia so that they return to your practice for future needs?
I inform patients undergoing Presbyond treatment that the effect will not last forever. They may need a touch-up in 5 to 10 years, and they can undergo cataract surgery when they develop cataracts.
Dr. McCabe: Is there anything on the horizon that, in your opinion, will be the bridge we need? I know you said presbyopia drops are not the perfect bridge for you. Is there something else on the horizon that you think might fill that role of a bridge treatment better or differently than drops?
Dr. Slade: There are some candidates. One is aggressive RLE. Monovision LASIK is a wonderful procedure, but multifocal LASIK is not. Another option could be an inlay that is biocompatible with the cornea. The corneal inlays that we had didn’t fail because of their visual results; they failed because of their poor biocompatibility. Third, a very long-acting drop would be a good bridge treatment.
Dr. Shultz: A nice aspect of prescribing presbyopia drops is that it can help identify patients who may be candidates for presbyopia surgery later in their lives and condition them to consider surgical options. If someone is willing to spend $1,000 a year on eye drops, that person may well be willing to undergo RLE or another procedure. These individuals are identifying themselves as prioritizing spectacle independence.
I offer presbyopia drops to patients with early presbyopia. Doing so builds my presbyopia practice. The best surgical option may not yet be available for certain patients, and drops allow them to delay surgical intervention. I expect allogenic corneal inlays and laser procedures to become the next step for patients who are 45 to 55 years old and have presbyopia but no changes in their crystalline lenses. The third step is lens-based procedures.
Dr. McCabe: Dr. Talley Rostov, how are you fitting the puzzle pieces together, and what are your thoughts on the future?
Dr. Talley Rostov: Education is key, especially for patients with early presbyopia and myopia who undergo SMILE or LASIK. Offering them a presbyopia drop is not the perfect solution, but at least for the moment, it can help to increase their range of vision after LVC, whether that be SMILE or LASIK. It can also delay when you might start considering RLE for these patients.
Of course, it is also important to be cognizant of risks such as retinal detachment and high myopia. I have mild concern about whether the presbyopia drops that include pilocarpine can also potentiate that. It’s wise to pause with these patients.
Dr. McCabe: Those are great points. Nothing comes without risks. We must weigh the benefits against the risks for each patient based on their individual needs and eye health. Dr. Shafer, what’s your approach, and is there anything you’re excited about for the future?
Dr. Shafer: I start the patient journey by seeing if the individual who’s coming to me for LVC in their late 30s to early 40s can tolerate a tiny offset. If they can tolerate even just -0.50 to -0.75 D in the nondominant eye, I’ll recommend that offset because I know they’ll be happier for longer.
I love RLE, and these patients are some of the happiest patients I have. But, every time I do RLE on somebody who’s a little on the younger side, I think about the longevity of the IOL in the eye.
Having a bridge to get patients to the point when they are ready for cataract surgery would be great. Maybe it is pharmacologic but in a sustained drug delivery form administered intracamerally or intracanalicularly or even just via a contact lens. These are all possibilities as the world of sustained drug delivery continues to develop. I hope that, in the future, we are not handling a million dislocated IOLs.
Dr. McCabe: I was just thinking that, Dr. Shafer. I see a lot of dislocated IOLs in my practice. We need to find better solutions for them as well.
Dr. Zhu: I see myself as the patient’s presbyopia physician over their lifetime because I’m not their Vivity doctor. I’m not their PanOptix doctor. I am their presbyopia physician, and I’m choosing the best technology for them at that period in their life.
Early in the disease state, we’re all trying to preserve the crystalline lens. If the eye retains partial accommodation, we don’t want to replace the lens. There are a lot of modalities available or under development today that can help to prolong the life of the natural lens and extend depth of focus. They include presbyopia drops, allogeneic corneal inlays, and phakic IOLs. Within the category of presbyopia drops, much work remains to be done. We’ve seen only one candidate so far, but many others are coming. Some of these are pilocarpine-based, and others are not. At least one product softens the lens. I’m excited to see what becomes of these options. I do a large number of RLE procedures in my practice, and these patient are happy. I always, however, try to preserve patients’ natural lenses because nothing beats Mother Nature.
Dr. McCabe: We all want to be 20 years old again with perfect lenses. That’s what I tell my patients.
Dr. Zhu: Exactly. I want to delay lens surgery for as long as possible—ideally until they are ready for cataract surgery. We’re practicing in a time when there are more options than ever before that could help our patients with early presbyopia until we can offer them a more permanent solution.
Dr. McCabe: I think that presbyopia presents an opportunity to create relationships with patients we might not have seen before and to demonstrate that we care about their needs and are looking for solutions that work for them during different phases of their lives. This can encourage them to refer family members and friends to the practice.
This has been a great discussion. I think we all learned a few things that we can take back to our practices to improve the way that we approach presbyopia correction. I really want to thank the panelists for sharing their pearls, thoughts, and approaches and giving us a peek into the future.
NEXT IN THIS ISSUE