
We have routinely used the IOLMaster (Carl Zeiss Meditec) since 1999. We started using the IOLMaster 500 in 2010, and, in August 2014, we added the IOLMaster 700.
With the help of optical biometry and the use of optimized A-constants—published in the User Group of Laser Interference Biometry (ULIB) database—collectively, cataract surgeons can achieve much better predictability in refractive outcomes than we could in 1999. With that said, the majority of surgeons continue to come within ±0.50 D of the intended correction in only 78% of patients, thus necessitating enhancements in some of those cases.1 One of the weak points for better predictability is estimation of the effective lens position. Even if the C-constant is of help,2 this factor remains an estimating tool.
I have been impressed by my early experience with the IOLMaster 700.
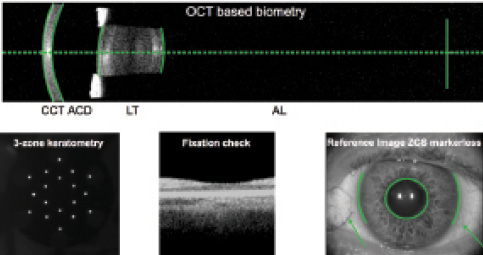
Figure 1. OCT detected morphologic structures (green lines).
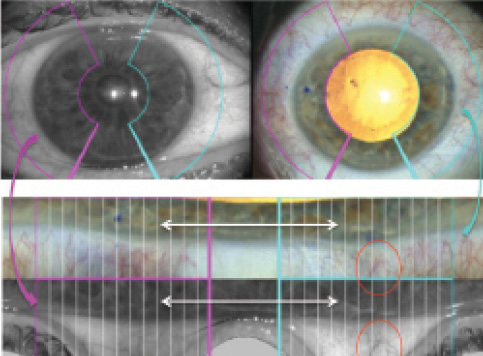
Figure 2. In this example, the limbal region with conjunctival
vessels is seen. The IOLMaster reference image aligns with the
image from the microscope; the fold-out reference image and
microscope image can be adjusted on the touchscreen of Callisto.
Our experience with the IOLMaster 700 in the past 11 months includes about 1,000 patient examinations. We now use this technology as part of our daily examination routine. The multitouchscreen and graphical user interface help to speed up the examinations, which are delegated to our assistant personnel. Integrated power calculations in the new Haigis Suite (Haigis-L and Haigis-T formulas) make it unnecessary to key data into online toric IOL calculators. Thus, in our practice, the IOLMaster 700 was immediately accepted.
In our office and ambulatory surgical center, we have 40 computer workplaces that integrate with Tomedo (http://www.tomedo.de/faq.html), our office's practice management system. This server-based software runs on Mac OS 10.9.5 and integrates with the Forum eye care data management system (Carl Zeiss Meditec). Thus, we can transfer patient data via Forum into the IOLMaster 500 and 700 and can redirect IOLMaster data into Forum, allowing us to display all data at every workplace and also in the operating room (Figure 1). We can also use these data with the Zeiss Cataract Suite markerless and Callisto eye (both by Carl Zeiss Meditec). Thus, the reference image of the IOLMaster and the online image of the OPMI Lumera microscope, aligned through Callisto eye, enable computer assistance for the surgeon (Figure 2), resulting in better centered, larger, and rounder capsulorrhexes and markerless alignment of toric IOLs. About 95% of alignments performed in our center are fully automatic; the residual 5% need interactive but still markerless alignment (Figures 3 and 4).
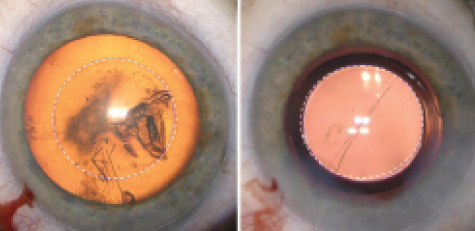
Figure 3. A centered and large capsulorrhexis, with overlay
assisted by Callisto eye.
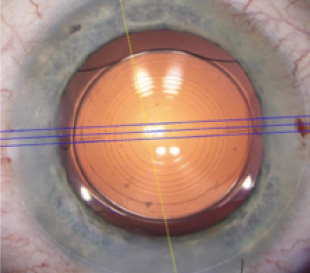
Figure 4. The dotted line marks the
limbal region; the yellow line marks the
horizontal 0° axis; and the blue lines
indicate the steepest meridian.
According to comparative measurements taken with the IOLMaster 500 and IOLMaster 700 in 84 eyes, the differences in axial length and keratometry measurements between the devices were 0.02 mm and 0.08 D, respectively. Also, 99.4% of the measurements taken with the IOLMaster 700 were predicted with the IOLMaster 500, and that is highly significant. Thus, the ULIB database is also valid for the IOLMaster 700.3
With regard to measuring ocular structures for biometry, this is the first time that OCT technology can be used to project morphologic structures, control fixation with the macula, and control IOL position pre- and postoperatively. Also, the decentration or tilt of the crystalline lens and the IOL can be registered.
As the IOLMaster 700 continues to mature as a technology, we expect additional features, such as measurement of more rings with keratometry and of anterior and posterior corneal surfaces for calculation of corneal thickness. These are the next steps for optimizing refractive outcomes.
Ekkehard Fabian, MD
• AugenCentrum, Rosenheim, Germany
• prof.fabian@augencentrum.de
• Financial disclosure: Consultant (Carl Zeiss Meditec, Abbott Medical Optics)

