



It is now widely accepted that there is an epidemic of myopia in East and Southeast Asia. In mainland China, Hong Kong, Taiwan, Japan, South Korea, and Singapore, the prevalence of myopia is between 80% and 90% in students completing secondary education.1 In cities in this part of the world, most children now complete high school, and a majority go on to some form of post-secondary education. These trends are also seen in rural areas, meaning that high prevalence rates are increasingly representative of the whole cohort of young adults, and they will spread throughout the adult population as these highly myopic young adults grow older.
This article discusses five fundamental facts about the growth in the prevalence of myopia, and, more specifically, of high myopia, acquired high myopia, and pathologic myopia, in East and Southeast Asia, and the implications for populations in Europe.
HIGH MYOPIA IS ON THE RISE

What has been less widely recognized is that the prevalence of high myopia has also increased and, in relative terms, has done so at a faster rate than the prevalence of myopia overall, leading to a growing proportion of high myopia among those with myopia. In cities in East and Southeast Asia, the prevalence of myopia has increased from between 20% and 30% to between 80% and 90% in young adults of school-leaving age over the past 50 years, representing a three- to fourfold increase. Something of a world record is held by 19-year-old male conscripts in Seoul, South Korea, where 96.5% of the cohort members are myopic.2 For high myopia, the prevalence has increased from between 1% and 2% in similar groups to 20% or even higher, representing more like a 10-fold increase. Values for the prevalence of high myopia with a cutoff of -6.00 D among senior school students, or the nearest equivalent, from selected studies are compared in Figure 1.
At a glance
• It is widely accepted that there is an epidemic of myopia in East and Southeast Asia, but what has been less recognized is that the prevalence of high myopia has also increased.
• The speed with which the prevalence of myopia has increased shows that environmental factors, primarily education and the amount of time that children spend outdoors, can have a major influence.
• Recent reports show that the prevalence of myopia is increasing in Europe and in people of European ancestry in other parts of the world.
• A new form of high myopia, acquired high myopia, has already appeared in East and Southeast Asia and is likely to appear in Europe as the prevalence of myopia and high myopia increases.
THE AGE Of ONSET OF MYOPIA IS DECREASING

It is not difficult to understand how the prevalence of high myopia has increased so much. One of the features of the myopia epidemic is that the age of onset has decreased as the prevalence of myopia has increased.3 Early-onset myopia naturally has more time to progress before refraction stabilizes, and the rates of progression tend to be higher, both because progression appears to be faster at younger ages4 and because, where the prevalence of myopia is high, progression rates also appear to be elevated.5 This results in a nonlinear increase in the prevalence of high myopia as the prevalence of myopia increases.
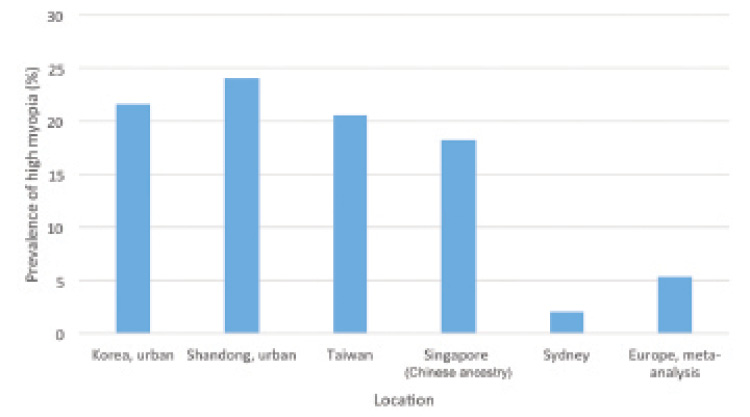
Figure 1. Comparison of the values for the prevalence of high myopia (cutoff, -6.00 D) in senior school students from selected studies in varying locations.
A striking feature of the changes in the prevalence of high myopia with age is that the increases in prevalence first appear around the age of 11 to 13 and then continue to increase at least until age 17.3,6 If we consider the case of a child who first becomes myopic around age 6, with the progression rates defined by Sankaridurg and Holden,4 children will start to pass a -6.00 D threshold for high myopia by around age 11 to 13.
It is therefore reasonable to assume that the early-onset high myopia apparent before age 11 is predominantly classical genetic high myopia, whereas that which appears after this age is predominantly environmental or acquired in origin. Supporting the hypothesis that high myopia is now predominantly acquired, rather than genetic in origin, Jonas and colleagues7 have recently shown that, in older cohorts, high myopia has limited or even negative associations with education. In contrast, in the younger cohorts from East Asia, high myopia was strongly associated with education-related parameters.
ENVIRONMENTAL FACTORS PLAY A MAJOR ROLE

Myopia was once thought to be almost entirely of genetic origin, based on the high heritability values reported in twin studies. However, the speed with which the prevalence of myopia has changed in this part of the world shows that environmental factors can have a major influence on the prevalence of myopia and must have played a major role in its increase.8 The two environmental factors that have been identified as important are (1) education, whether measured in terms of years of education or school grades, and (2) the amount of time that children spend outdoors.
Links between education and myopia have been documented for many years,8 but the discovery of the importance of time spent outdoors during daylight hours is more recent9-11 and, as we proposed, appears to be due to exposure to bright light. Bright light, therefore, provides a modifiable protective factor that can be used for prevention. Recently, clinical trials have confirmed the efficacy of this approach,6,12,13 and getting children outdoors more is now the basis of national myopia prevention programs in Taiwan and Singapore.
THE PREVALENCE OF MYOPIA IS INCREASING IN EUROPE, BUT THE CHANGES ARE NOT AS DRAMATIC

An important question for European readers is whether similar changes are appearing in Europe and in populations of European ancestry in other parts of the world. Recent reports show that the prevalence of myopia is increasing in Europe,14 in the United States in in people of European and African ancestry,15 and in people of European ancestry in Australia.11 However, compared with the increases seen in East and Southeast Asia, the changes in these groups have been limited.
At least in part, these increases seem to be driven by increases in educational pressures, although whether education provides a complete explanation has been challenged.16 The results of the Gutenberg Health Survey provide strong support for the role of education in producing a higher prevalence of myopia in younger cohorts,17 as younger, more myopic cohorts had greater educational exposures while there had been little change in genetic risk factors for myopia.
Similarly, the Rotterdam Eye Study has reported on gene-environment interactions in relation to myopia.18 Further analysis of the data, which covers three sequential cohorts of older people, shows that the prevalence of myopia has increased progressively in the more recent cohorts. This increase parallels that of increased educational exposures, again with little to no change in genetic risk factors. Therefore, education does appear to be an important factor in driving increases.
FUTURE PROSPECTS ARE NOT PROMISING

Given the strength of the evidence supporting the role of education, prospects for the future are not promising. The results of the Programme for International Student Assessment (PISA) surveys carried out by the Organisation for Economic Cooperation and Development (OECD) have become an important influence on education policies at national and community levels. Many countries officially express concern about their place in the PISA rankings, and some have taken action. For example, Poland has moved from being below the OECD average to being one of the top-placed countries in Europe, but it is still behind the highly myopic, top-achieving nations in East and Southeast Asia. With all that we know about the impact of intensive education on myopia, this would suggest that the prevalence of myopia and high myopia should have increased in Poland; the data, however, are not available to test this hypothesis.
Unfortunately, there is a remarkable lack of recent data on myopia in older school-aged children in Europe. Recent comprehensive studies on the development of myopia in children and adolescents are particularly lacking, with only the Northern Ireland Childhood Errors of Refraction study19,20 and a study from Poland21 providing good data based on cycloplegic refractions. More data are certainly required.
Despite the lack of data from Europe, it is clear that this new form of high myopia—acquired high myopia—has already appeared in East and Southeast Asia, and it is likely to appear in Europe as the prevalence of myopia and high myopia increases. It is important for clinicians to be alert to its existence.
One of the important and as yet unresolved questions about acquired high myopia is whether it carries the same potential for the development of pathologic myopia that exists with the more classical genetic form. If the potential is the same, then the 10-fold increase in prevalence of high myopia that has taken place in East and Southeast Asia should lead to a marked increase in pathologic myopia; this, in turn, would place severe strains on ophthalmic services, particularly in a country such as China, where the development of the education system and the epidemics of myopia and high myopia have outpaced the development of service provision.
Given that the percentage of high myopes who show pathologic signs depends on age, with pathologic signs clearly increasing with age, and that the emergence of significant levels of acquired myopia is relatively recent, it is too early to definitively answer this question. Only time will tell, but, at this stage, it would be unwise to assume that acquired high myopia will be benign and devoid of pathologic consequences, and we should carefully monitor the emergence of future problems.
CONCLUSION
We believe that Europe needs a system for surveillance of refractive errors in school-aged children and adolescents. This could be achieved cost-effectively through monitoring of visual acuity, as loss of visual acuity during schooling appears to be strongly associated with the emergence of myopia.22 Some relevant data are already collected through school screening programs, and consolidating them would give us a better idea of the future. Fortunately, research on prevention has advanced to the stage at which we now have means of both slowing the onset of myopia—with increased time outdoors—and slowing its progression, and these steps can be implemented if required.
1. Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379(9827):1739-1748.
2. Jung SK, Lee JH, Kakizaki H, Jee D. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in Seoul, South Korea. Invest Ophthalmol Vis Sci. 2012;53(9):5579-5583.
3. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(1):27-33.
4. Sankaridurg PR, Holden BA. Practical applications to modify and control the development of ametropia. Eye (Lond). 2014;28(2):134-141.
5. Donovan L, Sankaridurg P, Ho A, Naduvilath T, Smith EL 3rd, Holden BA. Myopia progression rates in urban children wearing single-vision spectacles. Optom Vis Sci. 2012;89(1):27-32.
6. He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA. 2015;314(11):1142-1148.
7. Jonas JB, Xiang F, Zeng Y, et al. Education-related parameters in high myopia: adults versus school children. PLoS One. 2016;11(5):e0154554.
8. Morgan I, K. Rose. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1-38.
9. Jones LA, Sinnott LT, Mutti DO, et al. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007;48(8):3524-3532.
10. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279-1285.
11. French AN, Morgan IG, Burlutsky G, Mitchell P, Rose KA. Prevalence and 5- to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology. 2013;120(7):1482-1491.
12. Wu PC, Tsai CL, Wu HL, Yang YH, Kuo HK. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080-1085.
13. Jin JX, Hua WJ, Jiang X, et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast China: the Sujiatun Eye Care Study. BMC Ophthalmol. 2015;15:73.
14. Williams KM, Bertelsen G, Cumberland P, et al; European Eye Epidemiology (E(3)) Consortium. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489-1497.
15. Vitale S, Sperduto RD, Ferris FL 3rd. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol. 2009;127(12):1632-1639.
16. Williams KM, Verhoeven VJ, Cumberland P, et al. Prevalence of refractive error in Europe: the European Eye Epidemiology (E(3)) Consortium. Eur J Epidemiol. 2015;30(4):305-315.
17. Mirshahi A, Ponto KA, Hoehn R, et al. Myopia and level of education: results from the Gutenberg Health Study. Ophthalmology. 2014;121(10):2047-2052.
18. Verhoeven VJ, Buitendijk GH, et al, for the Consortium for Refractive Error and Myopia (CREAM). Education influences the role of genetics in myopia. Eur J Epidemiol. 2013;28(12):973-980.
19. O’Donoghue L, McClelland JF, Logan NS, et al. Refractive error and visual impairment in school children in Northern Ireland. Br J Ophthalmol. 2010;94(9):1155-1159.
20. Breslin KM, O’Donoghue L, Saunders KJ. A prospective study of spherical refractive error and ocular components among Northern Irish schoolchildren (the NICER study). Invest Ophthalmol Vis Sci. 2013;54(7):4843-4850.
21. Czepita D, Zejmo M, Mojsa A. Prevalence of myopia and hyperopia in a population of Polish schoolchildren. Ophthalmic Physiol Opt. 2007;27(1):60-65.
22. Xiang F, He M, Morgan IG. The impact of severity of parental myopia on myopia in Chinese children. Optom Vis Sci. 2012;89(6):884-891.
Amanda N. French, BAppSci (Orth) Hons, PhD
• Lecturer, Discipline of Orthoptics, Graduate School of Health, University of Technology Sydney, Ultimo, Australia
• Financial interest: None acknowledged
Mingguang He, MD, PhD
• Professor, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangzhou, China
• Professor of Ophthalmic Epidemiology, Department of Ophthalmology, University of Melbourne and Centre for Eye Research Australia, Melbourne, Australia
• Financial interest: None acknowledged
Ian G. Morgan, BSc, PhD
• Visiting Fellow, Research School of Biology, Australian National University, Canberra, Australia
• Visiting Fellow, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangzhou, China
• Ian.Morgan@anu.edu.au
• Financial interest: None acknowledged
Kathryn A. Rose, PhD
• Professor, Discipline of Orthoptics, Graduate School of Health, University of Technology Sydney, Ultimo, Australia
• Financial interest: None acknowledged
