Cataract surgery is the most commonly performed surgical procedure in Belgium, with approximately 120,000 operations completed in 2014 among a population of 11 million. Today in our country, even though about 10% of these surgeries are performed in an outpatient setting, reimbursement for cataract surgery at an extramural surgery center—that is, outside the walls of a hospital, at an ambulatory surgery center—remains significantly less than that for the same operation conducted in a hospital.
AT A GLANCE
• A mandate to perform most cataract surgeries at extramural eye centers could save health care and insurance companies millions of euros per year.
• In the authors’ experience, renting a mobile femtosecond laser unit reduced the financial risk of incorporating the technology into practice and far surpassed the center’s goal of 5% acceptance.
• In an observational study, the femtosecond laser aided in the ability to provide exact, consistent, and predictable treatment for all cases, even challenging ones.
Equally compelling, worldwide, 19 million cataract operations are performed each year.1 The World Health Organization estimates that this number will increase to 32 million by 2020, given that the population of individuals over 65 years of age will double between 2000 and 2020.2,3
Considering the increasing number of cataract operations to be performed annually around the world, it would make sense to have a mandate to perform most cataract surgeries at extramural eye centers; this would save health care and insurance companies millions of euros per year. Furthermore, extramural surgery centers may be more likely to have newer technologies and to have employees who are dedicated specifically to ophthalmic care, creating a more efficient and patient-centric environment for cataract surgery. (For patient benefits related to extramural eye clinics, see the sidebar below.)
This article aims to detail the barriers to moving more ophthalmic surgery into extramural eye clinics and reviews the results of a recent study of laser-assisted lens fragmentation in an extramural setting.
BARRIERS TO MORE WIDESPREAD USE
Techniques and methodologies that have the potential to improve the quality of cataract surgery could profoundly affect the quality of life of millions of people across the globe. We believe the primary barriers to more widespread use of extramural eye clinics for cataract surgery are related to tradition, habit, and outdated regulations, rather than to anything evidence-based. It is up to ophthalmic surgeons to perform surgery responsibly in environments that are safe for our patients, whether that be in a major hospital or an extramural eye clinic. Conversely, the burden falls squarely on the shoulders of extramural eye clinic owners to continually reinvest in new technologies in order to provide patients with state-of-the-art care.
One such technology is the femtosecond laser, which is used in cataract surgery to increase the reproducibility, precision, accuracy, and safety of traditional manual phacoemulsification.4-6 Essentially, in laser-assisted cataract surgery (LACS), the laser takes the most delicate steps out of the hands of the surgeon and performs them with greater precision. This technique is becoming increasingly popular among today’s cataract surgeons.7,8
Just as any practice should before buying a new technology, our extramural eye clinic, Eye Clinic Okulus in Kortrijk, Belgium, conducted a financial analysis to determine whether the cost of a femtosecond laser would be justified. For us, it was decided not to purchase a femtosecond laser but rather to hire a mobile unit for several days a month. This meant renting a laser unit capable of use at multiple sites (Femto LDV Z8; Ziemer Ophthalmic Group) from an independent company in France. We have found that this service has reduced our financial risk of incorporating the technology into practice and has far surpassed our goal of 5% acceptance.
precise, CONSISTENT, PREDICTABLE TREATMENT
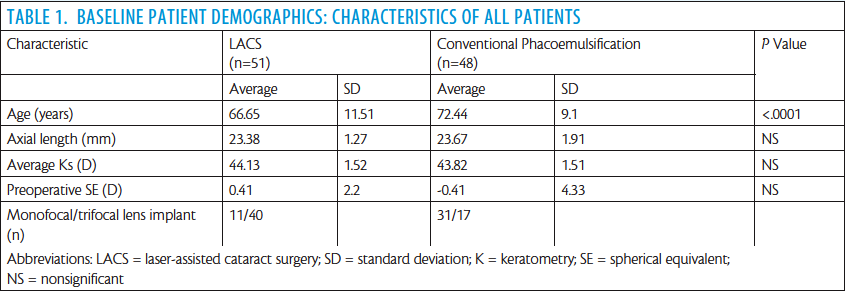
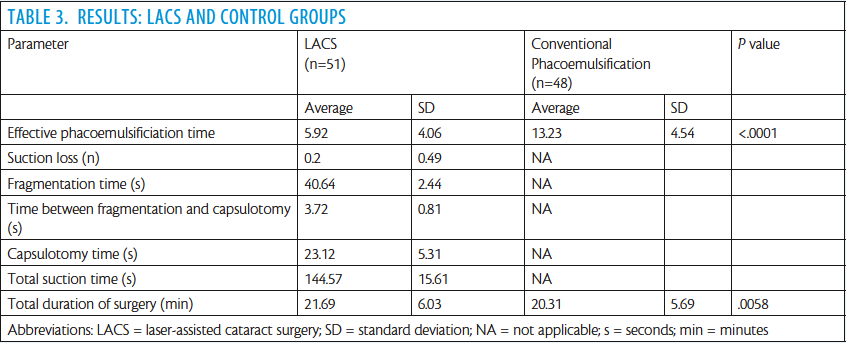
We recently performed an observational case series study to evaluate the effectiveness and safety of laser-assisted lens fragmentation in an extramural setting with the mobile femtosecond laser. Specifically, the study aimed to compare the adverse event profile of laser lens fragmentation and capsulotomy with that of standard phacoemulsification. The main measures evaluated were effective phacoemulsification time (EPT), total duration of surgery, completeness of capsulotomy, suction time, and complications.
In addition to the results we share in the sidebar Mobile LACS in an Extramural Setting on the following pages, what we found is that contracting out for use of a mobile femtosecond laser unit is one way in which extramural eye center owners can successfully reduce financial risks. As a general average, 20% of our patients now opt for LACS.
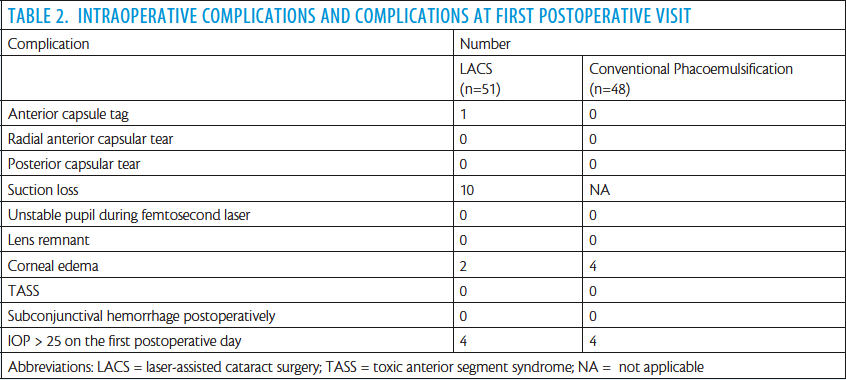
In our study, there was essentially no difference in total number of complications between the LACS and conventional phacoemulsification groups. With the use of the femtosecond laser, we are able to provide precise, consistent, and predictable treatment for all cases, even in otherwise challenging cases, such as eyes with anterior corneal dystrophy, Fuchs dystrophy, or pseudoexfoliation. In these cases, the performance of the femtosecond laser takes the angst away with creation of a great rhexis. In a mature cataract, the laser also decompresses the capsular bag to avoid the Argentinian flag sign, an ominous sign of impending disaster. The EPT was reduced in the LACS group in our study, which is consistent with findings in another similar study.9
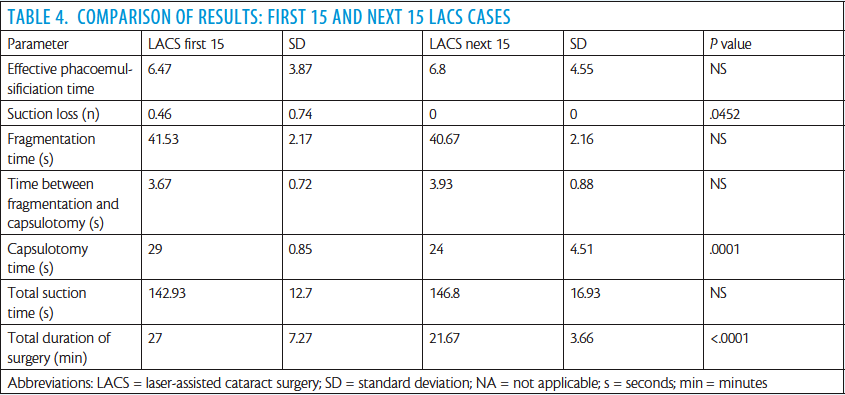
In this small sample case series, LACS with a mobile femtosecond laser facilitated complete and precise capsulotomy and highly effective and reproducible lens fragmentation. The safety of the procedure was good, even using a laser that travels around to different eye clinics in Europe.
SUMMARY
Mandating the performance of more cataract surgery procedures at extramural eye centers may not only save millions of euros per year in health care costs, but it also may help to create a more efficient environment for cataract surgery. Furthermore, we have found that hiring the use of a mobile femtosecond laser unit for several days a month can reduce the financial risk of incorporating the technology into practice.
In our study, intraoperative complications were similar in the LACS and conventional phacoemulsification groups. LACS with a mobile femtosecond laser that travels around to eye clinics across Europe seems to be as safe as conventional phacoemulsification. Although anterior capsule tags remain a concern, the LACS and control groups had similar rates of capsular complications.
1. Wu BM, Williams GP, Tan A, Mehta JS. A comparison of different operating systems for femtosecond lasers in cataract surgery. J Ophthalmol. 2015;2015:616478.
2. Brian G, Taylor H. Cataract blindness–challenges for the 21st century. Bull World Health Organ. 2001;79(3):249-256.
3. Donaldson KE, Braga-Mele R, Cabot F, et al; ASCRS Refractive Cataract Surgery Subcommittee. Femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013;39(11):1753-1763.
4. Abell RG, Vote BJ. Cost-effectiveness of femtosecond laser-assisted cataract surgery versus phacoemulsification cataract surgery. Ophthalmology. 2014;121(1):10-16.
5. Ranka M, Donnenfeld ED. Femtosecond laser will be the standard method for cataract extraction ten years from now. Surv Ophthalmol. 2015;60(4):356-360.
6. Nagy ZZ. New technology update: femtosecond laser in cataract surgery. Clin Ophthalmol. 2014;8:1157-1167.
7. Chee SP, Yang Y, Ti SE. Clinical outcomes in the first two years of femtosecond laser-assisted cataract surgery. Am J Ophthalmol. 2015;159(4):714-719.
8. Berdahl JP, Jensen MP. The business of refractive laser assisted cataract surgery (ReLACS). Curr Opin Ophthalmol. 2014;25(1):62-70.
9. Daya SM, Nanavaty MA, Espinosa-Lagana MM. Translenticular hydrodissection, lens fragmentation, and influence on ultrasound power in femtosecond laser-assisted cataract surgery and refractive lens exchange. J Cataract Refract Surg. 2014;40(1):37-43.
Caroline Cardyn, MD
• Consultant Ophthalmologist, Okulus Eye Clinic, Kortrijk, Belgium
• Consultant Ophthalmologist, AZ Zeno, Knokke, Belgium
• Financial interest: None acknowledged
Matthias Claeys
• Medical Student, Ghent University, Ghent, Belgium
• Consultant Medical Student, Okulus Eye Clinic, Kortrijk, Belgium
• matthias.claeys@hotmail.com
• Financial interest: None acknowledged
Marnix Claeys, MD
• Consultant Ophthalmologist and Medical Director, Okulus Eye Clinic, Kortrijk, Belgium
• Financial interest: None acknowledged
MOBILE LACS IN AN EXTRAMURAL SETTING
1. Arbisser LB, Schultz T, Dick HB. Central dimple-down maneuver for consistent continuous femtosecond laser capsulotomy.
J Cataract Refract Surg. 2013;39(12):1796-1797.