

In recent years, small incision lenticule extraction (SMILE) has become a widely used method for surgical correction of myopia and myopic astigmatism.1 Clinical trials have established that the efficacy and safety of the SMILE procedure are comparable with those of LASIK.2-4 Its small-incision, flapless, intrastromal approach to tissue ablation makes SMILE an attractive option for the surgical correction of appropriate levels of refractive error. Additionally, the fact that the anterior stroma is left intact suggests that SMILE may have some advantages over LASIK, such as reduction of dry eye symptoms and faster restoration of corneal innervation.
AT A GLANCE
• Sub-cap lenticule extraction is a modification of the SMILE procedure that can be used to eliminate residual myopic refractive error after SMILE.
• During the enhancement, the original interface of the primary SMILE procedure is used as the superior plane of the new lenticule.
• The new lenticule is removed through the original corneal incision.
With any refractive procedure, the possibility of enhancement is an important consideration. Several methods of enhancing unsatisfactory visual results after SMILE have been published. These include the use of topography-guided excimer laser surface ablation5 and a newer procedure called Circle, in which the original SMILE cap is converted into a flap to allow further stromal ablation.6
Another alternative is to perform a secondary SMILE procedure. This approach preserves the advantages of SMILE, including avoiding postoperative patient pain and dry eye and maintaining the biomechanical properties of the cornea.7 The challenge with this approach, however, is to avoid interference with the existing interface where the primary SMILE lenticule was removed. This should be possible by performing the second SMILE procedure either above or below the existing interface. If the primary cap was thick enough, then thin-flap LASIK can be performed.
Reinstein et al showed that the maximum thickness of the epithelium after primary myopic SMILE is 80 µm.8 This means that a retreatment with a thin flap of 100 µm would not cross either the existing cap interface or into epithelium, creating a cryptic buttonhole.
SUB-CAP LENTICULE EXTRACTION
We recently published a case report describing a new method for refractive enhancement after a primary SMILE procedure, which we call sub-cap lenticule extraction (sub-cap LE).9 This modification of the SMILE procedure avoids the problem of interference with the original interface. In sub-cap LE, the original interface of the primary SMILE procedure is used as the superior plane of the new lenticule. During the enhancement, the VisuMax femtosecond laser (Carl Zeiss Meditec) is used to create only the inferior plane and sidecut of the new lenticule; the surgeon then stops the ablation and the new lenticule is removed through the original corneal incision.
two case reports
Our original report of sub-cap LE included a single case presentation of our successful use of the technique in a 53-year-old woman who experienced blurred distance vision after bilateral SMILE for correction of moderate myopia.8 We have since used the same technique in a series of 12 eyes with similarly successful results. Two more case examples are described here.
Case No. 1. A 32-year-old woman with high myopia requested refractive surgery. At presentation, the patient’s distance UCVA in her left eye was 20/800; with a manifest refraction of -9.00 -0.50 X 160º, distance BCVA in her left eye was 20/20. A SMILE procedure was performed in this eye.
After the procedure (Figure 1), distance UCVA in the patient’s left eye was 20/30; with a manifest refraction of -0.25 -0.50 X 150º, distance BCVA was 20/16. Despite what might seem like an excellent refractive result, the patient expressed a desire for clearer uncorrected distance vision. It was decided to offer her enhancement with sub-cap LE.
Case No.1
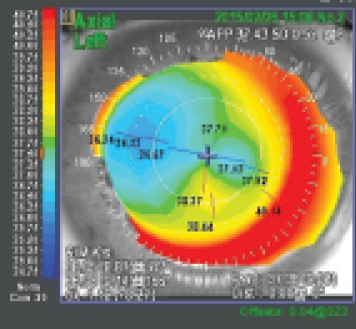
Figure 1. Corneal topography after the primary SMILE procedure.
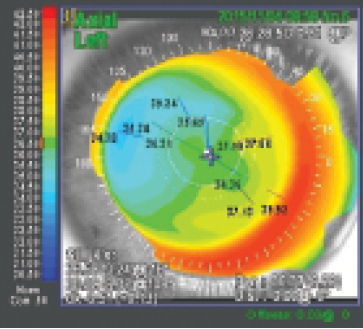
Figure 2. Corneal topography 6 months after enhancement with sub-cap LE.
Approximately 8 months after the primary SMILE procedure, sub-cap LE was performed in the patient’s left eye. Six months after the secondary procedure (Figure 2), the patient’s distance UCVA was 20/16. Distance BCVA was also 20/16 with a manifest refraction of 0.50 -0.50 X 65º.
Case No. 2. A 30-year-old woman with significant myopia expressed interest in refractive surgery. Baseline distance UCVA in her left eye was 20/800, correcting to 20/20 with refraction of -6.50 -0.50 X 120º. The patient underwent SMILE for myopic correction in this eye.
Case No.2
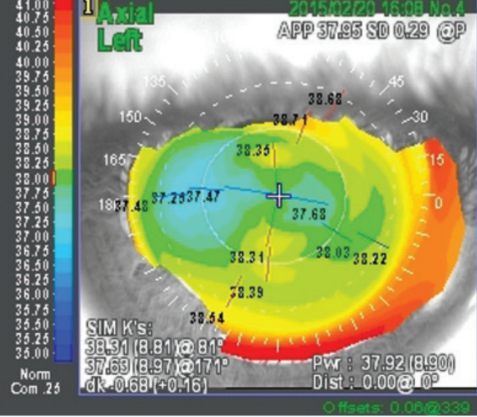
Figure 3. Corneal topography after the primary SMILE procedure.
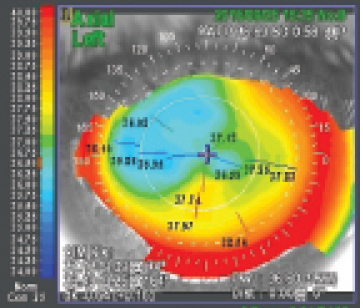
Figure 4. Corneal topography 6 months after enhancement with sub-cap LE.
After the procedure (Figure 3), the patient’s distance UCVA in her left eye was 20/40, correcting to 20/20 with refraction of -0.50 -0.50 X 155º. The patient was disappointed in the uncorrected vision result, and she was offered sub-cap LE as an enhancement procedure.
Eight months after the primary SMILE procedure, sub-cap LE was performed in the patient’s left eye. Six months after the enhancement (Figure 4), the patient’s distance UCVA was 20/20, correcting to 20/16 with refraction of 0.75 -0.50 X 135º.
CONCLUSION
As these two cases and our original case8 illustrate, sub-cap LE can help to eliminate residual myopic refractive error after primary SMILE. Clearly, more experience is needed, in more hands, to verify the safety and efficacy of this enhancement approach after an unsatisfactory SMILE result.
For surgeons who are familiar with the SMILE procedure and have the appropriate equipment, modifying the technique to perform sub-cap LE should be straightforward, with only a short learning curve. We look forward to reading reports of the results of other surgeons who adopt this useful technique.
1. Reinstein DZ. Are intrastromal treatments the future of refractive surgery? CRST Europe. November-December 2015:57-64.
2. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95:335-339.
3. Vestergaard A, Ivarsen AR, Asp S, Hjortdal JO. Small-incision lenticule extraction for moderate to high myopia: predictability, safety, and patient satisfaction. J Cataract Refract Surg. 2012;38:2003-2010.
4. Sekundo W, Gertnere J, Bertelmann T, Solomatin I. One-year refractive results, contrast sensitivity, high-order aberrations and complications after myopic small-incision lenticule extraction (ReLEx SMILE). Graefes Arch Clin Exp Ophthalmol. 2014;252(5):837-843.
5. Ivarsen A, Hjortdal J. Correction of myopic astigmatism with small incision lenticule extraction. J Refract Surg. 2014;30:240-247.
6. Riau A, Ang H, Lwin N, Chaurasia S, Tan D, Mehta J. Comparison of four different VisuMax Circle patterns for flap creation after small incision lenticule extraction. J Refract Surg. 2013;29:236-244.
7. Sinha Roy A1, Dupps WJ Jr1, Roberts CJ. Comparison of biomechanical effects of small-incision lenticule extraction and laser in situ keratomileusis: finite-element analysis. J Cataract Refract Surg. 2014;40(6):971-980.
8. Reinstein DZ, Srivannaboon S, Gobbe M, et al. Epithelial thickness changes induced by myopic LASIK as measured by Artemis very high frequency digital ultrasound. J Refract Surg. 2009;25:444-450.
9. Donate D, Thaëron R. Preliminary evidence of successful enhancement after a primary SMILE procedure with the sub-cap-lenticule-extraction technique. J Refract Surg. 2015;31(10):708-710.
David Donate, MD
• Private practice, Ophteo, Lyon, France
• david.donate@yahoo.fr
• Financial disclosure: Consultant (Carl Zeiss Meditec)
Rozenn Thaëron, OD
• Optometrist, Ophteo, Lyon, France
• rozenn.thaeron@gmail.com
• Financial interest: None acknowledged
