
Getting to Know the Patient
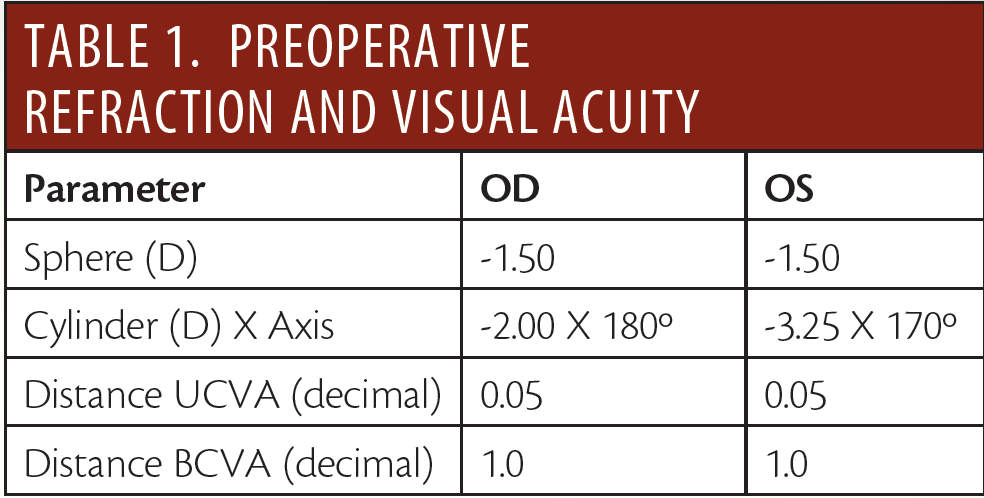
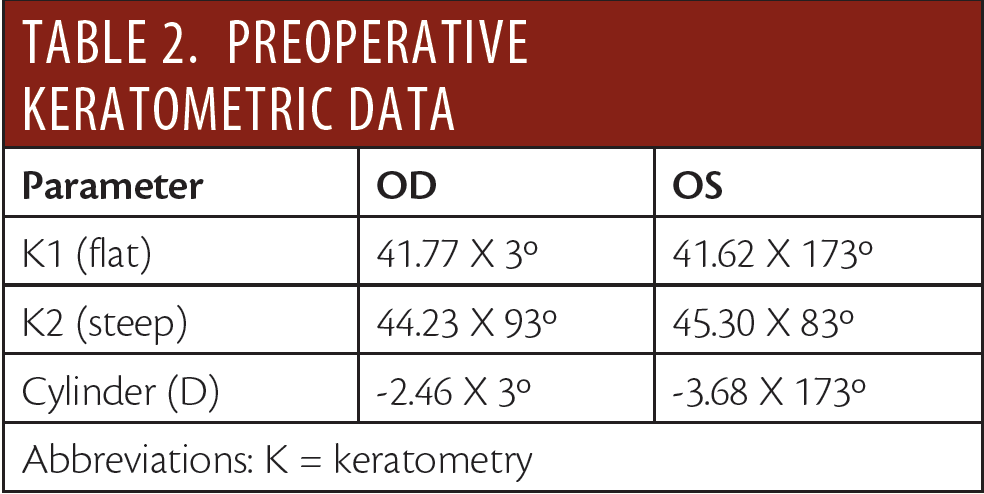
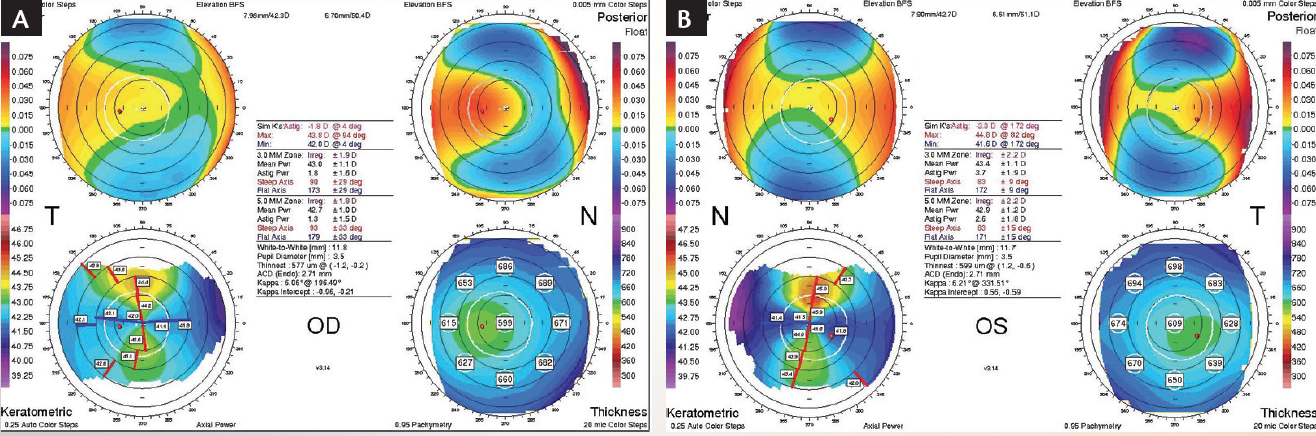
Figure 1. Preoperative anterior corneal topography of the right (A) and left (B) eyes.


For many years, it has been recognized that there may be a difference between refractive astigmatism and anterior corneal astigmatism. Historically, this difference was mainly blamed on lenticular astigmatism, which it has not been possible to measure with conventional methods. Recently, thanks to new corneal measuring devices, several studies have shown that posterior corneal astigmatism can significantly influence total corneal astigmatism, and, therefore, measurement of posterior corneal astigmatism can help to improve the accuracy of toric IOL power selection in certain cases. The patient described in Getting to Know the Patient is one such case.
Calculations for the toric IOL (Lentis Tplus; Oculentis) to be implanted in this patient were performed using keratometry readings obtained with the IOLMaster. The IOL implanted in the patient’s right eye was a model LS-313 with spherical equivalent of 15.50 D and cylinder of 3.00 D. With this lens, predicted residual astigmatism was 0.01 X 93º. The lens for the patient’s left eye was again a model LS-313 with 15.50 D spherical equivalent and cylinder of 4.50 D. Predicted residual astigmatism for this eye was 0.06 X 84º.
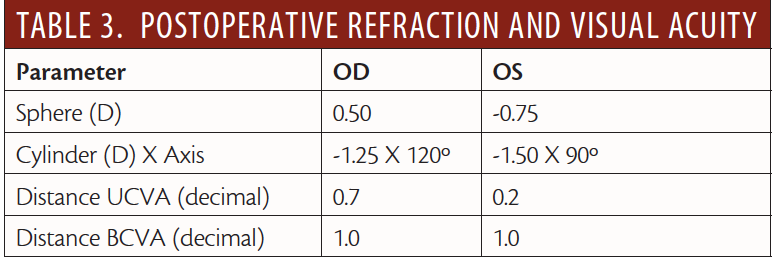
Both surgeries and the immediate postoperative periods were completed with normal results and no complications. The IOLs appeared to be perfectly aligned on mydriasis. During follow-up, however, the patient expressed discontent with his visual acuity without correction, especially for distance vision (Table 3).
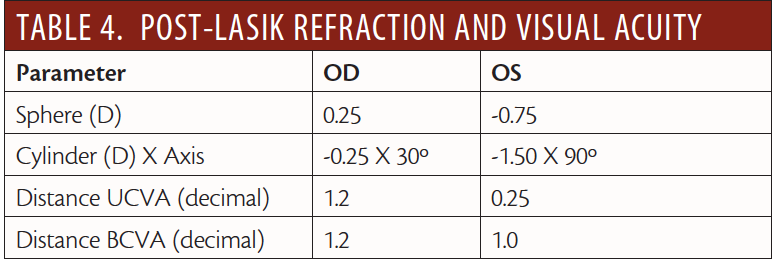
The patient underwent femtosecond LASIK in his right eye to achieve emmetropia and meet the initially proposed objective of spectacle independence at all distances. During the post-LASIK follow-up, the patient affirmed that he now performs most of his activities of daily life without any spectacle correction. Refraction and visual acuities 1 month after LASIK are shown in Table 4.
FACTORS THAT CONTRIBUTE TO
A REFRACTIVE SURPRISE
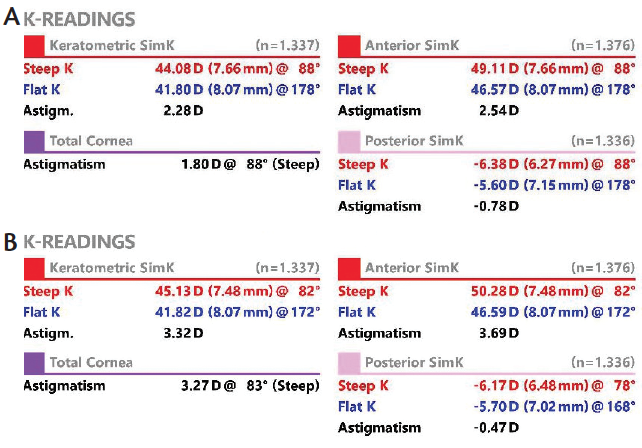
Figure 2. Keratometric data of the patient’s right (A) and left (B) eyes.
The development of toric IOLs has improved refractive results in cataract surgery for patients with significant astigmatism.1 However, residual astigmatism after implantation of toric IOLs is not always predictable,2 and unsatisfactory UCVA can be a postoperative outcome. Several factors may contribute to an astigmatic refractive surprise, including imprecise corneal measurements, miscalculation of the toric IOL power, error in the preoperative marking of the cornea, misalignment of the IOL, and the effect of the incision.3-6 In the case presented here, one factor that might have reduced residual astigmatism was adjustment of the IOL toricity based on the patient’s posterior corneal astigmatism.
The surfaces of the anterior and posterior cornea each contribute to the total corneal astigmatism. Studies have indicated that posterior corneal astigmatism contributes significantly to total corneal astigmatism7 and that its effect may vary from -0.26 to -0.78 D.7-14
Posterior corneal astigmatism in most patients is relatively stable, and almost 80% is vertical, or with-the-rule.7 This may contribute toward overcorrection of with-the-rule and undercorrection of against-the-rule astigmatisms, if posterior corneal astigmatism is not taken into account.
Case Recap
Who
60-year-old man with myopic astigmatism and a desire for spectacle independence at all distances after cataract surgery
What
Refractive cataract surgery using a micro-monovision strategy (targets: emmetropia in the dominant right eye and -1.00 D in the left) and implantation of a toric IOL left the patient with a residual refractive error that affected his distance vision
How
LASIK retreatment in the patient’s right eye resolved the residual refractive error; however, if posterior corneal astigmatism had been measured preoperatively and accounted for in the toric IOL power calculation, the need for enhancement may have been avoided
In our case presented here, we saw a significant difference in refractive and keratometric astigmatisms, which could have meant a greater influence of posterior corneal astigmatism on the total astigmatism. After observing this refractive surprise, we performed topography with the Cassini (i-Optics) to measure the astigmatism of the posterior corneal face (Figure 2). This confirmed our suspicion that the patient had a greater degree of posterior astigmatism than is usual.
A study of error in residual astigmatism prediction after implantation of toric IOLs did not find a significant difference whether the calculation of toricity was done based on total corneal power (as determined by ray-tracing Scheimpflug topography) or with the values of anterior automated keratometry.14 However, particularly in our case, it is evident that the overcorrection of astigmatism could have been reduced if the calculation had been done using the astigmatic value provided by the Cassini topographer.
Since the Baylor nomogram was published by Koch et al,7 multiple formulas have been proposed to reduce residual astigmatism after implantation of toric IOLs, and there is currently a lack of clear consensus on the best formula to use. It has recently been proposed that lower residual astigmatism can be achieved by using vector analysis, which is performed by integrating the posterior corneal astigmatism as measured by Scheimpflug camera with the anterior corneal astigmatism as measured by low-coherence optical reflectometry.15
LESSONS LEARNED
Surgeons may be able to minimize residual astigmatism after implantation of toric IOLs by taking posterior corneal astigmatism into consideration, especially in eyes in which there is a remarkable difference between the refractive astigmatism and the keratometric astigmatism. Had we done so in the case presented here, a retreatment procedure may likely have been avoidable.
1. Agresta B, Knorz MC, Donatti C, Jackson D. Visual acuity improvements after implantation of toric intraocular lenses in cataract patients with astigmatism: a systematic review. BMC Ophthalmol. 2012;12:41.
2. Alpins N, Ong JKY, Stamatelatos G. Refractive surprise after toric intraocular lens implantation: graph analysis. J Cataract Refract Surg. 2014;40:283-294.
3. Hirnschall N, Hoffmann PC, Draschl P, Maedel S, Findl O. Evaluation of factors influencing the remaining astigmatism after toric intraocular lens implantation. J Refract Surg. 2014;30:394-400.
4. Browne AW, Osher RH. Optimizing precision in toric lens selection by combining keratometry techniques. J Refract Surg. 2014;30:67-72.
5. Hill W, Potvin R. Monte Carlo simulation of expected outcomes with AcrySof toric intraocular lens. BMC Ophthalmol. 2008;8:22.
6. Huang J, Pesudovs K, Wen D, Chen S, Wright T, Wang X, Li Y, Wang Q. Comparison of anterior segment measurements with rotating Scheimpflug photography and partial coherence reflectometry. J Cataract Refract Surg. 2011;37:341-348.
7. Koch DD, Ali SF, Weikert MP, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38:2080-2087.
8. Royston JM, Dunne CMM, Barnes DA. Measurement of posterior corneal surface toricity. Optom Vis Sci. 1990;67:757-763.
9. Dunne MCM, Royston JM, Barnes DA. Posterior corneal surface toricity and total corneal astigmatism. Optom Vis Sci. 1991;68:708-710.
10. Ho J-D, Tsai C-Y, Liou S-W. Accuracy of corneal astigmatism estimation by neglecting the posterior corneal surface measurement. Am J Ophthalmol. 2009;147:788-795.
11. Dubbelman M, Sicam VA, van der Heijde GL. The shape of the anterior and posterior surface of the aging human cornea. Vision Res. 2006;46:993-1001.
12. Prisant O, Hoang-Xuan T, Proano C, Hernandez E, Awwad ST, Azar DT. Vector summation of anterior and posterior corneal topographical astigmatism. J Cataract Refract Surg. 2002;28:1636-1643.
13. Modis L Jr, Langenbucher A, Seitz B. Evaluation of normal corneas using the scanning-slit topography/pachymetry system. Cornea. 2004;23:689-694.
14. Zhang L, Sy ME, Mai H, Yu F, Hamilton DR. Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(1):84-89.
15. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: Comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217-225.
Daniel Elies, MD
• Cornea and Refractive Surgery Specialist, Instituto de Microcirugia Ocular, Barcelona, Spain
• Associate Professor of Ophthalmology, ESASO University, Lugano, Italy
• elies@imo.es
• Financial interest: None acknowledged
Jose L. Güell, MD, PhD
• Director, Cornea and Refractive Surgery Unit, Instituto de Microcirugía Ocular, Barcelona, Spain
• Associate Professor of Ophthalmology, Universitat Autonoma de
• guell@imo.es
• Financial disclosure: Consultant (Ophtec, Alcon, Carl Zeiss Meditec, Thea Laboratories, Orca Surgical), Partial owner (Calhoun Vision, Visiometrics)
Pablo Laso, MD
• Fellow, Cornea and Refractive Surgery Unit, Instituto de Microcirugía Ocular, Barcelona, Spain
• pablo.laso.u@gmail.com
• Financial interest: None acknowledged
Mercé Morral, MD, PhD
• Cornea and Refractive Surgery Specialist, Instituto de Microcirugia Ocular, Barcelona, Spain
• morral@imo.es
• Financial interest: None acknowledged
Fernando Santander, MD, FEBO
• Fellow, Cornea and Refractive Surgery Unit, Instituto de Microcirugia Ocular, Barcelona, Spain
• fsantandert@gmail.com
• Financial interest: None acknowledged
