
Getting to Know the Patient


The patient described above was counseled that he might need some mild correction after cataract surgery for the clearest possible distance vision. It was also explained that, with his history of RK, his astigmatism could be corrected with a toric IOL, but the clarity of his vision might not be as crisp as it was currently with his RGP contact lenses. He stated that his vision in spectacles was adequate and nearly equivalent to his RGP contact lenses, and that he wanted independence from the hard contacts, if possible. The patient was also counseled that, due to his RK, he might have some variability in his postoperative refraction for several weeks after surgery.
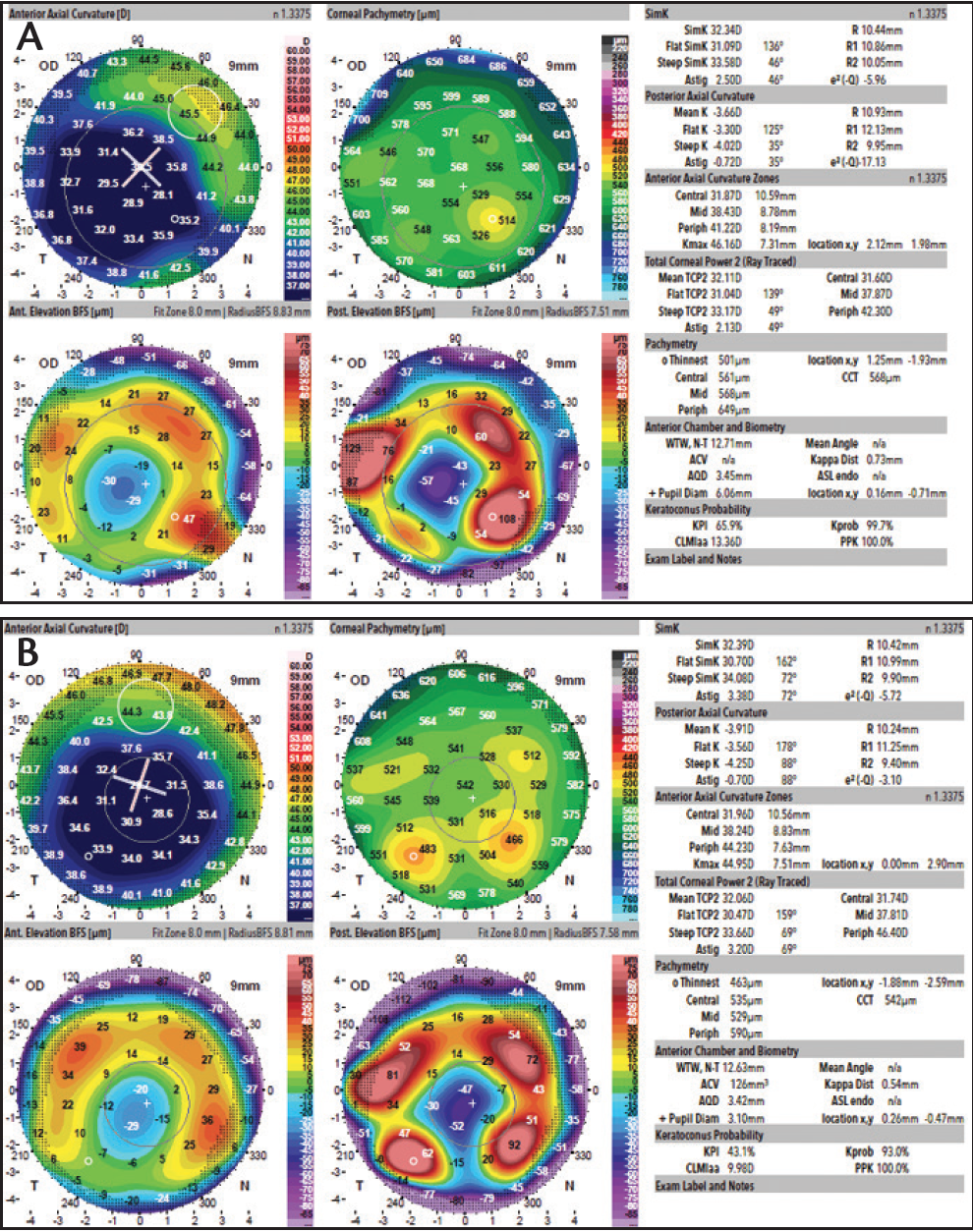
Figure 1. In the patient’s right eye, multiple topography captures (A, B) showed simKs ranging from 30.98 to 32.39 D and corneal astigmatism values ranging from 2.57 to 4.50 D at axes ranging from 42° to 60°.
PREOPERATIVE MEASUREMENTS
In preoperative testing for the right eye, axial length was 25.67 mm. The IOLMaster (Carl Zeiss Meditec) showed a simulated keratometry (simK) reading of 32.52 D with 3.34 D of astigmatism at 18°. Multiple captures with the Galilei topographer (Ziemer Ophthalmic Systems; Figure 1) showed simKs ranging from 30.98 to 32.39 D and corneal astigmatism values ranging from 2.57 to 4.50 D at axes ranging from 42° to 60°.
Topography with the Cassini topographer (i-Optics; Figure 2) demonstrated a simK of 28.70 D with 4.66 D of astigmatism at 51°.
Preoperative testing for the left eye revealed an axial length of 25.93 mm. The IOLMaster showed a simK reading of 32.52 D with 2.70 D of astigmatism at 113°. Multiple captures with the Galilei topographer (Figure 3) showed simKs ranging from 34.76 to 35.68 D and corneal astigmatism values ranging from 2.77 to 3.76 D at axes from 114° to 135°.
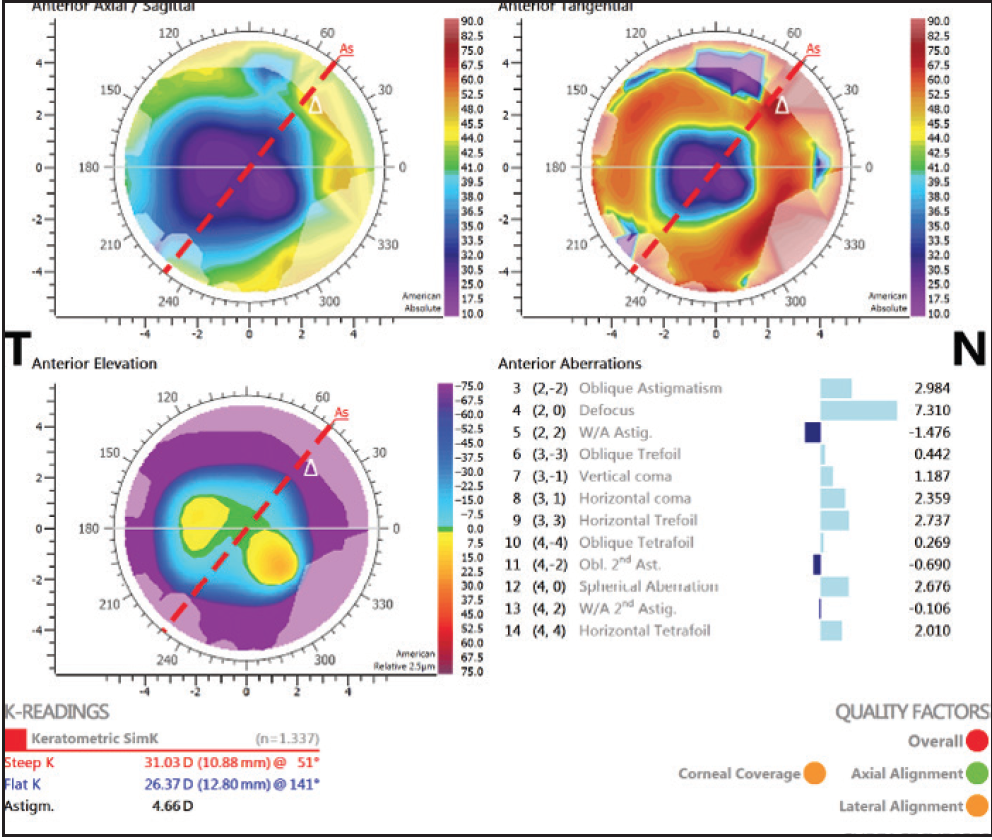
Figure 2. In the patient’s right eye, topography demonstrated a simK of 28.70 D with 4.66 D of astigmatism at 51°.
Topography with the Cassini topographer (Figure 4) demonstrated a simK of 31.74 D with 3.57 D of astigmatism
at 126°.
Right eye: IOL CHOICE AND SURGERY
Several IOLs were considered for the patient’s right eye and were narrowed down to two choices.
Choice No. 1: Monofocal spherical IOL. The patient was an RGP contact lens wearer, so a monofocal spherical IOL would allow him to continue to wear his RGP lenses.
Choice No. 2: Toric IOL. The patient’s desire to be free of his RGP lenses and his tolerance of spectacles suggested that a toric IOL would be a better choice for him. His corneal cylinder was relatively consistent in axis and power, although there was some variability.
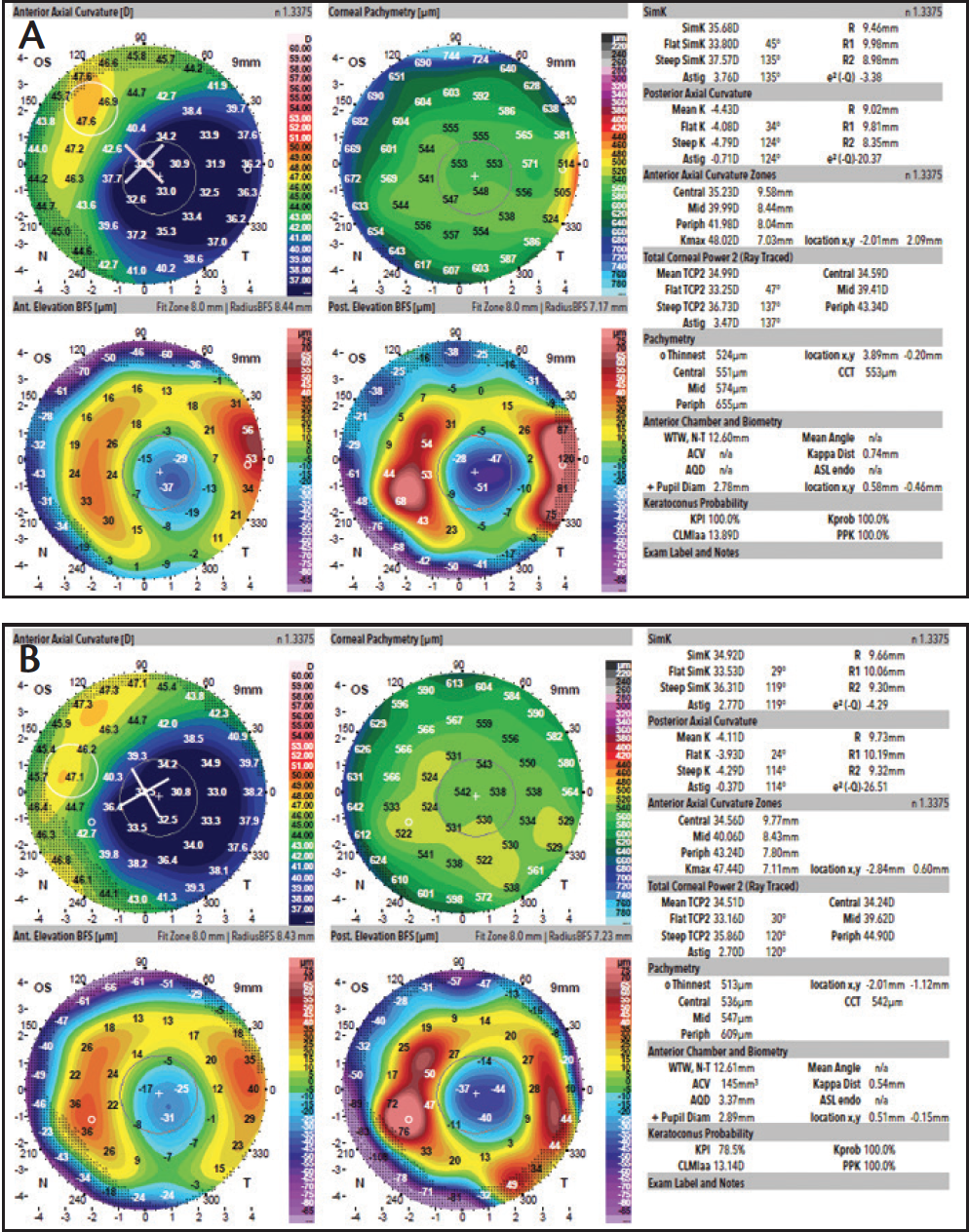
Figure 3. In the patient’s left eye, multiple topography captures (A, B) showed simKs ranging from 34.76 to 35.68 D and corneal astigmatism values ranging from 2.77 to 3.76 D at axes from 114° to 135°.
Decision. A toric IOL was determined to be the best choice to meet the patient’s goals. However, the power of the IOL was difficult to choose based on the variability of the simK on topography.
As part of our decision process, we performed IOL calculations using the flattest keratometry (K) values at the 3-mm optical zone on topography. Ultimately, the IOL power for the right eye was calculated using the IOLMaster K values (which were consistent with some of the Galilei simKs) with the Holladay 2 formula. The Cassini K values for the right eye were thought to be inaccurate, as they were significantly flatter than any of the other K values measured.
An AcrySof IQ Toric IOL (Alcon) with a power of 27.00 D and add of 4.50 D was selected for implantation in the patient’s right eye. The case was uneventful, and the IOL was successfully placed into the capsular bag. We attempted to use intraoperative aberrometry with the ORA System (Alcon) during the surgery, but a reading could not be obtained due to the irregularity of the cornea after RK. The toric IOL was implanted at an axis of 45°, as this appeared to be the most accurate alignment based on multiple topographies and was the recommendation of the live ORA readings.
BACK TO THE DRAWING BOARD
On postoperative day 1, visual acuity in the patient’s right eye was count fingers at 5 feet with a clear cornea, and manifest refraction revealed a refractive error of 6.75 D. The patient was seen again at 1 week postoperative. At this visit, his UCVA was 20/400, and a BCVA of 20/25 was obtained with a manifest refraction of 5.75 D. We discussed with the patient the options of IOL exchange or piggyback IOL insertion, and the piggyback IOL was chosen.
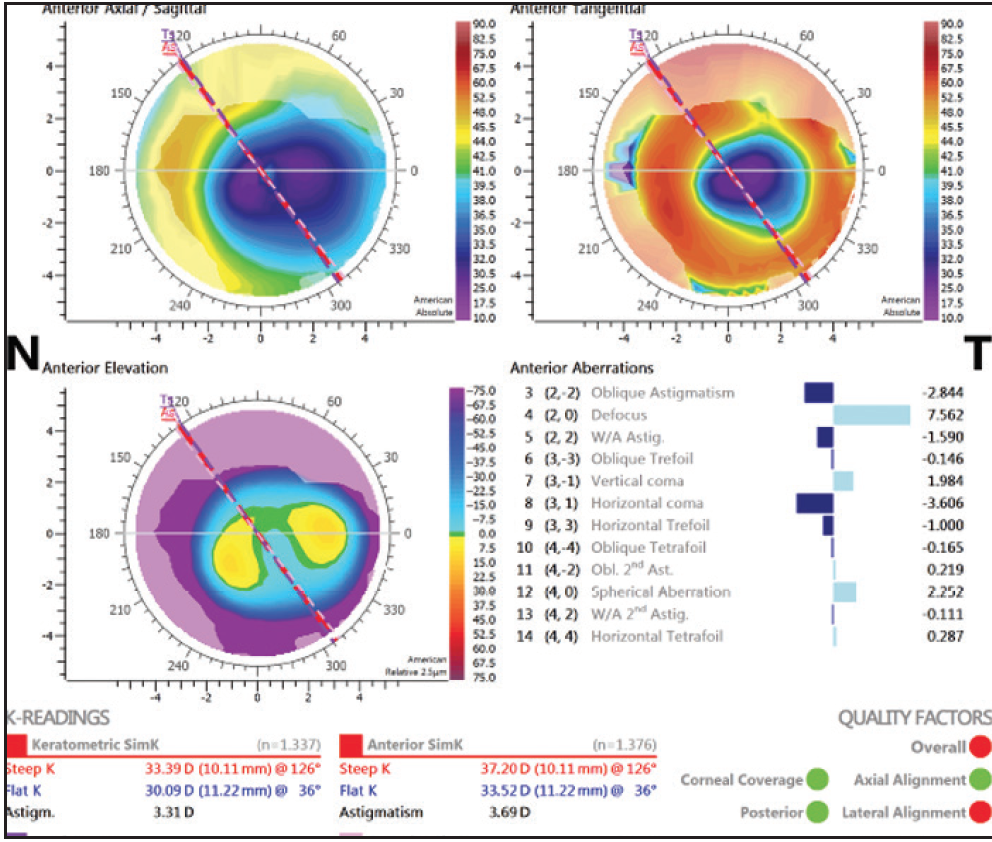
Figure 4. In the patient’s left eye, topography demonstrated a simK of 31.74 D with 3.57 D of astigmatism at 126°.
Based on the patient’s manifest refraction, it was determined that an additional 9.00 D of power would be required at the sulcus in order to completely correct his residual hyperopia. The surgery was uneventful, and a LI61AO (Bausch + Lomb) 9.00 D silicone IOL was placed in the sulcus. On postoperative day 1, the patient was 20/40 with a manifest refraction of +0.75 +0.25 X 110° yielding a BCVA of 20/30+. The patient was happy and wanted to proceed with surgery in his left eye.
LEFT EYE: IOL CHOICE AND SURGERY
For the patient’s left eye, the strongest AcrySof IQ Toric IOL power available was 30.00 D with an add of 3.75 D. Piggyback IOLs ranging in power from 1.00 to 5.00 D were made available for surgery, and the final choice was to be made based on intraoperative aberrometry.
Because of the slightly hyperopic manifest refraction in the patient’s right eye, the plan was also to aim slightly myopic for the left. The surgery was uneventful. Once again, ORA was unable to make an aphakic IOL power recommendation. The toric IOL was implanted at an axis of 114°.
Case Recap
Who
61-year-old man with a history of RK in each eye and laser touch-up in his right eye, presenting with a chief complaint of increasing glare and halos at night; with his current prescription (+8.75 +2.00 X 17° OD; +6.00 +2.25 X 126° OS), visual acuity was 20/40+2 OD, 20/25+2 OS, and 20/80 OU
What
Astigmatism correction with a toric IOL, with the goal of leaving the patient independent from hard contact lenses if possible
How
Implantation of a toric IOL with a power of 27.00 D and add of 4.50 D left the patient with poor visual acuity in the right eye postoperatively; a piggyback IOL with an additional 9.00 D of power was implanted in the sulcus in order to completely correct his residual hyperopia
At the postoperative day 1 visit, the patient had a UCVA of 20/30 OU, with near UCVA of J7 OD and J5 OS. At the postoperative 2-week visit, the patient had a UCVA of 20/30+2 OD and 20/25- OS, and he was happy with his outcome. Manifest refraction revealed a mild residual refractive error of +0.75 + 0.75 X 133° OD and -1.00 +1.75 X 165° OS.
LESSONS LEARNED
There are several important lessons to be learned from this case. In patients with previous RK, we will now be much more likely to select IOL powers based on the flattest K values when using the Holladay 2 formula. In general, we now prefer to use the IOLMaster K values with the Haigis formula for eyes after myopic LASIK or RK.
In the case described here, with the flat Ks obtained from the Cassini topographer, the IOL power for the patient’s right eye would have been between 32.00 to 34.50 D based on the Holladay 2 formula, which is significantly stronger that the 27.00 D toric IOL that was selected.
It is also important to note that, with proper counseling, even patients who are wearing RGP contact lenses after RK can be viable candidates for toric IOL implantation, as long as the degree and axis of astigmatism are relatively uniform and the patients can tolerate spectacle correction.
Chad Hummel, MD
• Fellow, The Eye Institute of West Florida, Largo, Florida
• chadhum@gmail.com
• Financial interest: None acknowledged
Robert J. Weinstock, MD
• Private practice, The Eye Institute of West Florida, Largo, Florida
• rjweinstock@yahoo.com
• Financial disclosure: Consultant (Alcon)
