

The 21st century has been a time of substantial paradigm shifts, especially when it comes to the emerging uses of information and communication technologies (ICTs) in health care. ICTs have proven to be greatly valuable for addressing challenges faced by both developed and developing countries in providing accessible, cost-effective, and high-quality health care services. They have also redefined or created new practice styles or delivery models encompassed within the term telehealth that are proving to be beneficial for the patient community.
AT A GLANCE
• Telehealth is a multidimensional concept that may differ depending on the context, region, country, or time in which it is applied.
• Lessons learned by the leaders at Instituto Zaldivar indicate that issues related to organizational change management must be taken into consideration when deciding to implement a virtual clinic.
• Building a telehealth clinic requires an interdisciplinary and collaborative approach, with an integrated vision of being able to provide cost-effective and quality services, regardless of the technology applied.
Today, telehealth can be considered a multidimensional concept that may differ depending on the context, region, country, or time in which it is applied. Bashshur et al defined teleheath as “a paradigmatic and disruptive concept where the new [health care] delivery modality challenges the traditional sine qua non dependence on physical presence and contact between providers and patients.”1
Under this model, the use of video communications in examining patients has propelled us into a new dimension of patient care.
VISUAL COMMUNICATIONS
As Edward R. Tufte stated, “To envision information—and what bright and splendid visions can result—is to work at the intersection of image, word, number, [and] art.” The use of videos together with images, diagrams, graphs, and other visual interpretations of material can help bring together the visual and the verbal to add another dimension and create a new path toward understanding, or seeing, its meaning.2
In ophthalmology, we have found this to be quite true. For the past 20 years, leaders at the Instituto Zaldivar have firmly believed in the power of visual communications, and they have used it to the benefit of patient outreach, integrating visual communication technologies such as its legacy videoconferencing systems with new high-quality pervasive video, video-over-Internet-protocol telephony, and multimedia educational applications.
Increased access to these tools has enabled the institute to set up cost-effective outreach programs and allow telescreening applications, clinical patient services, and second opinions to enrich our service portfolio. Our aims have been not only to improve patient care and strengthen our referral models but also to provide continuing education for all personnel, including attending physicians, residents, nurses, and other allied health care employees and to potentiate our foundation’s community eye care awareness campaigns.
In order to accomplish this, in the 1990s, we established our presence on the then-new World Wide Web, followed by the deployment of our teleophthalmlogy program in 2001. At the time, our main goal was to overcome the geographic barriers between our patients and care centers during a profound social, political, and economic crisis in Argentina. To do so, we linked our hub and spoke sites in real time with videoconferencing, and digital imaging management tools and electronic health record (EHR) data were partially integrated into our health information system.
In the following years, innovations in the video communication and web-enabled technology industry led us to redesign our network. The acquisition of telepresence solutions allowed us to develop the pervasive experience of a virtual in-person encounter.

Figure 1. A virtual consultation at Instituto Zaldivar, showing views of Roger Zaldivar, MD (A), Dr. Ricur (B), and the patient (C).
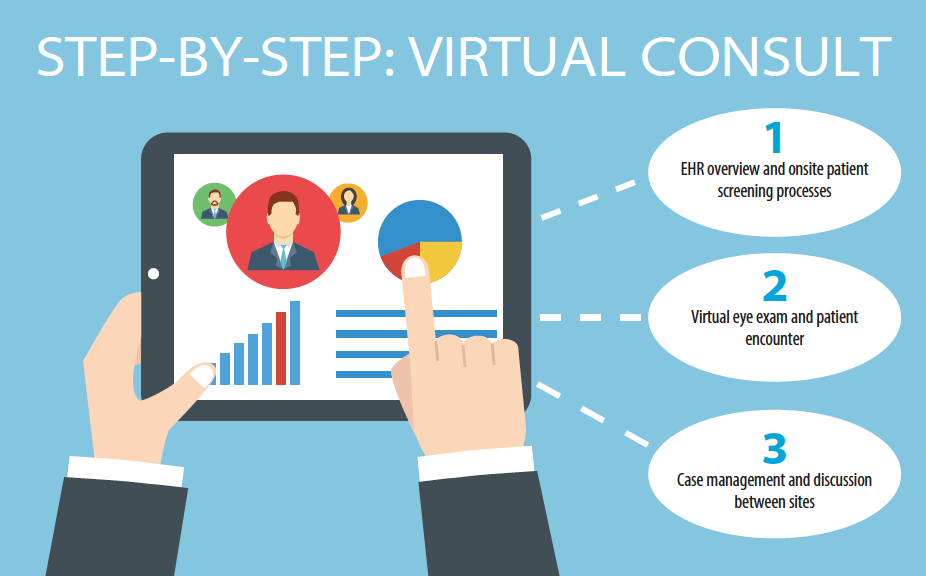
In 2012, we created a service based on high-quality video and audio capability in a collaborative environment that we termed TP Consults. Telepresence suites were built in Mendoza and Buenos Aires to ensure that physicians and patients could see each other in life-size images on 65-inch high-definition plasma screens (Figure 1), and we redefined our standard operating procedures or protocols for seeing cataract and refractive patients. A three-step pathway was established, consisting of: (1) an EHR overview and onsite patient screening process, (2) a virtual eye exam and patient encounter, and (3) case management and discussion between sites. Formal training, role playing, and coaching initiatives were undertaken to troubleshoot and support users during the adoption phase.
BENEFITS AND CHALLENGES
Soon enough, patients started benefiting from TP Consults. Their access to our innovative eye care services was improved, and waiting lists for appointments were reduced. TP Consults also facilitated postoperative remote monitoring, and, thus, patients could avoid unnecessary trips to our hub in Mendoza. Both factors resulted in savings of patients’ time and money.
We also targeted improving patient satisfaction; in turn, the numbers of consults grew as increased loyalty and attraction of new patients occurred, and more patients were willing to pay, leading to increased earnings for the practice. Additionally, costs were tapered, as monthly staff travel to and training at the remote sites was reduced.

A recent study published by IHS Technology revealed that physicians’ virtual consults with patients are expected to double by 2020, with total numbers of virtual consults growing 10% per year. Specialty consultations are projected to jump from 14.5 million to 21.5 million.3
Our experience shows that we are following the same trend: In 2013, 531 cataract and refractive consultations were performed, and this increased 16% the following year (629 virtual consults) and 39% by the end of November 2015 (1,031 virtual consults). Of these encounters, more than 26% of the virtual consults led to surgeries.
TECHNOLOGY DOES NOT OPERATE ON ITS OWN
Developing and implementing a successful quality telehealth program is no easy endeavor. We strongly believe that the unique challenge of this health care modality is defying the paradigm of traditional in-person encounters. Although avant-garde technology such as telepresence solutions can undoubtedly help overcome this, the human factor remains our main goal for change management.
In other words, lessons learned indicate that one must take into consideration all of the issues related to organizational change management when deciding to implement a virtual clinic. Top-level institutional commitment must be warranted before the startup phase is initiated. Capacity building and team building are crucial keys to success, and they must be taken into account when the strategic plan is designed. All necessary resources should be allocated to provide for this.
This not only applies to interdisciplinary staff hiring and training but also should include identifying staff champions who will readily adopt this new modus operandi of seeing patients or training and help to create synergy among the rest of the newly appointed team. Additionally, troubleshooting and supporting the users during the entire process is as crucial as identifying the proper technology for the applications to be used.
After the organizational aspects have been managed, the team should decide on the scope and modality of the programs that will be offered. This will affect the design of the telecommunications network; the selection and acquisition of the proper technology; the needs for training; and the design of all the processes, procedures, and monitoring that will support the ocular telehealth programs in a validated and structured format.
SUMMARY
Building a telehealth clinic requires an interdisciplinary and collaborative approach, with an integrated vision of being able to provide cost-effective and quality services, regardless of the technology applied. Proper introduction and change management is required when innovative technologies are adopted into an eye clinic’s regular workflow. In our case, continuous analysis of the business model is required, due to constant political and economic changes in Argentina. Regardless, physician and patient satisfaction will always be the key elements required to ensure a successful virtual visual encounter.
1. Bashshur R, Shannon G, Krupinski E, Grigsby J. The taxonomy of telemedicine. Telemed J E Health. 2011;17(6):484-494.
2. Tufte ER. Envisioning Information. Cheshire, CT: Graphics Press; 1990.
3. Roashan R. Telehealth & Remote Patient Monitoring Report – 2015. IHS Technology. July 31, 2015.
Giselle Ricur, MD
• Director, Telemedicine Program, Instituto Zaldivar, Mendoza, Argentina
• giselle.ricur@institutozaldivar.com
• Financial interest: None acknowledged
