
Iris-fixated IOLs, positioned either anterior or posterior to the iris plane, are an alternative to scleral-fixated posterior chamber IOLs or angle-fixated anterior chamber IOLs, with several advantages. Specifically, although scleral fixation of a posterior chamber IOL preserves the ocular anatomy, the surgical procedure is complex, with potentially severe complications, extended surgical time, and a long learning curve.1 Implantation of anterior chamber IOLs is more straightforward; however, these IOLs can cause endothelial cell loss, bullous keratopathy, and secondary glaucoma.2
AT A GLANCE
• Several published reports have demonstrated excellent results in terms of good visual outcome, low postoperative complication rates, and low endothelial cell loss with posterior positioning of iris-fixated IOLs.
• The main benefits of retroiridial implantation of an iris-fixated IOL are greater preservation of the ocular anatomy, which results in better optical correction, and a greater distance
Because positioning an IOL anterior to the iris can cause problems with the corneal endothelium and angle structures, posterior positioning of iris-fixated IOLs has been advocated by some authors in both adult and pediatric populations.3,4 With this retroiridal approach, not only is the eye’s original anatomy better preserved, but also positioning the IOL at a greater distance from the cornea minimizes damage to the endothelium. Studies have demonstrated endothelial cell loss of between 10.5% and 10.9% with anterior positioning of iris-fixated lenses.5,6
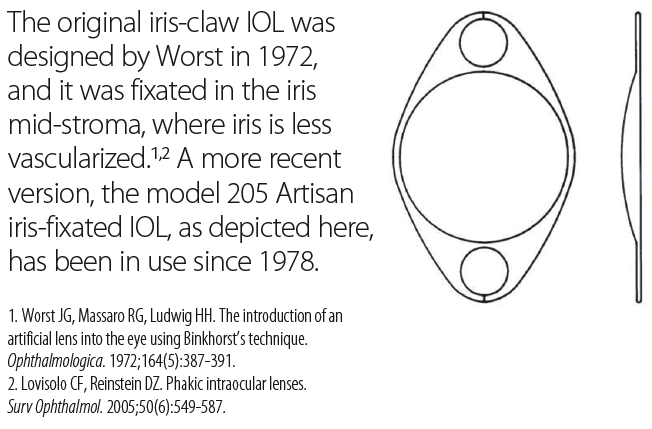
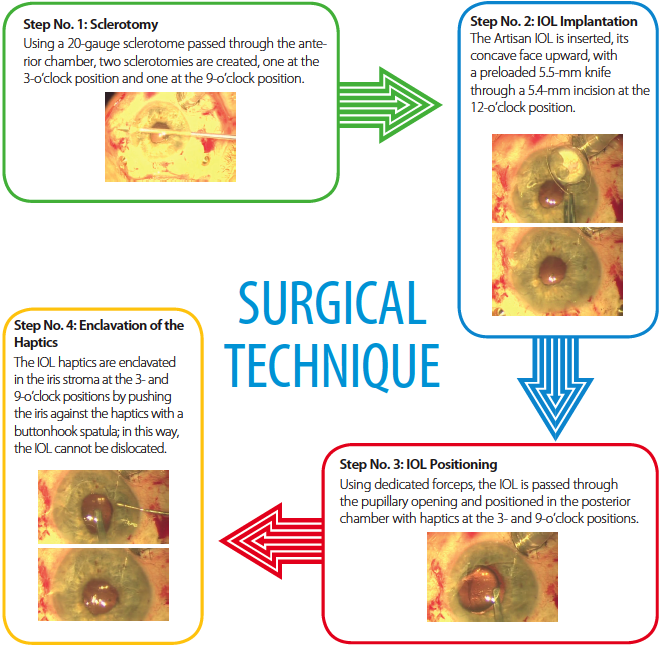
In the accompanying diagram, Surgical Technique, we describe a method for implantation of an iris-fixated IOL (Artisan Aphakia IOL; Ophtec) in the posterior chamber. This IOL is most often used when suitable capsular support is not available; however, it also may be used when IOL subluxation occurs after cataract surgery or when the capsular bag breaks due to trauma, causing damage to the zonular structures that results in lens subluxation. Thus far, we have performed this technique in three patients who could not undergo capsular bag implantation due to earlier traumatic cataract with capsular rupture and zonular disinsertion.
GOOD RESULTS WITH POSTERIOR POSITIONING
Several published reports have demonstrated excellent results in terms of good visual outcome, low postoperative complication rates, and low endothelial cell loss with posterior positioning of iris-fixated IOLs. Brander et al reported outcomes using retroiridial positioning with these IOLs in a population of 15 pediatric eyes.3 Gonnerman et al also used this procedure in pediatric patients, and they reported their results with 3 years of follow-up.7,8 According to these authors, this technique was safe and effective, with excellent visual outcomes and a low rate of complications in pediatric eyes.
Anbari and Lake reported results with 2 years of follow-up in adult patients who underwent iris-fixated IOL implantation behind the iris. The safety and, in particular, the preservation of corneal endothelial cells with this technique were ascertained. These authors noted the need for a new A-constant for more accurate IOL power calculation with retroiridial positioning.4 Another study, by Schallenber et al, stressed the lack of corneal decompensation signals in 31 patients who underwent iris-claw IOL implantation behind the iris.9
CONCLUSION
The surgical technique we described here is not more difficult, from a technical point of view, than the insertion of an anterior chamber angle-fixated IOL. It is certainly easier than scleral fixation, which is time-consuming and demanding. The main benefits of our technique are greater preservation of the ocular anatomy, which results in better optical correction, and a greater distance between the IOL and the corneal endothelium. Of course, larger studies with longer follow-up are needed for better evaluation of the long-term benefits and final outcomes with this technique. n
1. Kwong YY, Yuen HK, Lam RF, et al. Comparison of outcomes of primary sclera-fixated versus primary anterior chamber intraocular lens implantation in complicated cataract surgeries. Ophthalmology. 2007;114(1):80-85.
2. Sawada T, Kimura W, Kimura T, et al. Long-term follow-up of primary anterior chamber intraocular lens implantation. J Cataract Refract Surg. 1998;24(11):1515-1520.
3. Brandner M, Thaler-Saliba S, Plainer S, et al. Retropupillary fixation of iris-claw intraocular lens for aphakic eyes in children. PLoS One. 2015;10(6):e0126614.
4. Anbari A, Lake DB. Posteriorly enclavated iris claw intraocular lens for aphakia: long-term corneal endothelial safety study. Eur J Ophthalmol. 2015;25(3):208-213.
5. Koss MJ, Kohnen T. Intraocular architecture of secondary implanted anterior chamber iris-claw lenses in aphakic eyes evaluated with anterior segment optical coherence tomography. Br J Ophthalmol. 2009;93(10):1301-1306.
6. Gȕell JL, Velasco F, Malecaze F, et al. Secondary Artisan-Verysise aphakic lens implantation. J Cataract Refract Surg. 2005;3(12):2266-2271.
7. Gonnermann J, Torun N, Klamann MK, et al. Posterior iris-claw aphakic intraocular lens implantation in children. Am J Ophthalmol. 2013;156(2):382-386.
8. Gonnermann J, Amiri S, Klamann M, et al. Endothelial cell loss after retropupillary iris-claw intraocular lens implantation. Klin Monbl Augenheilkd. 2014;231(8):784-787.
9. Schallenberg M, Dekowski D, Hahn A. Aphakia correction with retropupillary fixated iris-claw lens (Artisan) – long term results. Clin Ophtalmol. 2014;8:137-141.
Giulio Maione, MD
• Carlo Poma Hospital, Mantova, Italy
• oculisticamaione@gmail.com
• Financial interest: None acknowledged
Giuseppe Sciuto, MD
• Carlo Poma Hospital, Mantova, Italy
• giuseppesciuto@aopoma.it
• Financial interest: None acknowledged
Paolo Trabucco, MD
• Carlo Poma Hospital, Mantova, Italy
• paolotrabucco@libero.it
• Financial interest: None acknowledged
