

In a refractive surgery procedure that involves flap creation, whether with a microkeratome or a femtosecond laser (namely, LASIK), it makes sense to perform CXL at the same time. This approach, dubbed LASIK Xtra, certainly has a role in the refractive surgeon’s armamentarium, although it has both clear indications and contraindications.
The biomechanical strength of the cornea decreases when a flap is created. John Marshall, PhD, FRCPath, FRCOphth(Hon), and others have published studies indicating that corneal strength decreases in relation to the thickness of the flap. According to Professor Marshall, an 80- to 90-μm flap causes a 15% decrease in the strength of the cornea, and flaps of 140 μm decrease corneal strength by 25% to 30%.1,2 In my own studies, I have found that corneal resistance factor (CRF) measurements on the Ocular Response Analyzer (Reichert Technologies) decrease by 1 unit with a 100-μm femtosecond laser flap and by 2 units with a 100-μm microkeratome flap.
There is no doubt that CXL increases the strength of the cornea.3,4 In the majority of corneas in which a flap is created for excimer laser surgery, the resulting decrease in corneal strength is not drastic enough to produce ectasia; however, logic dictates that, if possible, we should use a procedure that increases the strength of the cornea when a debilitating surgery such as LASIK is performed. The only downside to this would be if the addition of CXL were to change the results of the LASIK surgery. My own studies have suggested that there is no change in the final outcome between LASIK and LASIK Xtra.5 Another study has confirmed this finding.6
INDICATIONS
The combination of CXL and LASIK is not indicated in all patients. Based on my experience, LASIK Xtra may be indicated in the following cases:
- Young LASIK candidates (less than 24 years of age);
- Patients with severe ocular allergies, due to the risk of heavy eye rubbing;
- Patients with completely normal corneas with no signs of keratoconus but with a family history;
- Patients with thin corneas with normal preoperative evaluation (in which risk of ectasia has been ruled out);
- High myopes (requiring large resections);
- Patients who require retreatments, particularly if the thickness of the previous flap is unknown;
- Patients who experienced unexpected thick flap creation during standard LASIK; and
- Patients who experienced unexpected irregular flap creation with variable thickness along its surface.
A. John Kanellopoulus, MD, has stated that, in the peripheral ablation patterns used for hyperopic treatments, CXL locks in the new corneal shape, and, therefore, regression is delayed.7,8
WARNING
It is erroneously believed by some that LASIK Xtra is indicated for the treatment of keratoconus. This procedure is not indicated when keratoconus is detected or when a preoperative evaluation indicates the possibility of ectasia development. In such cases, surface ablation with CXL is the preferred approach.
TECHNIQUE and results
LASIK Xtra is a simple procedure that adds only a few minutes to standard LASIK surgery. After excimer laser ablation is completed, with the flap still lifted, riboflavin (Vibex Xtra; Avedro) is instilled onto the nude stroma for 90 seconds. Then the riboflavin is rinsed out with balanced saline solution, and the flap is repositioned. The cornea is then exposed to UV-A light for 75 seconds, with a total energy of 2.30 J/cm2.
Long-term results are needed to confirm that LASIK Xtra is able to reduce ectasia development in LASIK patients. Because there has been only a few years since its introduction, we are not yet able to prove that LASIK Xtra works to prevent weakening of the cornea or to return the cornea to its preoperative biomechanical strength. Unfortunately, although substantial research has been conducted to find a system that measures the strength of the cornea in an accurate manner, the only available method we have is not accurate and produces some false positive and false negative cases.
The Ocular Response Analyzer is the only system in use today to study the coefficient of hysteresis (CH) and CRF. These two measurements, made preoperatively and postoperatively, can be used to evaluate changes in the biomechanical strength of the cornea. The ideal study, however, would be to treat one eye with CXL and leave the other eye untreated to truly understand the benefit of the procedure. To the best of my knowledge, no study like this has been published.
At my clinic, we compared pre- and postoperative CRF in 50 eyes treated with LASIK Xtra with femtosecond laser flaps. We found that 16 eyes (32%) maintained similar CRFs, eight eyes (16%) had a mean 0.8 unit improvement in CRF, and 26 eyes (52%) had a mean 0.89 unit decrease in CRF. In a previous study of CRF decrease with femtosecond laser–created flaps, 100% had a mean decrease of 1 unit. From this result, it could be deduced that CXL helps to maintain the biomechanical stability of the cornea after LASIK flap creation. Other studies have confirmed this idea.9,10
LASIK XTRA: NO CHANGE IN REFRACTIVE RESULTS
We are in need of better-designed studies and, most important, better methods to accurately measure, predict, and evaluate corneal strength. While we wait the necessary time needed to measure the effectiveness of CXL at the time of LASIK, it is even more important to determine the safety of LASIK Xtra. This would mean no change in the final refractive result, no changes in the nomogram, and no additional complications.
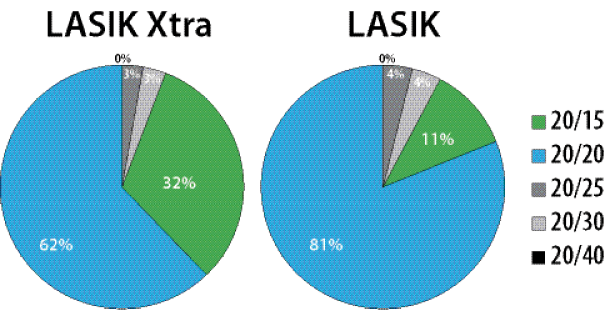
Figure 1. UCVA: One-month results in patients treated with LASIK Xtra or LASIK.
In order to demonstrate this, we conducted a retrospective analysis of results in 66 standard LASIK eyes and 42 LASIK Xtra eyes. Patients were matched for age and refractive defect, and all treatments were performed with femtosecond laser (IntraLase; Abbott Medical Optics) flap creation and with wavefront ablation with the Visx Star S4 IR (Abbott Medical Optics). Figure 1 summarizes the 1-month results.
This study demonstrated that there is no need to make any changes to the nomogram or other factors with LASIK Xtra.
1. Arons I. An Interview with Professor John Marshall. February 11, 2011. http://irvaronsjournal.blogspot.com/2011/02/interview-with-professor-john-marshall.html. Accessed April 20, 2016.
2. Jaycock PD, Lobo L, Ibrahim J, Tyrer J, Marshall J. Interferometric technique to measure biomechanical changes in the cornea induced by refractive surgery. J Cataract Refract Surg. 2005;31(1):175-184.
3. Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66(1):97-103.
4. Seiler T, Spoerl E, Huhle M, Kamouna A. Conservative therapy of keratoconus by enhancement of collagen cross-links. Invest Ophthalmol Vis Sci. 1996;37:S1017.
5. Tamayo GE. Predictable visual outcomes with accelerated corneal cross-linking concurrent with laser in situ keratomileusis. J Cataract Refract Surg. 2012;38(12):2206.
6. Nguyen MK, Chuck RS. Corneal collagen cross-linking in the stabilization of PRK, LASIK, thermal keratoplasty, and orthokeratology. Curr Opin Ophthalmol. 2013;24(4):291-295.
7. Jaycock DP, O’Brart DP, Rajan MS, Marshall J. 5-year follow-up of LASIK for hyperopia. Ophthalmology. 2005;112(2):191-199.
8. Kanellopoulos AJ, Kahn J. Topography-guided hyperopic LASIK with and without high irradiance collagen cross-linking: initial comparative clinical findings in a contralateral eye study of 34 consecutive patients. J Refract Surg. 2012;28(11 Suppl):S837-S840.
9. Kanellopoulos AJ. Long-term safety and efficacy follow-up of prophylactic higher fluence collagen cross-linking in high myopic laser-assisted in situ keratomileusis. Clin Ophthalmol. 2012;6:1125-1130.
10. Li N, Peng XJ, Fan ZJ. Progress of corneal collagen cross-linking combined with refractive surgery. Int J Ophthalmol. 2014;7(1):157-162.
Gustavo E. Tamayo, MD
• Director, Bogotá Laser Refractive Institute, Bogotá, Colombia
• gtvotmy@telecorp.net
• Financial disclosure: Medical Advisory Board Member, Lecture fees (Avedro), Board of Advisors (Abbott Medical Optics)
