


To become a medical doctor in the United States, one must complete 4 years of college, 4 years of medical school, 1 year of internship, and 3 years of residency. To complete an ophthalmology residency, one must meet a set of core competencies, both medical and surgical. Is that enough to go out and practice? Perhaps for some, but I suspect that they are the minority. What about the rest of us?
I challenge you to find a residency that provides comprehensive education on coding, practice development, patient experience, the Merit-based Incentive Payment System, leadership, staff management, and industry relationships. It’s true that, if one joins a multispecialty practice with well-established referral patterns, coders, and office managers after training, these areas are less important to master. However, at least 60% of ophthalmologists work in smaller private practices with one to three providers, which means new associates must learn these skills on the job—and fast!
New associates realize early on that medicine is the easy part; it’s everything else that is challenging. I propose that we can, and should, educate the next generation of ophthalmologists on the business of medicine while also providing the medical and surgical core competencies.
MY FELLOWSHIP EXPERIENCE
As I was completing my residency, I realized that I wanted to gain additional surgical experience in the anterior segment. I applied to both academic and private practice cornea fellowships, but I quickly noticed that the private practice fellowships offered a few perks that academia did not, specifically regarding the business of medicine. I was fortunate enough to match at Vance Thompson Vision, where I now spend my days operating alongside, and picking the brains of, John P. Berdahl, MD, and Vance Thompson, MD, FACS.
Business acumen. I spend around 75% of my fellowship in the clinic or OR, and the other 25% is devoted to learning about practice development, industry relationships, research, leadership, and practice management. In addition to learning from the doctors, I meet monthly with Matt Jensen, CEO of Vance Thompson Vision, and regularly learn from the marketing and coding teams, business office, and practice managers. In July, when I move back to Philadelphia to join Chester County Eye Care, I will be fully armed with at least the basics of the business of ophthalmology.
Mentorship. Mentorship is essential in the business of ophthalmology, but not everyone is fortunate to have the opportunity to complete a private practice fellowship that provides these built-in relationships. New ways of obtaining mentorship are emerging to meet this need, including platforms such as YoungMD Connect (Bryn Mawr Communications), which I have found highly valuable. Through YoungMD Connect, young ophthalmologists can participate in weekly mentoring sessions with thought leaders in the field and full workshops focused on topics such as the pathway to the podium and global ophthalmology. In my experience, these mentorship sessions invariably end up covering intangible things such as industry relationships and building a reputation in the field—skills not acquired in residency.
CONCLUSION
Currently, access to the nonclinical side of ophthalmology is dependent on individual interest and motivation. Educating the future generation of ophthalmologists more equitably will require buy-in from residency program directors. It is even conceivable that residency programs could integrate the offerings of platforms like YoungMD Connect into their core curriculum. A formal course on the business of ophthalmology through a platform such as this would be invaluable.
As demand grows, I hope that private practice fellowships and platforms such as YoungMD Connect authentically fill this niche for generations to come. For anyone else interested in helping to make this future a reality, let’s connect, collaborate, and educate!


Educating the next generation of ophthalmologists has always been at the core of our mission. At Ospedali Privati Forlì “Villa Igea,” everyone shares a deep passion for teaching residents, fellows, and doctors to become excellent physicians, researchers, and leaders in the field of ophthalmology. We view mentorship as a team effort and recognize that each person brings a unique perspective and skillset. By developing a strong mentorship pipeline within our organization, we continuously transform mentees into mentors and facilitate the passing of the baton from peer to peer. This empowers everyone to maximize their own contribution to the shared success of the team.
PROVIDING A RICH EDUCATIONAL EXPERIENCE
Ospedali Privati Forlì “Villa Igea” is home to Italy’s leading corneal transplant center. We evaluate thousands of potential transplant candidates and perform more than 500 corneal transplants annually. A strong emphasis is placed on high-quality clinical and surgical care.
Given the constantly changing global landscape and the rapid expansion of basic and clinical knowledge in ophthalmology, direct patient interaction is more critical now than ever. Cornea fellowship training at a high-volume tertiary referral center offers an incomparable opportunity to build professionalism and develop the skills necessary to manage all forms of corneal disease with reasonable certainty and consistency. Completing a formal training program is absolutely necessary to achieve the required competency to perform all types of corneal surgery independently, including ultrathin Descemet stripping automated endothelial keratoplasty, Descemet membrane endothelial keratoplasty, deep anterior lamellar keratoplasty, and penetrating keratoplasty.
The era of lamellar corneal surgery has raised the standard of care. Disastrous complications have become exceedingly rare, however, they are not impossible. The ability to maintain equanimity in the face of complications is acquired only through experience. Mastery of all procedures is essential to achieving consistent and optimal outcomes regardless of the circumstance. In order to meet patients’ ever-increasing expectations, surgical decision-making must be informed by a pragmatic and prudent determination of the best procedure for each patient by the right surgeon.1 Thus, we ensure that every fellow is equipped with all the valuable tools in the surgical armamentarium of a true corneal specialist.
FOSTERING A CULTURE OF CONTINUOUS LEARNING
To encourage scientific discovery and lateral thinking, we have established an internal research arm, Istituto Internazionale di Ricerca e Formazione in Oftalmologia, where young investigators engage in collaborative research and cutting-edge innovation projects. We actively disseminate our research on various surgical techniques both locally and internationally through scientific conferences and remote training sessions with live surgery demonstrations. Through our international alumni network of clinical fellows, we maintain professional relationships and foster lifelong learning and career development.
Although we are committed to the highest standards of patient safety and care, our model of training has remained simple and intuitive—see one, do one, teach one.
1. Busin M, Yu AC. The ongoing debate: Descemet membrane endothelial keratoplasty versus ultrathin Descemet stripping automated endothelial keratoplasty. Ophthalmology. 2020;127(9):1160-1161.




Kensington Eye Institute, a partner of the University of Toronto’s Department of Ophthalmology and Vision Sciences, conducts about 25,000 patient visits and performs about 15,000 cataract and subspecialty surgical procedures each year. Training the next generation of Canadian ophthalmologists is a huge part of our mission as a teaching hospital. Each year, we train 12 surgical residents (six fourth-year and six fifth-year) using competency-based medical education. In our experience, a program of this design produces the best opportunity for residents to gain a high level of surgical skill as well as hands-on familiarity with advanced technologies.
STAGED LEARNING
We follow a staged learning approach. Residents progress through five clearly defined stages of competency that are composed of 20 cataract surgery days in the OR each, and the level of surgical difficulty progresses within these stages.
Residents are evaluated daily throughout the surgical phase of their training. Our evaluation system is based on the principles of the global movement known as competency-based medical education. Each distinct stage of training includes clear learning objectives, documented observation, and committee review. At the M1 level, residents perform simple aspects of routine cases. At the M2 level, they perform most parts of the case, including incisions, IOL insertion, OVD removal, and wound hydration. Intermediate steps include hydrodissection and irrigation and aspiration of cortex. By M3, residents are able to complete full cases, including phacoemulsification and capsulorhexis, which require more skill to master (Figure 1).
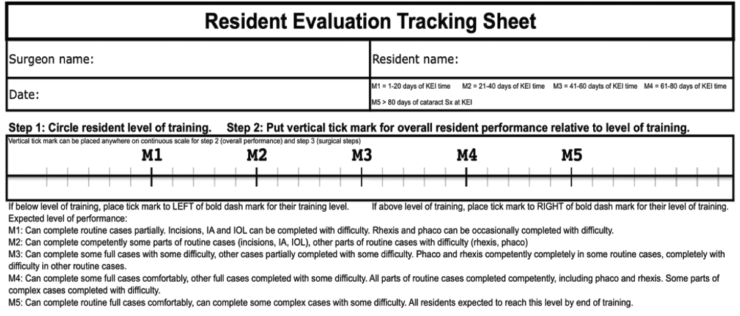
Figure 1. The resident evaluation tracking sheet is used to rate residents’ competency levels and track the number of cataract cases performed during each series of 20 OR days.
Figures 1 and 2 and the Figure in the sidebar courtesy of David B. Yan, MD, FRCS(C)
At each level, residents receive a numeric score with the minimum competency corresponding to their M level. For M1, the minimum expected score is 1.0, M2 is 2.0, M3 is 3.0, etc. The numeric value assigned to each tick mark is 0.2. A score of 2 marks to the right of the M2 marker is equivalent to a gross score of 2.4. At each M level, residents’ competencies are expected to be well above the minimum, which encourages positive feedback in the evaluation process.
DATA ANALYSIS
We adopted this competency by design system in 2013. Since then, we have statistically analyzed data covering six cohorts (35 graduating residents) to develop reliable confidence intervals of expected resident performance (Figure 2).
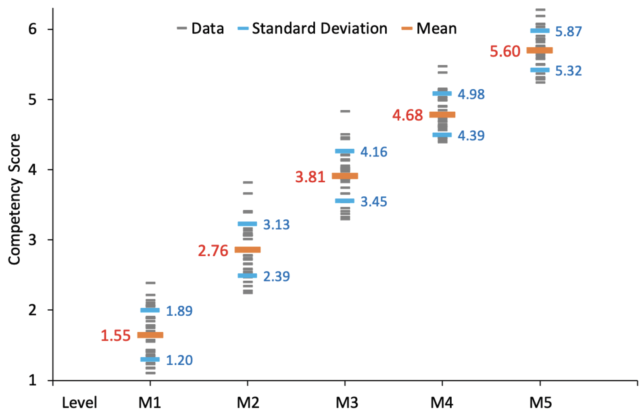
Figure 2. Competency scores for all residents over a 6-year period were tracked through each stage of residency. Residents who fall more than 1 standard deviation below the mean may be identified for remediation to ensure they achieve the desired level of competency.
Remediation plans. A resident whose score is close to the minimum of 2.0 for M2 (eg, 2.1) may be identified as needing remediation. A remediation plan doesn’t mean the resident is failing but rather that we want to help them catch up. The remediation plan may include more wet lab and OR time and/or directed time with faculty known to be the most effective at teaching trainees who are struggling with earlier stages of competency (see Wet Lab Training). Most importantly, we can avoid realizing only near the end of a student’s residency that they haven’t mastered cataract surgery. In our experience, residents who struggle during the M1 stage can often catch up without remediation, but residents who continue to fall behind by the end of M2 require some degree of extra attention to get back on course.
WET LAB TRAINING
The ophthalmic industry plays a role in Kensington Eye Institute’s residency program by providing the technology that residents need to learn to achieve competency and be prepared for clinical practice. Third-year residents spend a lot of their time learning how to use the equipment in wet labs and practicing with model and eye bank eyes so that they can learn the fundamentals of surgery before operating on patients. The surgical wet lab facility (Figure) is a valuable tool for surgical remediation when residents fall behind in training evaluations.
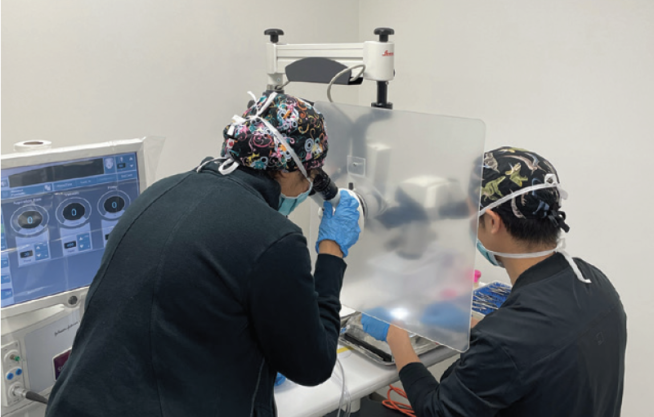
Figure. Nupura Bakshi, MD, FRCS(C), the director of surgical teaching (left), instructs a senior resident (right) on phacoemulsification during the COVID-19 pandemic. Through generous donations from industry sponsors, the number of wet lab stations was doubled to increase teaching opportunities while elective surgery was paused.
The same evaluation system is also used to track the cumulative number of cases completed by residents after each stage of training. There is a strong correlation between the number of cases completed by residents and their average evaluations.
The guiding principle behind the entire system is that competency doesn’t just happen—it must be monitored, benchmarked, and incentivized.
FACULTY EVALUATIONS
We track how many cases each surgeon shares with residents closely. Resident teaching reduces surgeon productivity, so the teaching load must be shared among all 40 of our cataract teachers fairly and equitably. The number of cases with resident participation is tracked for every case, resident, and teacher. A benchmark is set for the minimum percentage of cases teachers are expected to share with a resident at each level of training, starting at 10% for M1 and increasing linearly to 30% at the M5 stage.
When teacher tracking began in 2013, about 50% of teachers reached their minimum teaching target. Two years later, 100% were above their minimum target, and the proportion of cases shared by surgeons had grown by 80%. During that period, OR days for surgeons who didn’t hit their benchmark teaching target were reduced. This mandate has led to the resignations of a few surgeons who gradually lost OR time for refusing to teach, but it has ensured that the burden of training new surgeons is shared by all fairly. Equity in teaching has incentivized all surgeons at our academic center to fully embrace resident education.
An Equitable Pivot
The combination of rigorous monitoring, evaluation, and benchmarking and the utilization of a wide variety of advanced technology has helped Kensington Eye Institute and the University of Toronto graduate surgeons who are well prepared to treat patients. We have found that it ensures equity and fairness in the allocation of cases and residents’ progress toward graduation. A more ambitious or aggressive resident doesn’t get more OR time just because they push for it. Nor does a struggling resident get fewer cases—quite the opposite. Based on the evaluations and numbers of cases completed, we can deftly adjust resident OR schedules as needs are identified. It’s important to us that every resident has the opportunity to master cataract surgery (and other procedures) and be excellent surgeons when they leave us. This evaluation system has also been able to demonstrate gender equity in training among the cohort of 35 residents who have completed training since the inception of the program (19 female and 16 male residents).
Never has the value of this process been clearer than during the COVID-19 pandemic. All of our residents experienced a 3-month interruption in their training, which means they could have been in jeopardy of not completing residency on time for not achieving acceptable levels of surgical competency. Because we had tracked skills and case volumes so tightly, however, we were able to reconfigure OR schedules and ensure that every resident reached the M5 level. In fact, all of them performed the same number of cases (or more) as residents in previous, non–COVID-19 years.
At the time of this writing, the pandemic has been—and continues to be—a profound challenge, but it is one that our competency-by-design program has proven more than capable of handling.
