



Visualization of the posterior capsule is difficult during cataract surgery on eyes with asteroid hyalosis (AH) because of the increased translucence and decreased foldability of the capsule (Figure 1). The anterior capsulorhexis is also intrinsically different in these eyes because the anterior capsule is more brittle than usual. Although the preoperative appearance of the anterior capsule is typical in AH eyes, its postoperative appearance is qualitatively different at the slit lamp.
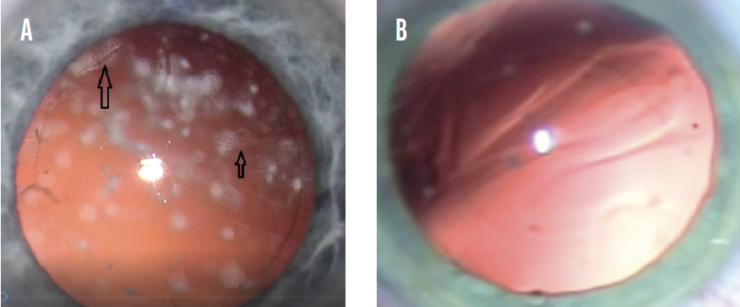
Figure 1. Cataract surgery on an eye with AH. Areas of the anterior and posterior capsules have an ethereal, frosted appearance (A). A normal eye with posterior capsular folds not observed in AH eyes (B).
This article discusses ultrastructural differences we have identified in anterior capsule samples obtained from normal and AH eyes and the practical implications of these differences.
BACKGROUND
In the Beaver Dam Eye Study, AH was present in 1.2% of the population, and its incidence increased with age.1 AH is primarily unilateral, and its prevalence is higher in men. The association of AH with diabetes is controversial. Some investigators have found a positive association, whereas others have found none.2,3
OCT is the preferred method of retinal imaging in advanced cases where fundal visibility is reduced.4 The asteroid bodies, which contain calcium and phosphorus,5 may impede the A-scan determination of axial length.6
Silicone IOLs are known to opacify in AH eyes7 and are wtherefore contraindicated.
STUDY METHODS AND RESULTS
Methods. Anterior capsule specimens were obtained from patients with AH and healthy patients who served as controls. Examinations were carried out using electron microscopy in two separate phases because of refurbishments to the department. A total of five normal and nine AH specimens were obtained.
Results. The normal human lens capsule is formed by layers of basal lamina composed of collagen type IV secreted by the lens epithelial cells.8 The capsule is the only basement membrane that is formed continually throughout life9 Its external surface is composed of fibrils similar to those of the zonules.10
In the first phase at magnifications ranging from 500x to 1,000x, the AH specimens showed a banded phenotype appearance not observed in the normal specimens. In the second phase, there was a reversal of this banded appearance between the two groups (Figure 2). This may be explained by some difference in staining technique and the model of microscope used. At high magnification (15,000x), some difference was again observed between the two groups; the AH specimens exhibited a less directional arrangement of microfibrils (Figure 3).
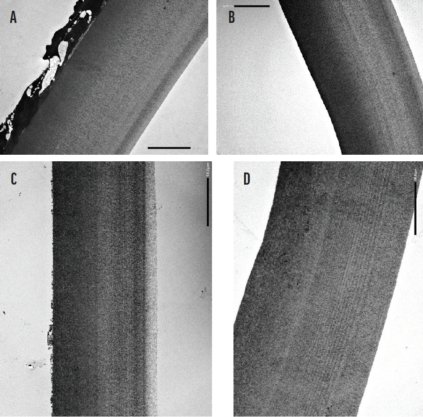
Figure 2. A composite image of 1,000x magnification (bar, 10 μm) with the anterior surface to the right of the image (phase 2). AH samples have a more uniform phenotype on transmission electron microscopy (A and B). Normal samples exhibit a more banded phenotype within the deeper structure (C and D).
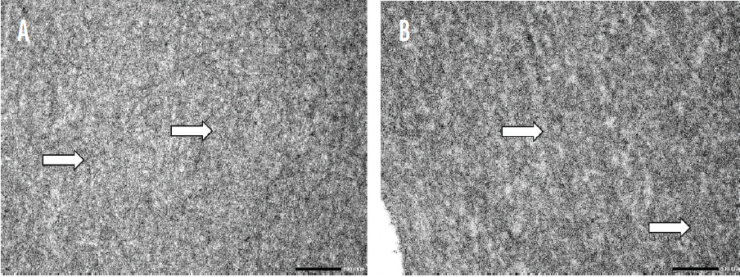
Figure 3. A composite image of high-magnification (15,000x; bars, 0.5 μm) appearances on transmission electron microscopy. An AH sample appears to be uniform with a microfibrillar nondirectional arrangement (arrows, A). A normal sample has a less uniform and somewhat dappled appearance with a tendency for the microfibrillar structure to be more linear (arrows, B).
Scanning electron microscopy of the anterior capsular surface revealed more pronounced features in the AH specimens (Figure 4). No significant difference in the thickness of capsule specimens was observed between the groups.
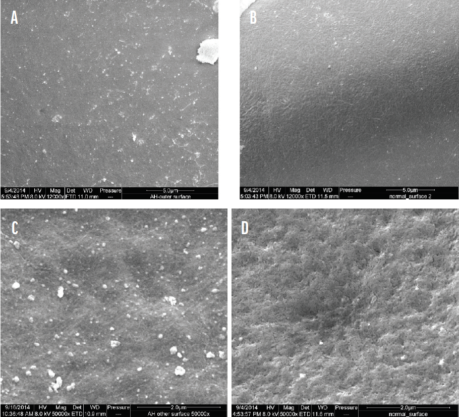
Figure 4. A composite image of 12,000x magnification (bars, 5 μm) of anterior surfaces on scanning electron microscopy. A relatively featureless surface in an AH eye (A). A normal anterior surface with a more distinct fibrillar pattern (B). At 50,000x magnification (bars, 2 μm), the outer surfaces of the AH (C) and normal (D) samples appear to be smooth and rough, respectively.
ASSOCIATIONS
Polychromasia capsulare. First described in 1969,11 this rare, benign, autosomal dominant ocular condition is not associated with other ocular findings or systemic abnormalities.12 The iridescent colors seen at the slit lamp are associated with an abnormal ultrastructural regular pattern at high magnification.13 This association may bear some relation to our findings in AH: Light interacts differently with the lens capsule where ultrastructural changes are found.
Other conditions associated with capsular anomalies. Pseudoexfoliation, originally thought to be limited to the lens capsule,14 is a more widespread condition both within the eye15 and systemically.16 Other conditions with recognized anomalies of the anterior lens capsule are Marfan syndrome,17 Peters plus syndrome,18 and Alport syndrome.19 Ultrastructural changes have also been noted in the capsules of eyes that develop cataracts secondary to uveitis.20
SIX REASONS TO TAKE EXTRA CARE WITH CATARACT SURGERY IN EYES WITH AH
No. 1: A-scan errors may be caused by asteroid body interference.
No. 2: Silicone IOLs are contraindicated in eyes with asteroid hyalosis.
No. 3: The anterior capsule may be more brittle than usual.
No. 4: The posterior capsule is more translucent and less liable to show folds than usual.
No. 5: These properties are independent of the number of asteroid bodies.
No. 6: Asteroid hyalosis of any degree represents an increased risk for cataract surgery.
CONCLUSION
Our findings suggest that AH involves the lens capsule, adding to its known ocular manifestations. AH is usually a unilateral condition and is not known to be hereditary. Nor is it known to have systemic implications.
The difficulty of cataract surgery on eyes with dense AH has been described (see Six Reasons to Take Extra Care With Cataract Surgery in Eyes With AH).21 The use of trypan blue dye to increase visibility of the posterior capsule in eyes with extensive AH is recommended.22 The asteroid bodies may compromise visualization of the posterior capsule during cataract surgery, but our research suggests that the capsule itself is more translucent as a consequence of ultrastructural changes in AH and less discernible as a result.
On a practical level, AH of any degree should be recognized as likely to increase the risk of complications during cataract surgery, and the condition should be incorporated into preoperative risk grading systems.23
1. Moss SE, Klein R, Klein BE. Asteroid hyalosis in a population: the Beaver Dam Eye Study. Am J Ophthalmol. 2001;132(1):70-75.
2. Yazar Z, Hanioglu S, Karakoç G, Gürsel E. Asteroid hyalosis. Eur J Ophthalmol. 2001;11(1):57-61.
3. Fawzi AA, Vo B, Kriwanek R, et al. Asteroid hyalosis in an autopsy population: the University of California at Los Angeles (UCLA) experience. Arch Ophthalmol. 2005;123(4):486-490.
4. Hwang JC, Barile GR, Schiff WM, et al. Optical coherence tomography in asteroid hyalosis. Retina. 2006;26(6):661-665.
5. Kador PF, Wyman M. Asteroid hyalosis: pathogenesis and prospects for prevention. Eye. 2008;22(10):1278-1285.
6. Wong SCK, Sampath R. Erroneous automated refraction in a case of asteroid hyalosis. J Cataract Refract Surg. 2002;28(9):1707-1708.
7. Espandar L, Mukherjee N, Werner L, Mamalis N, Kim T. Diagnosis and management of opacified silicone intraocular lenses in patients with asteroid hyalosis. J Cataract Refract Surg. 2015;41(1):222-225.
8. Danysh BP, Duncan MK. The lens capsule. Exp Eye Res. 2009;88(2):151-164.
9. Alio JL, Anania A, Sagnelli P. Age-related changes in crystalline lens. In: Cavalloti CAP, Cerulli L, eds. Age-Related Changes of the Human Eye. Humana Press; 2008:61-131.
10. Cohen AI. The electron microscopy of the normal human lens. Invest Ophthalmol. 1965:433-446.
11. Knox D, Wolfe RL, Murdoch JL, Gragg WG, Pfaffenbach DD. Hereditary tinted lenses in two families. In: Birth Defects Original Article Series. vol V, No. 2. Allan R. Lis; 1969:1661.
12. Traboulsi EI, Chung D, Koors JM. Polychromasia capsulare (multicolored capsule): report of three families. Trans Am Ophthalmol Soc. 2005;103:93-97.
13. Osher RH, Miller VJ, Eagle RC Jr, Siegman MJ, Wang D, Osborn DA. Polychromasia capsulare: determining the cause of multicolored iridescence of the anterior lens capsule. J Cataract Refract Surg. 2016;42(4):631-634.
14. Ashton N, Shakib M, Collyer R, Blach R. Electron microscopic study of pseudo-exfoliation of the lens capsule. I. Lens capsule and zonular fibres. Invest Ophthalmol. 1965;4:141-153.
15. Conway RM, Schlötzer-Schrehardt U, Küchle M, Naumann GO. Pseudoexfoliation syndrome: pathological manifestations of relevance to intraocular surgery. Clin Exp Ophthalmol. 2004;32(2):199-210.
16. Schlotzer-Schrehardt UM, Koca MR, Naumann GOH, Volkholz H. Pseudoexfoliation syndrome. Ocular manifestation of a systemic disorder? Arch Ophthalmol. 1992;110(12):1752-1756.
17. Traboulsi EI, Whittum-Hudson JA, Mir SH, Maumenee IH. Microfibril abnormalities of the lens capsule in patients with Marfan syndrome and ectopia lentis. Ophthalmic Genet. 2000;21(1):9-15.
18. Hwang DK, Yang AH, Yen MY, Wang AG. Ultrastructure of anterior lens capsule in Peters’ plus syndrome. Eye (Lond). 2007;21(6):862-864.
19. Choi Jh, Na Ks, Bae Sh, Roh Gh. Anterior lens capsule abnormalities in Alport syndrome. Korean J Ophthalmol. 2005;19(1):84-89.
20. Stunf S, Hvala A, Vidovič Valentinčič N, Kraut A, Hawlina M. Ultrastructure of the anterior lens capsule and epithelium in cataracts associated with uveitis. Ophthalmic Res. 2012;48(1):12-
21. Fishkind WJ, Crandall AS, Davison JA. The torn posterior capsule: prevention, recognition and management. Focal Points. 1999;17(4):1-13.
22. Friedman N. Pearls for using trypan blue. Ophthalmology Web. March 13, 2012. Accessed May 21, 2021. https://www.ophthalmologyweb.com/Tech-Spotlights/38928-Pearls-for-Using-Trypan-Blue
23. Galan A, Tavolato M, Babighian S. Grading the surgical difficulty of cataract phacoemulsification. Ophthalmic Surg Lasers Imaging. 2009;40(4):361-365.
