
Cataract development after vitrectomy is highly likely within a year of surgery. The type of cataract is generally nuclear. Despite the fact that the nucleus itself may not be particularly challenging, the rate of complications in vitrectomized eyes is reported to be significantly higher than the norm.1
Removal of the vitreous and, in some cases, injection of silicone oil into the vitreous cavity can have a profound effect on subsequent cataract surgery. Consideration must be given not only to the actual performance of the surgery but also to its planning, from biometry and decisions about incision configuration and IOL design to the best type of anesthesia to use. This article highlights the important considerations involved in performing cataract surgery in an eye after vitrectomy.
PREOPERATIVE considerations
Certain decisions must be made before surgery, generally related to biometry and IOL choice. A careful history of the reasons for vitrectomy and what took place at surgery is essential. If silicone oil was used, this can influence ultrasound biometry results, as sound travels at a different speed in oil than in the vitreous gel; optical biometry should overcome this issue. Another consideration in an eye with silicone oil present is that some of the oil may have migrated to the anterior chamber, and this probably has to be removed at the time of cataract surgery.
Once biometry has been performed, the surgeon's attention should turn to the choice of IOL. If the eye is very myopic, a three-piece lens with stiff haptics is useful to help stabilize the capsular bag. Implantation of a capsular tension ring may be helpful also, particularly if a one-piece IOL is chosen.
Intraoperative considerations
Anesthesia. Although the surgeon's usual preference for anesthesia will suffice, there are certain things to bear in mind in a vitrectomized eye. First, many of these patients have long axial lengths, and peribulbar anesthesia injection is potentially a hazardous approach due to the risk of globe penetration. Topical or sub-Tenon anesthesia is a safer approach.
When topical anesthesia alone is used, be aware that sudden changes in anterior chamber depth can cause the patient discomfort or sharp pain. Even the use of 1% nonpreserved lidocaine during hydrodissection does not prevent this. A method to avoid the sudden deepening of the anterior chamber and the related patient discomfort is described below.
Incision position and size. Scleral rigidity is generally reduced in vitrectomized eyes because the globe is softer when the vitreous has been removed. Because of this, and also because this condition is often present in myopic eyes, the type and size of the cataract incision is important. Some surgeons prefer scleral incisions in highly myopic eyes, as the location is further posterior and, therefore, the phaco tip is angled less in these deep anterior chambers. Also, a scleral incision may close more easily without sutures than a corneal incision. The incision should not be too far corneal, as this may result in distortion of the cornea, impairing visibility during the surgery. Using a Kelman-style curved phaco tip can help to avoid steep angulation of the probe.
Matching instrumentation size to the phaco incision is important in order to avoid unnecessary leakage and anterior chamber instability. Microincision techniques are less likely to induce leakage and distortion than techniques using a larger incision.
AT A GLANCE
- A careful history of the reasons for vitrectomy and what took place at surgery is essential prior to the start of cataract surgery.
- When considering IOL choice in these eyes, remember that a three-piece lens with stiff haptics is a good option in very myopic eyes and a capsular tension ring can be helpful in eyes in which a one-piece IOL was chosen.
- The defining issue in removing a cataract from a previously vitrectomized eye is the potential for lens-iris– diaphragm retropulsion syndrome.
SURGERY
After the incisions have been constructed, the eye is filled with an ophthalmic viscosurgical device (OVD). It is easy to overfill the anterior chamber, as it deepens readily without the support of the vitreous. This can make performing the capsulorrhexis more difficult. It can also widely dilate the pupil, which leads many surgeons to adhere too closely to the pupillary margin and, thus, make the rhexis too large.
Steps in LIDRS Prevention
• Lower the irrigation bottle to 40 cm
•
Place the phaco needle and sleeve in the eye with irrigation off
•Place the second instrument in the sideport to allow easy
egress of fluid (A)
•Lift the iris opposite the sideport
•Press the footpedal to foot position 2 to allow the eye to fill
but also draw fluid out
•Return the irrigation bottle to its normal height (there will
be no or only minimal change in anterior chamber depth)
•Repeat the above steps for each anterior chamber reentry
(B); this is crucial, because LIDRS occurs not just when the eye
is entered with the phaco tip but also at the start of irrigation/
aspiration and when OVD is removed after lens implantation.
The defining issue in removing a cataract from a previously vitrectomized eye is the potential for lens-iris–diaphragm retropulsion syndrome (LIDRS), which, essentially, is posterior pupillary block in which the inrush of irrigation fluid pushes the iris backward against the underlying structures. LIDRS results in a sudden and profound deepening of the anterior chamber. This has a number of effects, of which the most immediate from the patient's point of view is discomfort, and, when topical anesthesia has been used, outright pain. It can also cause iris sphincter damage, as reported by Osher and colleagues.2 The second effect of LIDRS is the need to operate with a very deep anterior chamber and, thus, a steeply angled phaco tip. Anterior chamber stability in the presence of LIDRS is also often less than ideal. This combination of conditions is thought to lead to a higher incidence of posterior capsular rupture.
Various methods of minimizing LIDRS have been advocated, such as using a low bottle height. The best method to break the posterior pupillary block may be the one described Cionni and colleagues, who note that lifting the iris will alleviate the immediate situation.3
It is possible, however, to prevent LIDRS from occurring in the first place. Some have recommended using an iris hook placed through a sideport to lift the iris,4 but it seems wasteful to use a whole packet of hooks for this purpose. Others have suggested making iridotomies.5 I devised a modification of the Cionni technique that can be used prophylactically (see Steps in LIDRS Prevention).6

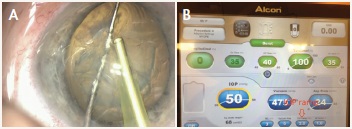
Figure 1. The Centurion machine has the ability to slow the ramp-up of IOP by up to 2 seconds.
On the Centurion Vision System phaco machine (Alcon), for which the irrigation cannot be lowered because it is inside the machine, a different approach is needed. Here, the machine has the ability to slow the ramp-up to the surgeon's chosen IOP by up to 2 seconds (Figure 1). This delay, combined with prophylactic lifting of the iris with the sideport instrument, is sufficient to stop LIDRS from occurring.
When LIDRS and posterior pupillary block are avoided, the surgery should proceed normally with no greater risk of complication than a standard case.
As mentioned above, vitrectomized eyes may contain silicone oil used as part of the initial vitreoretinal procedure. To prevent this from interfering with the surgical procedure, the oil can easily be sucked out using footpedal position 2 with the phaco probe.
CONCLUSION
With a little care and thought about biometry, IOLs, anesthesia, incisions, and capsulotomy, combined with maneuvers to avoid LIDRS, cataract surgery in postvitrectomy eyes can conclude with satisfactory outcomes. n
1. Biro Z, Kovacs B. Results of cataract surgery in previously vitrectomized eyes. J Cataract Refract Surg. 2002;28:1003-1006.
2. Osher RH, Osher JM, Cionni RJ. Multifocal iris sphincter ruptures: New sign of the lens–iris diaphragm retropulsion syndrome. J Cataract Refract Surg. 2010;36(1):170-172.
3. Cionni RJ, Barros MG, Osher RH. Management of lens-iris diaphragm retropulsion syndrome during phacoemulsification. J Cataract Refract Surg. 2004;30:953-956.
4. Vishwanath MR. Lens–iris diaphragm retropulsion syndrome and iris hooks. J Cataract Refract Surg. 2006;32(5):708.
5. Mendicute J, Bidaguren A. Lens–iris diaphragm retropulsion syndrome and iridotomies. J Cataract Refract Surg. 2007;33(2):177.
6. Packard RB. Avoiding lens-iris diaphragm retropulsion syndrome. J Cataract Refract Surg. 2010;36(7):1245.
Richard Packard, MD, DO, FRCS, FRCOphth
- Director of Arnott Eye Associates, London
- Practices at Prince Charles Eye Unit, King Edward VII Hospital, Windsor, United Kingdom
- mail@eyequack.vossnet.co.uk
- Financial disclosure: Consultant, Lecture Fees (Alcon)
