
Having the benefit of more than 20 years of follow-up, the safety and efficacy profile of modern-day refractive surgery is well established. Vision correction procedures such as LASIK and the implantation of phakic IOLs are now widely available for more patients. This is the case for patients with mild and moderate refractive disorders, and even those with more extreme amounts of ametropia.
Many surgeons believe that a refractive procedure specifically designed and indicated for the treatment of presbyopia is the final frontier in ophthalmology. One attractive approach is use of a corneal inlay. This device can be implanted in the nondominant eye to restore near visual acuity; the benefit of this technology is that it avoids the significant degradation in distance vision that can be seen with classic monovision techniques.
Several corneal inlay technologies are available internationally; however, because none are yet approved for use in the United States, my experience with one such device, the Raindrop Near Vision Inlay (ReVision Optics; Figure 1), has come as an investigator in the US clinical trials, which are nearing completion. I have treated more than 50 patients with the inlay (both phakic and pseudophakic), placing it in the nondominant eye under a corneal flap.
PROFOCAL MECHANISM OF ACTION
The Raindrop is designed to biomechanically raise the stroma anterior to the inlay. Epithelial remodeling over the inlay creates a profocal cornea; near refractive power is centered over the pupil, gradually transitioning to intermediate and distance vision toward the periphery.
To date, my use of the inlay has been dictated by the strict protocols of the FDA clinical trial. However, one of the attractive qualities of this and other corneal inlays is that they have the potential to be combined with LASIK and other refractive procedures to address preexisting refractive errors and presbyopia in a single surgical visit—as is already the case in Europe—and, perhaps, in conjunction with refractive cataract surgery.
COMBINATION PROCEDURES
The most common combination with corneal inlays to date has been placement under a stromal flap at the time of LASIK; however, other combined uses are possible, such as inlay implantation with a phakic IOL and with cataract surgery or refractive lens exchange.
Corneal inlay plus excimer laser. Presbyopic patients with any variety of refractive error may have the opportunity to undergo a LASIK treatment and have an inlay placed under the flap. This treatment has the potential to eliminate or reduce the need for all correction (even for near) postoperatively. For patients in their mid to late 30s, which is the age when many people commonly seek LASIK, we might have a discussion about inserting the inlay at the same time because we know that presbyopia is only a few years away. This would be one strategy to give patients the least need for glasses for the greatest length of time.
AT A GLANCE
- One of the attractive qualities of corneal inlays is that they can potentially be combined with other refractive procedures to address patients' existing refractive error at the same time as their presbyopia.
- Using a removable technology such as the Raindrop inlay allows surgeons to maintain maximum flexibility, without removing tissue that can never be put back.
In my experience with the Raindrop inlay, patients who are slightly hyperopic preoperatively seem to do best. Therefore, when the Raindrop is used concomitantly with LASIK—as has been the case internationally already—the recommended target for the ablation in the inlay eye is to leave the patient slightly hyperopic. This is likely counterintuitive for most refractive surgeons; normally, when we treat presbyopia with IOLs or other approaches, we think about leaving the nondominant eye a little myopic. It is important to remember this in surgical planning for the Raindrop inlay.
A Unique Appraoch to Near Vision
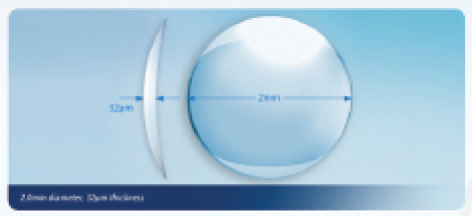
Figure 1. The Raindrop corneal inlay, 2 mm wide and 30 μm thick, creates a dedicated near vision zone in the central cornea. Placed in the nondominant eye, it provides functional reading vision for the patient. The inlay modifies the central corneal curvature in the implanted eye, resulting in a prolate shape that creates a multifocal optical system in the cornea and allows the patient to see both far and near in the operated eye.
Corneal inlay plus phakic IOL. Internationally, phakic IOLs such as the Visian ICL (STAAR Surgical) can be used to treat myopia and hyperopia, and the Toric ICL can be used for both myopic and hyperopic astigmatism. However, to date, a version that addresses presbyopia does not exist. Many patients have a strong affinity for removable and reversible technologies. Therefore, in the sense that they treat different problems but do not involve a permanent change to the cornea, phakic IOLs and corneal inlays have the potential to be complementary.
Corneal inlay plus cataract surgery or refractive lens exchange. I have performed cataract surgery in patients with a Raindrop corneal inlay, and I have found that these patients do well with implantation of a monofocal IOL and a target of emetropia. The multifocal optics of the inlay combine well with a monofocal implant, allowing these patients to have their uncorrected distance and near visual acuities restored.
PROMISING RESULTS
We are currently involved in the FDA clinical trial of the Raindrop inlay in patients who are already pseudophakic, and therefore only in need of reading glasses. To date, results are promising and consistent with what we have seen in phakic presbyopic emmetropes.
One 52-year-old patient who is enrolling in our clinical trial originally had presbyopia, myopia, and a significant amount of corneal astigmatism preoperatively. After discussing the options for treating both her refractive error and presbyopia, she opted to have a refractive lens exchange performed using a toric IOL, and then implantation of the Raindrop inlay subsequently to address her presbyopia.
Normally in her nondominant eye, I would have targeted slight myopia, but, knowing what we do about the Raindrop, I targeted slight hyperopia with the toric IOL (0.25 to 0.50 D). In her dominant eye, which had a similar preoperative refractive error, I performed myopic astigmatic LASIK for distance. The result was strong distance acuity in both eyes and good near vision in the nondominant eye with the inlay.
CONCLUSION
The availability of a corneal inlay opens many more possibilities for combinations of techniques and technologies. There are various ways we can mix and match to provide the best refractive surgery solution for each individual patient. By using a removable technology such as the Raindrop, we maintain maximum flexibility, without removing tissue. I look forward to being able to add the Raindrop to my armamentarium of refractive surgical procedures in the near future. n
Gregory D. Parkhurst, MD, FACS
- Cataract and Refractive Surgeon/Physician CEO, Parkhurst NuVision, San Antonio, Texas
- http://www.sanantonio-lasik.com
- gregory.parkhurst@gmail.com
- Financial disclosure: Consultant (ReVision Optics, STAAR Surgical, Alcon)
