

As a result of recent innovations, pediatric cataract surgery has become a highly sophisticated subspecialty in ophthalmology. The functional results after early surgical intervention are very promising today, but there still exist certain challenges and controversies in this important field.
AT A GLANCE
• Cataract surgery procedures, considerations, and risks differ in children and adults.
• Although there is general agreement on the timing of surgery, the decision whether to implant an IOL is still the subject of discussion.
Children with cataracts are not just small adults with cataracts. They present numerous problems and challenges that involve medical, social, and surgical issues. Procedures for cataract surgery and refractive correction in children have changed dramatically in recent years.
The implantation of an anterior chamber IOL in a child was first performed by Choyce in 1955. Several years later, Binkhorst implanted an iridocapsular-fixated IOL in another pediatric patient.
However, IOL implantation in children did not become common practice until the 1990s. Since that time, primary IOL implantation in young children is gaining popularity as surgical techniques have improved and biocompatible IOL materials and designs have become available. Despite these advances, some issues in pediatric cataract surgery are still under debate.
TIMING OF SURGERY
Early diagnosis and early surgical intervention are necessary in children with congenital cataracts. Especially in the case of unilateral cataracts, surgery should be performed within the first 6 weeks in order to prevent the development of severe amblyopia. In bilateral cases, it is advisable to perform surgery on both eyes at the same time to minimize the risk of repeated general anesthesia in this critical period of neurodevelopment. The incidence of secondary glaucoma is higher if surgery is performed early.
Children with partial cataracts treated conservatively must be followed closely. If the opacities are severe enough to obscure the fundus through an undilated pupil, amblyopia development can be expected. After surgery, prompt optical rehabilitation and treatment of amblyopia are mandatory.
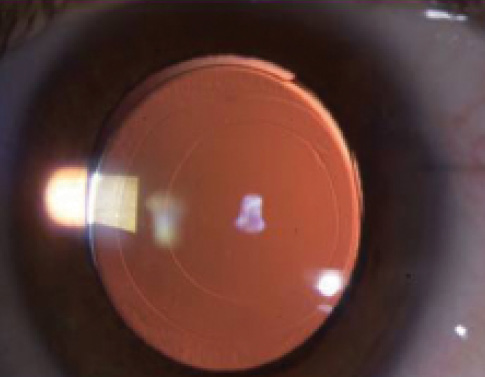
Figure 1. Anterior and posterior capsulorrhexis in a 1-year-old.
SURGICAL TECHNIQUE
Special surgical techniques, such as primary posterior capsulorrhexis (Figure 1), posterior optic capture, and anterior vitrectomy in children younger than 5 years help to prevent posterior capsular opacification (PCO). PCO after cataract surgery in children occurs with a much higher frequency than in adults.
Postoperative management of an opacified posterior capsule is usually difficult. Nd:YAG laser capsulotomy is often impossible due to the child’s inability to cooperate with the treatment. This often necessitates a return to the operating room for surgical posterior capsulotomy, which is an additional stressful situation during the highly sensitive period of visual development in younger children.
I prefer to use a transpupillary, limbal approach to cataract surgery in children. I dilate the pupil with a highly viscous OVD, perform the capsulorrhexis with forceps, aspirate the lens, and create a posterior capsulorrhexis. In children younger than 5 years, I then perform dry anterior vitrectomy.
If I do not implant an IOL, I enlarge the posterior opening in order to avoid capsular contraction syndrome. With this technique, secondary sulcus implantation of an IOL may be performed under controlled conditions in most cases, as the visibility of the rhexis margin is good.
If I do implant an IOL, I perform bag implantation with posterior optic capture. In complicated cases with fibrotic capsular alterations, it is necessary to cut parts of the lens capsule with scissors or with the vitrectome.
I routinely inject cefuroxime into the anterior chamber at the end of surgery, and for wound closure I use 10-0 resorbable sutures.
If IOL implantation is not planned, some surgeons still perform lensectomy via the pars plana. Femtosecond laser-assisted cataract surgery techniques have been applied in children, but I do not see any evident advantage for this in pediatric cases.
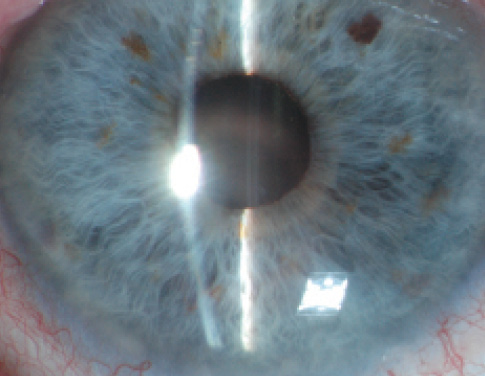
Figure 2. Supplementary IOL in a 3-year-old.
IOL IMPLANTATION
Although there is more or less a consensus regarding the timing of surgery in pediatric cataract, the best time for implantation of an IOL is still a subject of discussion. Some surgeons implant IOLs in the newborn, while others try to wait as long as possible to avoid large changes in refraction. The latter argue that contact lens correction, rather than early IOL implantation, gives maximum flexibility to adapt to the rapid changes in axial length that occur during infancy.
In the Infant Aphakia Treatment Study,1 a multicenter randomized trial comparing pediatric patients aged between 1 and 4.5 years undergoing cataract surgery with and without IOL implantation, visual acuity did not differ significantly between the two treatment groups. On the contrary, findings of a safety review showed higher rates of complications and additional intraocular surgeries in the IOL implantation group.
However, an individualized regimen that takes all factors into account would seem to be advantageous.
As the highest degree of eye growth is within the first year, I personally implant IOLs after 1 year of age in order to avoid a severe myopic shift and high reoperation rate. Even after meticulous surgery and sophisticated antiinflammatory treatment in these very small eyes, inflammation is usually prominent. Only in cases in which poor compliance with contact lens wear is anticipated do I make an exception to this rule.
The use of PMMA. For years, surgeons used rigid PMMA and heparin surface-modified PMMA IOLs in pediatric eyes. In recent years, the trend has been away from PMMA toward foldable materials for childhood IOL implantation. This move has been driven by the desire to employ proven biocompatible materials that can be inserted through a small incision, therefore causing less inflammation.
With the introduction of IOLs that incorporate a blue light filter, another interesting aspect has evolved for pediatric cataract patients. Even though it has not been demonstrated that a blue light filter helps to reduce age-related macular degeneration in older cataract patients, theoretically it could make sense to implant these IOLs in children because they need light protection for so many more years.
Dynamic refraction. The management of pediatric cataract is challenging because of the evolving refraction in children; I like to refer to it as their dynamic refraction. Although many surgeons rely on one of three standard treatments—glasses, contact lenses, or IOL implantation in the capsular bag—a new alternative is implanting a supplementary IOL designed for sulcus placement. By adding, removing, or exchanging a supplementary IOL, we can repeatedly correct the child’s dynamic refraction so that the eye can develop as it is supposed to.
Duet implantation. Implanting an additive lens at primary surgery (Figure 2) is part of what I have termed duet implantation.2 This approach combines in one procedure primary IOL implantation in the capsular bag and supplementary lens implantation in the sulcus. The advantage of this corrective strategy is that the supplementary IOL can be exchanged (refractive exchange of supplementary IOL) or explanted to compensate for the child’s changing refraction. Additionally, it allows the surgeon to aim for emmetropia or myopia instead of undercorrecting the eye.
RISKS
It should be mentioned that there are certain risks in cataract surgery in children compared with adults. First, the eye is smaller and may be more likely to develop a pupillary block syndrome. Therefore, a primary peripheral iridectomy should be performed in all these cases. Second, the child’s eye reacts with a higher degree of inflammation. Therefore, proper administration of antiinflammatory treatment is mandatory. I currently use this option only in children after 1 year of age.
CONCLUSION
Whether a pediatric cataract is present at birth or develops during the first few years of a child’s life, timely surgical intervention is needed to maximize visual development. Complete preoperative evaluation and visual rehabilitation, including patching therapy to prevent amblyopia and promote visual development, are essential components of intervention.
Pediatric cataract surgery is a very complex, demanding procedure. In order to achieve a favorable outcome for these young patients who clearly need their sight, specialized care is required from pediatric ophthalmologists, pediatricians, and skillful surgeons.
1. Infant Aphakia Treatment Study. ClinicalTrials.gov Identifier: NCT00212134. https://clinicaltrials.gov/ct2/show/NCT00212134. Accessed December 4, 2015.
2. Kahraman G, Amon M. Duet implantation: an update. CRST Europe. March 2011.
Michael Amon, MD
• Professor and Head of the Department of Ophthalmology, Academic Teaching Hospital of St. John, Vienna, Austria
• Member, CRST Europe Editorial Board
• amon@augenchirurg.com
• Financial disclosure: None
